

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiac rehabilitation (CR) is an interdisciplinary team approach to treat patients with functional limitations secondary to heart diseases [1]. The goal of this treatment is to help patients restore their optimal medical, physical, mental, psychological, social, emotional, sexual, vocational, and economic health, all of which are dependent on the severity of disease [1].
It has been reported that CR has beneficial effects [23]. In a meta-analysis for randomized controlled trials, it has been revealed that participation in exercise-based CR can improve both survival rate and risk factors associated with coronary artery disease [2]. An observational analysis of Medicare Beneficiaries in 1997 has also found a survival benefit associated with participation in CR among patients hospitalized for coronary conditions [3].
Until now, acute coronary syndrome (ACS) management has been focused on reducing mortality and morbidity without considering patient's health-related quality of life (HRQoL). Since the survival rate of ACS patients has increased, HRQoL has become a more important part of ACS management. Many studies have shown that health status, specifically the extent of angina symptoms, strongly predicts long-term clinical outcomes including quality of life of patients with coronary artery disease [456]. In one study, physical limitation has been found to be a significant and independent predictor of 1-year mortality, while angina frequency is a predictor of 1-year ACS readmission [5]. In another study, early primary coronary intervention has provided greater gains in HRQoL compared to conservative therapy mainly due to improvements in angina symptoms [6].
The evaluation of health status through the Medical Outcome Study 36-item Short-Form Health Survey (MOS SF-36) is an assessment tool frequently employed to evaluate HRQoL. MOS SF-36 is a standardized and validated instrument recommended by the American Association of Cardiovascular and Pulmonary Rehabilitation for evaluating HRQoL in patients with cardiovascular disorders [7].
Despite the benefits of CR in myocardial infarction and bypass surgery patients have been widely recognized, participation in and adherence to CR are less than optimal. Previous studies have reported that the rate of participation ranges from 29.5% to 55% in the United States [89]. In Japan, only 21% of those with acute myocardial infarction participated in CR [10]. In Australia, only 29% of those eligible for CR were referred and only one-third of those referred actually attended CR [11]. In Korea, studies on the adherence to or awareness of CR have been rarely reported. One study investigated the reasons why cardiac patients did not participate in CR programs or dropped out [12]. Therefore, the objective of this study was to determine the level of HRQoL, life satisfaction, and their present awareness of CR program in people with cardiovascular diseases.
MATERIALS AND METHODS
Subjects
We enrolled patients with cardiovascular diseases who were admitted to the Department of Cardiology and referred for CR. Patients treated between April 2011 and July 2011 were included. Inclusion criteria were: (1) a diagnosis of ACS and heart failure due to ACS, ST elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI), or unstable angina; (2) admitted in the Department of Cardiology; and (3) referred to the Department of Rehabilitation Medicine for CR. Exclusion criteria were: (1) uncontrolled arrhythmia; (2) peripheral arterial disease; and (3) psychological problems.
