

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dysesthesia accompanied by pain in the lower extremities is a common complaint in outpatient clinics. It can result from diverse causes that include overuse of back muscles, zygapophyseal joint degeneration, disc herniation, spine instability such as spondylolisthesis, spondylolysis, lumbosacral (LS) radiculopathy, and peripheral polyneuropathy (PPNP) [1]. LS radiculopathy and PPNP are frequently present in patients with lower extremity dysesthesia [23]. Physical examination and pain questionnaires may not be adequate for a diagnosis because of their subjective nature, which underestimates detection compared to other tools [4]. Imaging of only structural lumbar lesions can be insufficiently revealing and provides limited information in cases of LS radiculopathy. Nerve conduction study (NCS) and needle electromyography (EMG) can help diagnose LS radiculopathy and PPNP [5678]. However, these tools can only reveal abnormalities of the large fiber nerves and not those involving the small fibers [9]. Small fiber dysfunction has been linked to pain associated with diabetic neuropathy, chronic kidney disease, autonomic diseases, vasculitis and fibromyalgia [10].
There is a need for tests that are less time-consuming and less invasive than conventional tests. Also, assessment of small fibers through sudomotor evaluation might be helpful in evaluating dysesthesia of the lower extremities. The American Diabetes Association recommends evaluation of sudomotor function for early diagnosis of neuropathy and small fiber involvement in diabetes mellitus (DM) patients [11]. SUDOSCAN (Impeto Medical, Paris, France) is a novel quantitative assessment tool that provides index values of the thin, unmyelinated C fibers and assesses sudomotor function by evaluating the secretory function of the sweat glands. This device is a noninvasive, painless, and convenient tool that measures electrical conduction activity in the hands and feet by reflecting cholinergic neurotransmission of the sweat glands. Also its diagnostic validity to reflect small fiber function has already proven by past test with skin biopsy results [12131415]. However, the current literature on its use has been mainly limited to PPNP patients, and its application to other patients with lower extremity dysesthesia related to different causes have not been proven. Proper diagnosis of sudomotor dysfunction, which can lead to painful dysesthesia, is important [916]. The clinical utility and benefit of evaluating sudomotor dysfunction using SUDOSCAN among outpatients with mixed etiologies remain unclear.
In addition to patients with PPNP, there is evidence that both the sudomotor system and sympathetic responses are involved in patients with painful LS radiculopathy [161718]. Significant prolongation of sympathetic skin response (SSR) latency has been found in LS radiculopathy and failed back surgery syndrome (FBSS) [1617]. There is a considerable theoretical support to help detect sympathetic and sudomotor dysfunction in LS radiculopathy. However, no clinical studies have attempted to use it in patients with LS radiculopathy.
The primary study objective was to investigate whether SUDOSCAN could detect differences of its parameters in outpatients with dysesthesia of the lower extremities related to PPNP or LS radiculopathies who had been referred for NCS and EMG evaluations. The secondary objective was to assess the diagnostic validity of the obtained values related with sudomotor dysfunction values and determine the clinical utility compared with conventional NCS and needle EMG studies.
