

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
An estimated 86% Korean residents have availed some form of Traditional Korean Medicine (TKM) at least once in their lifetime, with maximum application of acupuncture [1]. In particular, bee venom acupuncture is a commonly practiced treatment for musculoskeletal and joint pain in TKM [2]. Although focal inflammation is a minor and temporary side effect of bee venom acupuncture [3], severe complications can arise when applied around or directly to a nerve. This case report is the first to describe severe ulnar nerve injury caused by bee venom acupuncture, performed at a TKM clinic.
CASE REPORT
In April 2015, a 52-year-old right-handed man visited our clinic presenting with a right claw hand, decreased sensation below the right elbow, and decreased motor strength in the 4th and 5th digits of the hand. Previously, the patient had pain in the right elbow, and had received more than 10 bee venom acupunctures on the medial side of the affected elbow and forearm, at a TKM clinic. Immediately after the procedure, he experienced severe pain and swelling of the right elbow. Although the pain subsided several days after the acupuncture, he had developed weakness of the right 4th and 5th finger flexors, and a sensory change on the ulnar dermatome of the right hand. When the patient was referred to our clinic 7 days after acupuncture, the strength of the 3rd and 4th lumbricals and interosseous muscles of the right hand were graded 1 out of 5 by a numeric rating scale.
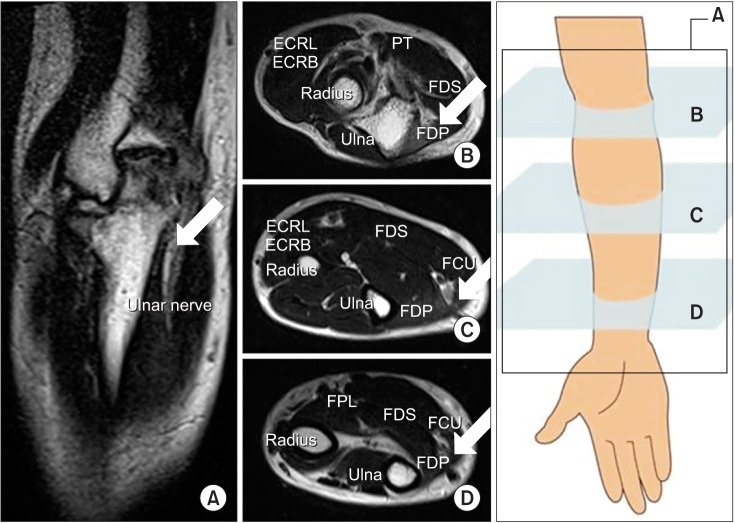
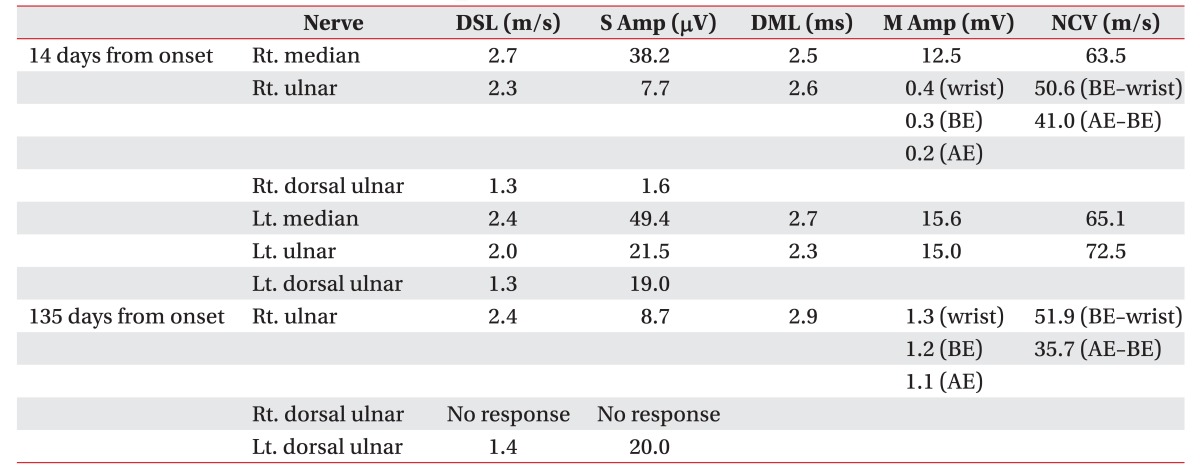
A right ulnar motor nerve conduction study 2 weeks after the injury, showed low amplitude of compound muscle action potentials and slow nerve conduction velocity at the elbow segments, indicating potential focal segmental demyelination, axonal damage, and Wallerian degeneration.