Methods
General characteristics
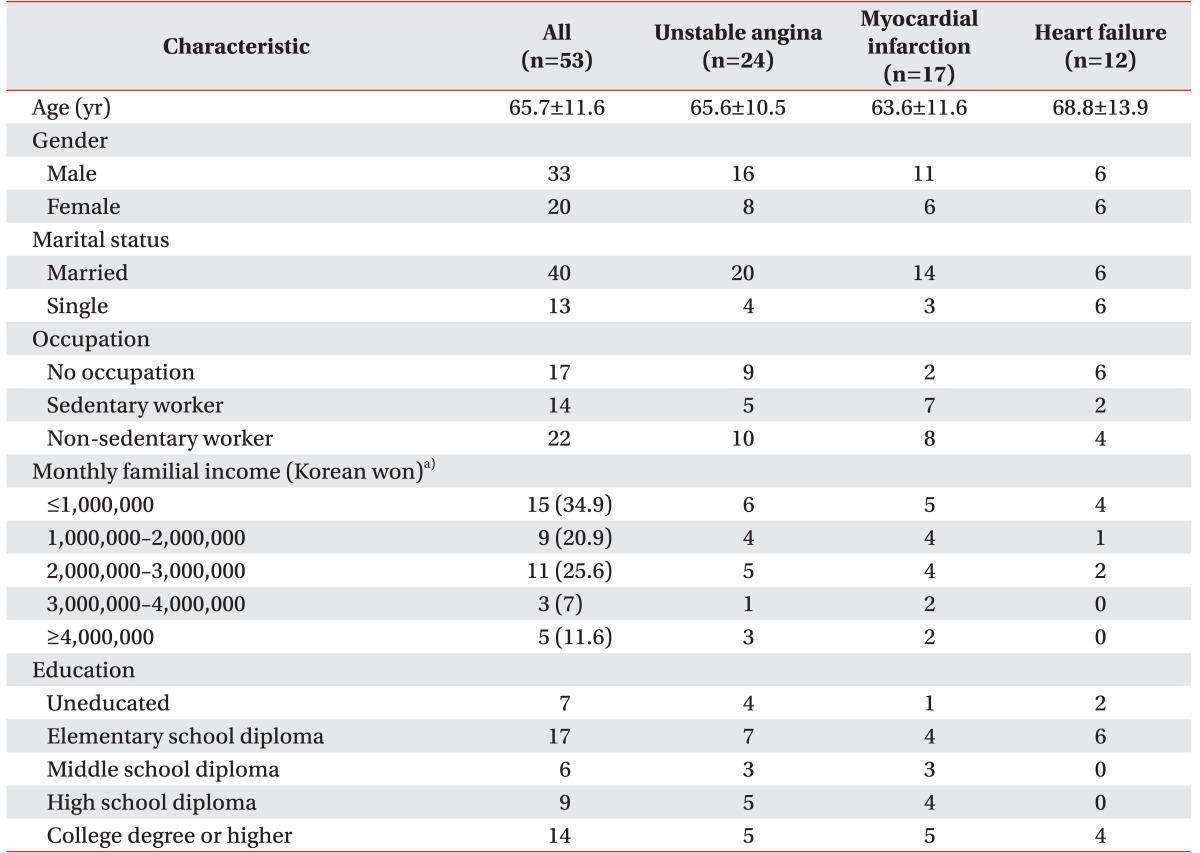
Socioeconomic and demographic characteristics including age, gender, marital status, occupation, familial income, and education were obtained. Marital status was coded as married or not married. Occupation was classified into 16 categories, including no occupation, simple laborer, service manager, technician, office worker, and housewife. In addition, occupational levels were grouped into three categories: no occupation, non-sedentary worker, and sedentary worker. Familial income was classified into five categories in 1 million Korean won increments from ≤1,000,000 to ≥4,000,000 Korean won per month. Education was measured in eight categories, ranging from uneducated to college degree or higher. Educational levels were also grouped into five categories, including uneducated, elementary school diploma, middle school diploma, high school diploma, and college degree or higher.
Before inclusion in the study, all patients were asked for informed consent and all agreed to participate.
Clinical characteristics
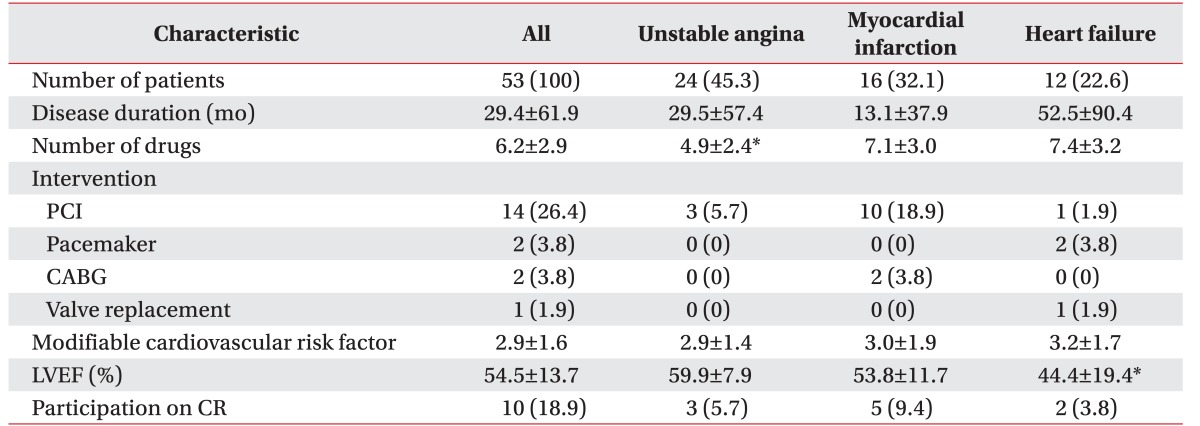
Disease status-related clinical variables included major diagnosis, duration, number of medications, type of intervention, the latest left ventricular ejection fraction, the number of modifiable cardiovascular risk factors (hypertension, diabetes mellitus, hyperlipidemia, obesity, smoking, exercise, drinking, stress level), and the degree of participation in the CR program. Clinical data were obtained from clinical records by a single investigator.