MATERIALS AND METHODS
Patient enrollment
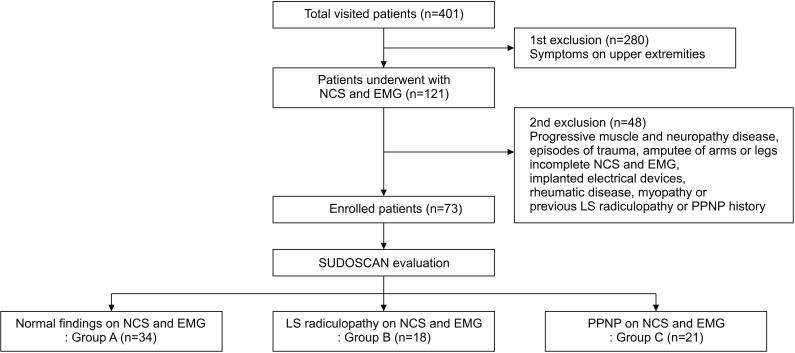
This cross-sectional study was conducted from May 1, 2015 to August 31, 2015, and was based on outpatients who had been referred from an NCS and EMG clinic for dysesthesia and discomfort in the lower extremities to the EMG clinic at our institution. Preliminary clinical history taking, physical, and electrophysiological examinations were performed by physicians. Exclusion criteria were symptoms and signs confined to the upper extremity related to cervical radiculopathy or upper extremity entrapment neuropathies, prior amputation of arms or legs and implanted electrical devices, episodes of trauma, incomplete electrophysiologic studies, and previous LS radiculopathy or PPNP history (Fig. 1). The study protocols were approved by Bucheon St. Mary's Hospital, Catholic University of Korea local ethical boards of committee (HC15RISI0100).
Patient demographic characteristics
Clinical and demographic characteristics, including sex, age, pre-existing comorbidities like DM, lumbar spine surgery, alcohol consumption, body mass index (BMI), serum fasting glucose, serum uric acid, serum creatinine, total cholesterol (TC), total triglyceride (TG), low-density lipoprotein (LDL), and high-density lipoprotein (HDL) were retrieved from medical records. The Michigan Neuropathy Screening Instrument (MNSI) and visual analogue scale (VAS) were used to record the nature and severity of pain.
NCS and EMG
NCS was performed with a Viking Electromyography System (Nicolet-Viasys Biomedical Inc., Madison, WI, USA) with a setting of 20 Hz for the lower filter, 3 kHz for upper filter for sensory studies, and 5–10 kHz for motor studies. The pulse duration was with 0.1 ms. NCS tests included the sural sensory, superficial peroneal sensory, common peroneal motor, and tibial motor nerves. The minimum F-response latencies from both tibial nerves and H-reflex latencies from tibial nerve stimulation were collected. EMG needling was done by inserting the monopolar needle in selected lower extremity muscles and lumbar paraspinalis muscles from the L1-L2 to L5-S1 levels. All NCS and EMG tests were performed by experienced physicians with more than 3 years experience in the procedures. NCS results obtained from only one side were used in the statistical analysis.
Patients were stratified by electrophysiological results into normal (group A), LS radiculopathy (group B), and PPNP (group C) findings. Group A patients had normal latency range and amplitude on NCS without abnormal spontaneous activity in the sampled muscles. Group B patients had abnormal spontaneous activity, such as positive sharp waves and other denervation potentials, in the tested muscles with normal NCS parameters [1920]. Group C had reduced sensory nerve action potential (SNAP) amplitudes of the sural nerve (<10 µV) and abnormal peroneal (compound muscle action potential [CMAP] and/or F-wave) responses [21]. Patients were included in group C when reduced amplitudes of SNAPs in both sural nerves [22].