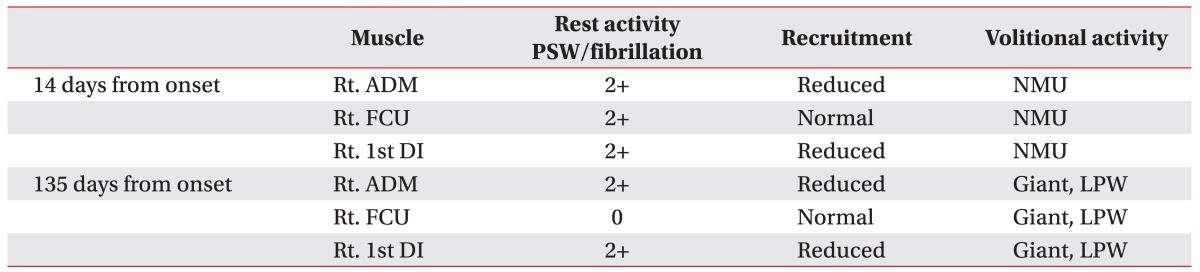
A right ulnar sensory nerve conduction study showed low amplitude of sensory nerve action potentials (SNAPs) (Table 1). Electromyography revealed abnormal spontaneous activity and a decreased interference pattern at the right abductor digiti minimi muscle and the first dorsal interosseous muscles, and abnormal spontaneous activity at the right flexor carpi ulnaris (Table 2). The patient underwent steroid pulse therapy for 4 weeks since his first visit, and also received electrical stimulation therapy at an outpatient clinic.
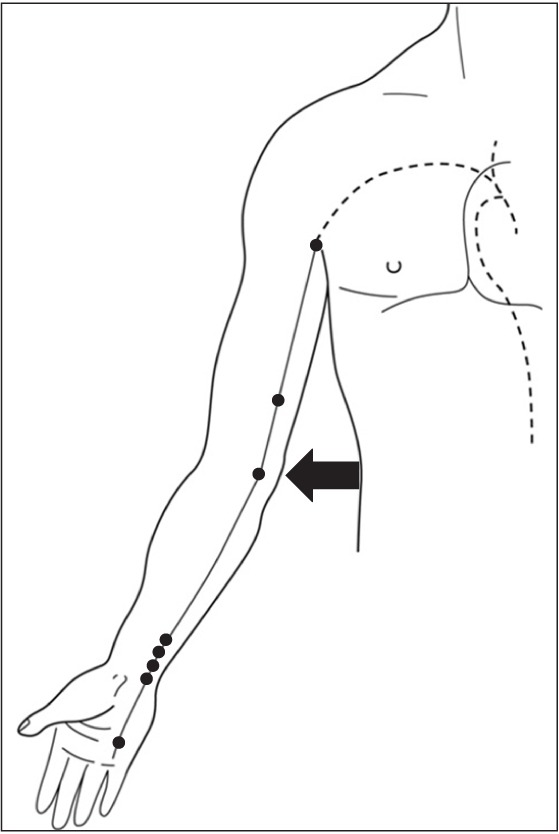
Magnetic resonance images of the right forearm, hand, and wrist were obtained 1 month after the injury. Swelling of the right ulnar nerve at the cubital tunnel was observed (Fig. 1). Ultrasonography showed diffuse right ulnar nerve swelling, and the cross-sectional area in transverse view at elbow level was 13 mm2. On the other hand, left side cross-sectional area was 8 mm2. There was subluxation of the right ulnar nerve escaping the cubital tunnel to the anterolateral area of the forearm during elbow flexion (Fig. 2). An electrodiagnostic study was conducted 4 months after the injury. There was decreased right ulnar motor conduction velocity at the elbow segment and no response of SNAP at the right dorsal ulnar nerve (Table 1). A giant and long duration polyphasic motor unit was found in the right forearm and hand muscles innervated by the ulnar nerve (Table 2). Thus, although there was evidence of regeneration of the denervated muscles, complete recovery was not indicated by the electrodiagnostic study (Table 1).
DISCUSSION
This case report highlights the concern regarding medical complications arising from TKM treatment. Acupuncture points most commonly used for elbow pain are located on the medial side of right elbow near the ulnar nerve course (arrow in Fig. 3) [4]. However, the patient showed subluxation of the ulnar nerve escaping the cubital tunnel to the anterolateral area of the forearm during elbow flexion (Fig. 2), which overlapped the course of the acupuncture points. This implies that the ulnar nerve injury was likely caused by focal inflammation or by direct injury of bee venom acupuncture around or direct to the ulnar nerve. Bee venom acupuncture is more dangerous than needle acupuncture if done around or directly to the nerve [5]; this observation is supported by the sustained nerve swelling in magnetic resonance imaging and ultrasonography 1 month after acupuncture in this case. Further studies are required to understand the neurotoxic effects of bee venom more exhaustively.
To avoid nerve damage, TKM practitioners should know the exact anatomical positions of the nerves. The physical examination and an electrodiagnostic study revealed the lack of a complete recovery from the ulnar nerve injury. Thus, the patient sustained poor performance of daily activities by severe dysfunction of his right hand.
Traditional medical practices are common. For example, the percentage of people who have used some form of traditional medicine is 68.9% in Australia, 90% in China, 86% in Korea, and 53% in Singapore [67]. However, there are few published reports relating to the adverse effects of TKM treatments [89]. This is the first report of ulnar nerve injury as a complication of bee venom acupuncture, and indicates the possibility of sustained complications from TKM procedures, which may be avoidable by the increased anatomical training of practitioners.

 XML Download
XML Download