Health-related quality of life
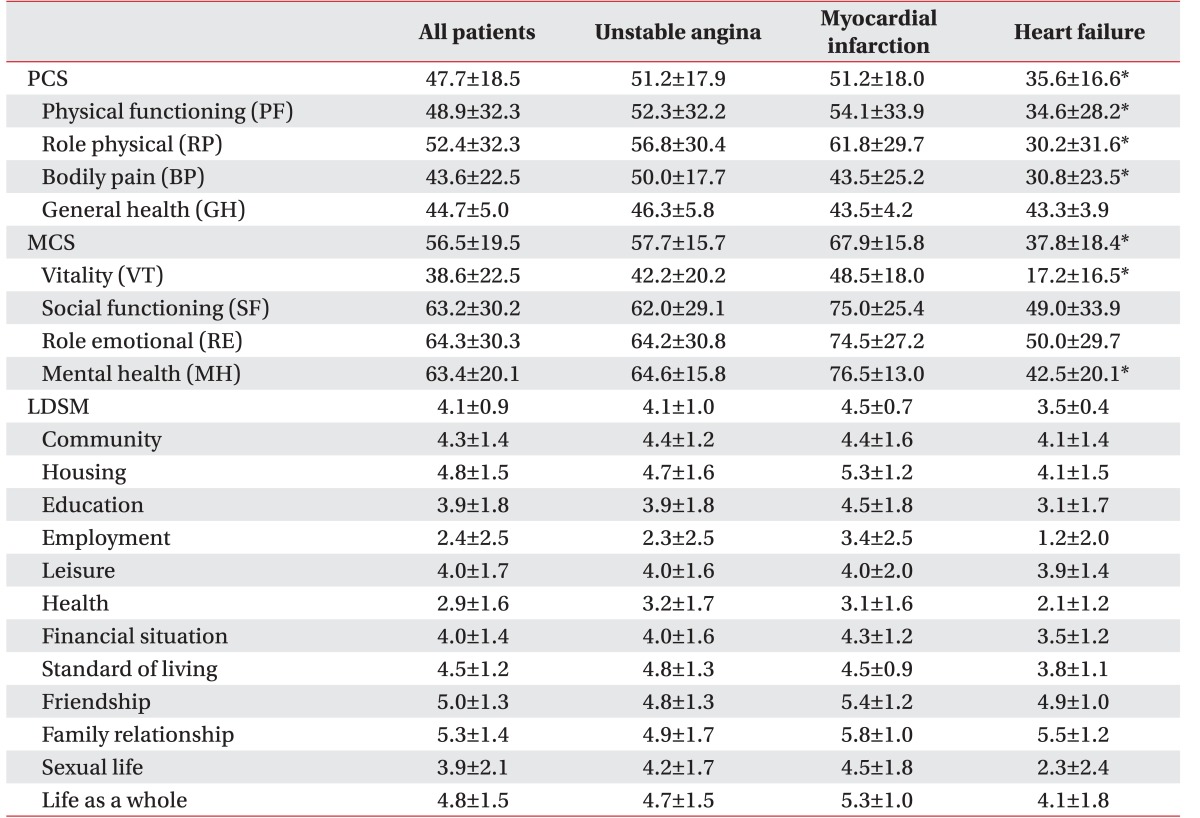
The HRQoL of patients with cardiovascular diseases was assessed with the MOS SF-36 method developed by Ware and Sherbourne [13] in 1992. This is a widely used measure for HRQoL. It has been extensively validated [1415]. The MOS SF-36 consisted of two categories: the physical component summary (PCS) and the mental component summary (MCS). It had eight subcategories. PCS included four subcategories, including physical functioning (PF), physical role (PR), bodily pain (BP), and general medical health (GH). MCS also included four subgroups: vitality (VT), social health (SH), role emotional (RE), and mental health (MH). The MOS SF-36 consisted of these eight subcategories with a total of 35 questions. It also included an additional question about health changes [13]. Summing the item scores from the same scale gave the scale scores in the range from 0 to 100, with higher scores indicating better quality of life [16]. The eight scale scores were aggregated into norm-based PCS and MCS scores with a population mean of 50 and a standard deviation of 10.