ESC and SUDOSCAN-risk score
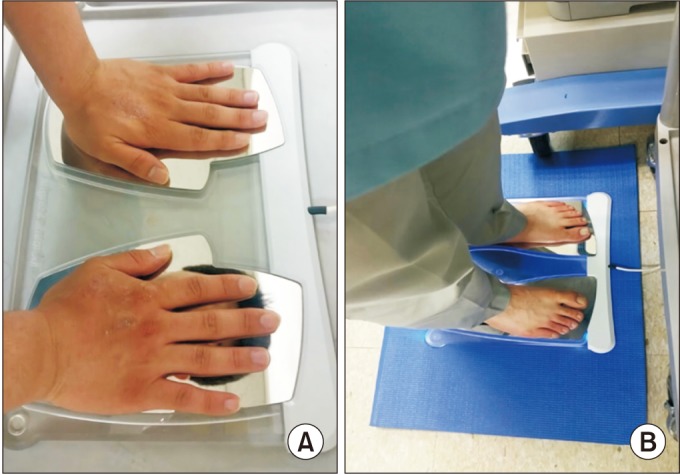
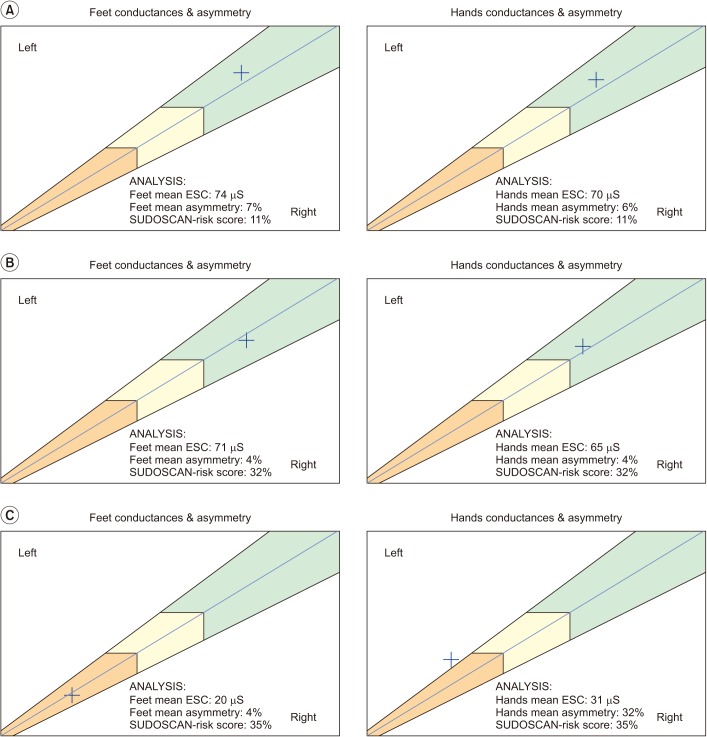
SUDOSCAN was performed on the same day by a separate examiner blind to patient's clinical symptoms and history before NCS and EMG evaluation. Sudomotor function was assessed as ESC values and SUDOSCAN-risk score using two pairs of electrodes for the feet and hands, and connected to a computer for data recording and modulation [11]. Subjects maintained contact with the electrodes for 3 minutes after their age, height, and weight had been recorded (Fig. 2). ESC values were calculated by analysis of electrochemical currents generated in response to low voltage stimulation and expressed in microsiemens (µS) [12] (Fig. 3).
Lower ESC values indicated dysfunction of the sweat glands. SUDOSCAN-risk scores were calculated automatically from ESC values, BMI, and age using an algorithm included in the device software. Scores are presented as percentages. Higher SUDOSCAN-risk scores have been related to increased risk of cardiac autonomic abnormalities. Both ESC values and SUDOSCAN-risk scores were displayed numerically with graphs on the device monitor.
Statistical analyses
Descriptive statistics are expressed numerically and as percentages for categorical variables, and as mean±standard deviation for continuous variables. Demographic characteristics and NCS values were compared by Kruskal-Wallis test followed by Man-Whitney U-test to identify differences among the three groups. Analysis of covariance (ANCOVA) followed by least significant difference (LSD) analysis were used to compare differences of SUDOSCAN-risk scores, hands-ESC, feet-ESC, and asymmetry of ESC on hands and feet, among the three groups with adjustment for age and DM history, which was confirmed showing normal distribution by Kolmogorov-Smirnov test [23].