Life domain satisfaction measure
The life domain satisfaction measure (LDSM) [17] was used to assess life satisfaction. This measure contained 12 factors covering community, housing, education, employment, leisure, health, financial situation, standard of living, friendship, family relationship, sexual life, and life as a whole. Each question was rated on a 7-point Likert-type scale (from 1 ‘very dissatisfied’ to 7 ‘very satisfied’), with higher mean scores in each item indicating better satisfaction [17].
Statistical analysis
Statistical analyses were performed using PASW ver. 18.0 for Windows (SPSS Inc., Chicago, IL, USA). All calculated p-values were two-sided. Statistically significance was considered when p-value was less than 0.05. Categorical data are expressed as number (%). Continuous variables are expressed as mean±standard deviation. Mean scores from MOS SF-36 were compared among diagnoses using one-way analysis of variance (ANOVA) followed by post-hoc analyses. Pearson correlation analysis was performed to determine the association among socioeconomic, clinical status, and HRQoL factors.
RESULTS
Demographic and clinical characteristics
Of the 65 participants, 53 patients met the inclusion criteria, including 33 males and 20 females. Data of the 53 patients were analyzed. Their mean age was 65.7 years (range, 38–86 years) (Table 1). Most patients (75.5%) were married. Of the 53 patients, 17 (32.1%) had graduated from elementary school. Forty-three patients responded to questions about monthly family income—15 (34.9%) earned less than 1,000,000 Korean won, 9 (20.8%) earned 1,000,000–2,000,000 Korean won, 11 (25.6%) earned 2,000,000–3,000,000 Korean won, 3 (7%) earned 3,000,000–4,000,000 Korean won, and 5 (11.6%) earned more than 4,000,000 Korean won (Table 1). For occupation area, 45.5% were manual workers, 32.1% had no occupation, and 26.4% were sedentary workers (Table 1). There were no significant differences in socioeconomic characteristics among the three types of cardiovascular diseases. Twenty-four (45.3%), 16 (32.1%), and 12 (22.6%) patients were diagnosed with unstable angina (UA), myocardial infarction (MI), and heart failure (HF), respectively. The average duration of the disease was 29.4±61.9 months. The average number of drugs taken by patients was 6.2±2.9. The mean number of modifiable cardiovascular risk factors was 2.9±1.6. The mean LVEF was 54.5%±13.7% (Table 2). The number of drugs taken (F=4.560, p=0.015) and LVEF (F=4.550, p=0.017) were significantly different among the three types of cardiovascular diseases. Scheffe post-hoc analysis revealed that both drug number (p<0.05) and LVEF (p=0.022) were significantly different between the unstable angina group and the heart failure group.