Receiver operating characteristic (ROC) curves were calculated to estimate the effectiveness of foot-ESC values to predict PPNP and SUDOSCAN-risk scores in the abnormal electrophysiological findings of groups B and C. Spearman correlation coefficients were calculated to correlate NCS parameters (SNAP latencies and amplitude) with hands-ESC, feet-ESC, and SUDOSCAN-risk score. Two-sided p-values <0.05 were considered significant. Statistical analyses were performed using SPSS ver. 19.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Enrollment and demographic characteristics of outpatients
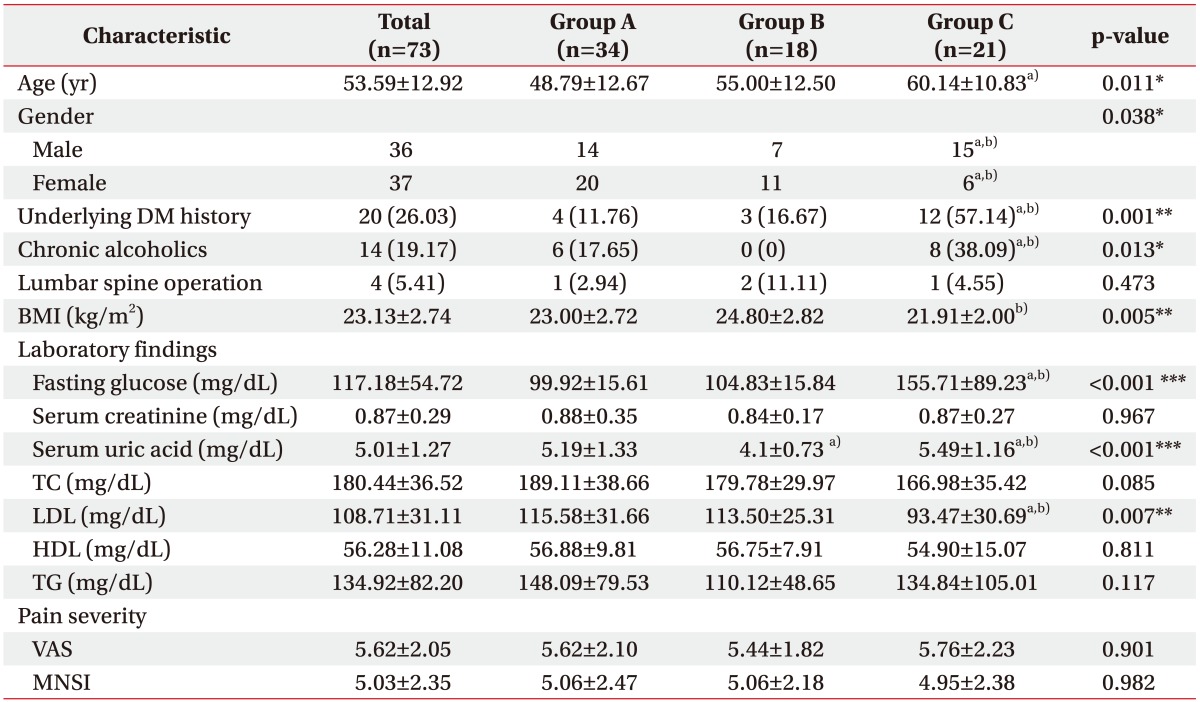
Out of the 401 patients who visited the electromyography clinic, 73 outpatients met the inclusion criteria. Thirty-four patients had normal NCS and EMG results (group A), 18 were diagnosed with LS radiculopathy (group B), and 21 with PPNP (group C). The patient demographic and clinical characteristics are shown in Table 1. There were no significant differences in MNSI and VAS scores among the three groups. There were significant baseline differences in age, sex, history of DM and alcohol abuse, BMI, serum fasting glucose, serum uric acid, and LDL level.