Quality of life and life domain satisfaction measures
The average MOS SF-36 PCS score was 47.7±18.5 and the average MCS score was 56.5±19.5. In disease group analysis, the PCS scores of UA, MI, and HF were 51.2±17.9, 51.2±18.0, and 35.6±16.6, respectively. They were significantly different among disease groups (F=3.62, p=0.03) by ANOVA. However, post-hoc analysis did not reveal any significant difference among groups. Disease group analysis revealed that the MCS scores of UA, MI, and HF were 57.7±15.7, 67.9±15.8, and 37.8±18.4, respectively, which were significantly different (F=12.0, p<0.001) based on ANOVA. Scheffe post-hoc analysis revealed that the HF group had significantly lower MCS score than the MI group (p<0.001) and the UA group (p=0.005). Each MOS SF-36 factor including PR (F=4.2, p=0.02), VT (F=10.7, p<0.001), MH (F=15.9, p<0.001), PCS (F=3.6, p=0.034), and MCS (F=11.9, p<0.001) showed significant differences among disease groups. The RP score in the HF group was lower (p=0.03) than that in the UA group. VT in the HF group was lower than that in the UA group (p=0.002) and the MI group (p<0.001). MH in the HF was also lower than that in the UA group (p<0.001) and the MI group (p<0.001) (Table 3).
The life satisfaction score was 4.7±1.5, which was above the ‘moderate’ score. However, there was no significant difference among disease groups (F=2.6, p=0.09) (Table 3).
Correlation between quality of life and cardiac disease
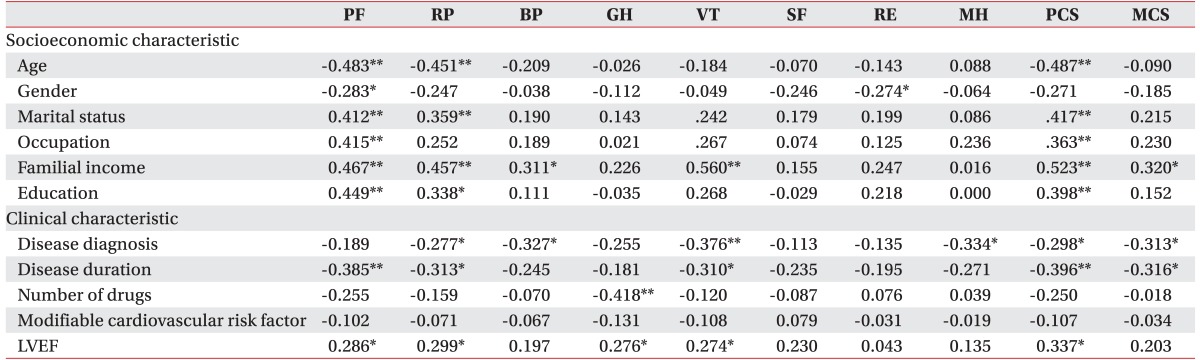
Pearson correlation analysis revealed that older age and female gender were correlated with worse statuses of several MOS SF-36 factors, including PCS (γ=−0.487, p<0.001), PF (γ=−0.483, p<0.001), RP (γ=−0.451, p<0.001), PF (γ=−0.283, p<0.05), and RE (γ=−0.274, p<0.05). Marriage and education were correlated with better PCS (γ=0.417, p<0.001), PF (γ=0.412, p<0.001), and RP (γ=0.359, p<0.001). Monthly income was significantly associated with higher SF-36 scores, including PCS, MCS, PF, RP, BP, and VT. Older age, being female, single, lower educational level, lower income, and harder work were associated with low HRQoL scores (Table 4).
Disease duration was significantly (p<0.05) associated with lower PCS (r=−0.396), MCS (r=−0.316), PF (γ=−0.385), RP (γ=−0.313), and VT (γ=−0.310) scores. LVEF was positively (p<0.05) correlated with PCS (γ=0.337), PF (γ=0.286), RP (γ=0.299), GH (γ=0.276), and VT (γ=0.274). Pearson correlation analysis revealed that disease duration and LVEF were associated with low HRQoL scores (Table 4).
Awareness of cardiac rehabilitation program
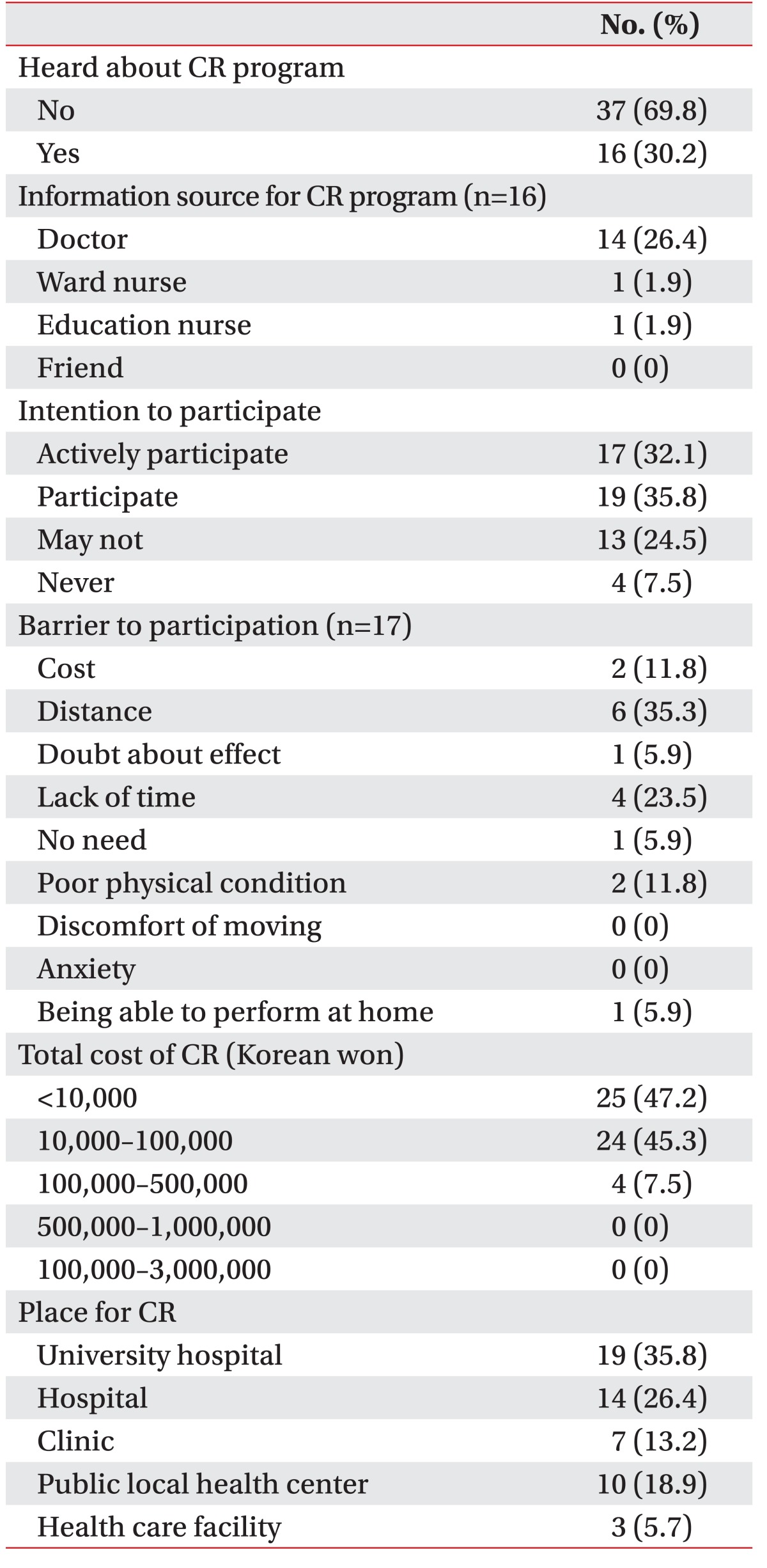
A total of 16 patients (30.2%) indicated that they had heard about a CR program. Of these 16 subjects, 14 (87.5%) reported that the person who introduced them to CR program was a doctor.
After explaining the CR program, we asked patients about their intention to participate in such program. Seventeen (32.1%) patients indicated that they would actively participate, 19 (35.8%) indicated that they might participate, 13 (24.5%) said that they might not participate, and 4 (7.5%) indicated that they would never participate. We asked these patients about barriers to participation and 23 of the 53 subjects responded. The most common barrier was distance (35.3%). Lack of time was the second most common barrier (23.5%). Almost all subjects (92.5%) selected below 100,000 Korean won as a reasonable cost for a monthly CR program. A total of 35.8% of patients reported that university hospital was the most convenient place to participate in the CR program (Table 5).
DISCUSSION
In this study, we determined the characteristics of patients admitted for cardiovascular diseases. For HRQoL, patients with heart failure due to ACS were affected more than those with just acute coronary syndrome. The overall life satisfaction of cardiac disease patients was slightly higher than that of the general population. Several MOS SF-36 factors were significantly correlated with age, gender, marriage, education level, monthly income, occupation level, disease duration, and LVEF. LDSM had a significant correlation with HRQoL. However, it had no significant correlation with patient characteristics.
Various studies on patients with heart diseases have revealed that age is a predictive factor for HRQoL, particularly after percutaneous myocardial revascularization or MI [181920]. Previous studies have demonstrated that age is a common predictor for the quality of life using MOS SF-36 MCS and PCS measures [18]. In addition, baseline PCS and MCS scores are independent predictors of follow-up PCS and MCS scores [18]. Older patients in CR programs have shown less ability to perform daily activities, which by itself can affect their perception of HRQoL [21]. At the same time, data from the literature suggest that older patients are less likely to receive more aggressive treatment [2223]. In this study, advanced age was associated with worse perception of physical quality of life, although it was not an independent predictor.
Another variable associated with HRQoL was the sex of the patient, with females being more predisposed to having lower PF and RE scores. Soto et al. [24] have also investigated HRQoL in coronary patients and found that females have worse physical dimension scores than males, particularly for PF. They suggested that this might be due to lower morbidity levels and worse CHD-related recovery in females [24]. Van Jaarsveld et al. [25] have shown that females constitute a vulnerable group with more physical limitations, more distress, and more social limitations than males. Women also had lower score in emotional factors compared to men in our study. This suggests that women with coronary heart disease might have been affected by low levels of physical activity and mental factors, thus affecting their quality of life.
Awareness of the CR program was very low (30.2%). The majority of patients who had heard about it had been informed by a physician (87.5%). A total of 67.9% of patients indicated that they would participate in CR, while only 18.9% of patients actually participated. This suggests that improving the awareness of CR program is very important. In addition, the difference between those who wish to participate in CR and the number of those who actually do so suggests that there are some barriers to participating in the CR program. Kim et al. [12] have reported that the most common cause of low participation is the lack of awareness. Having doubt about its effect and poor physical condition are also often-cited reasons. This study also suggest that the awareness of CR program is not high among people with cardiovascular diseases and that non-physician medical professionals have little idea about the availability of CR program. The most common reasons cited for not participating were distance, lack of time, and financial problems. To improve participation in CR program, further studies are needed to determine the barriers to CR participation.
Almost all patients indicated that appropriate cost for monthly CR was less than 100,000 Korean won (92.5%). Jolly et al. [26] have reported that the cost of hospital-centered CR is £486 per course. Marchionni et al. [27] have reported that direct cost (in US $2,000) calculated as the sum of CR program cost ($8,841) and healthcare utilization cost ($12,457) over the study duration is $21,298 for hospital-based CR. Given these findings, the monthly cost preferred by patients in this study was well below the average cost for CR. The most commonly cited location for CR was in a hospital (62.2%). However, Jolly et al. [26] have shown that PCS and MCS scores after 6–12 weeks of hospital-based CR and after 18 weeks of home-based CR are not significantly different. In contrast, Arthur et al. [28] and Smith et al. [29] have reported that PCS scores are higher after home-based CR. The location of CR can be a barrier to participation in CR. CR outcome may vary by location. Therefore, further studies are needed to determine the effectiveness of CR in different locations.
In conclusion, results of this study suggest that CR program needs to focus on factors associated with HRQoL. In addition, the awareness of CR program is still too low. Therefore, physicians need to improve their communication about the availability of CR program. Information obtained from this study can be used to determine appropriate ways to increase participation in CR programs in the future for patients with cardiovascular diseases.
 XML Download
XML Download