NCS and EMG results
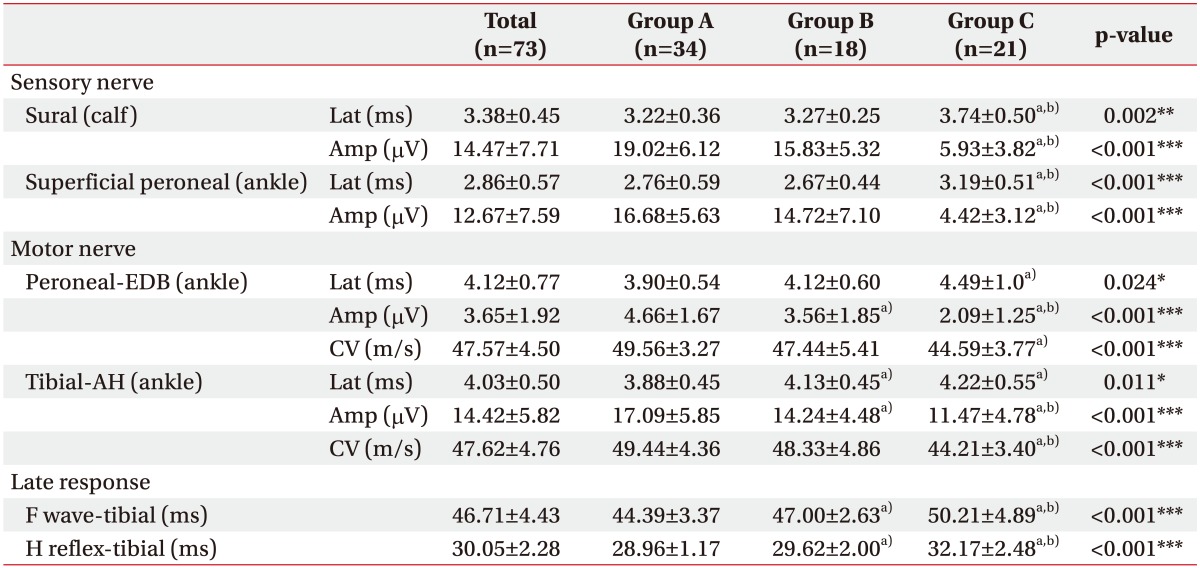
NCS did not reveal right to left side difference in any group. As expected, the latencies and amplitudes of SNAPs and CMAPs in all tested nerves of group C were significantly lower than in other groups (Table 2). The EMG profiles in group B showed denervation potentials in the lumbar paraspinalis muscles with multiple level involvement in 7 patients (38.9%), single level involvement in 8 (44.4%) patients, and in the lower limbs in 7 patients (38.9%). PPNP was associated with underlying alcohol consumption in 4 patients, uremia in 2, DM in 12, and was idiopathic in 3.
Low feet-ESCs were significantly correlated with decreased amplitudes of SNAPs of sural and superficial peroneal nerves (r=0.274 to 0.358, p<0.002 to 0.019). Hands-ESCs showed no correlation with amplitudes of sural and superficial peroneal nerves (r=0.133 to 0.198, p=0.126 to 0.263). High SUDOSCAN-risk score was significantly correlated with decreased SNAP amplitudes in both sural and superficial peroneal nerves (r=−0.352 to −0.415, p<0.001 to 0.002). ESC values and SUDOSCAN-risk score were not statistically correlated with latencies in both sural and superficial peroneal nerves.
Differences of SUDOSCAN values
ESC values and its diagnostic validity
Comparison of ESC values among the three groups was done using ANCOVA followed by LSD. The results indicated that feet-ESC values and asymmetry of group C were statistically different from those in groups A and B (Table 3).
Feet-ESC had a 57.1% sensitivity and 94.2% specificity at 48 µS to detect PPNP (95% confidence interval [CI], 0.646–0.915) with 80.0% positive predictive value and 84.5% negative predictive value. Hands-ESC had 71.4% sensitivity and 78.8% specificity at 55 µS (95% CI, 0.577–0.860) with a 57.7% positive predictive value and 87.2% negative predictive value.
SUDOSCAN-risk score
ANCOVA followed by LSD revealed significantly higher SUDOSCAN-risk scores were in groups B and C than group A (Table 3). The sensitivity and specificity of the SUDOSCAN-risk score for detecting abnormal electrophysiological findings (LS radiculopathy and PPNP) were 64.1% and 82.4%, respectively, at a cut-off on 29% and area under the curve (AUC) of 0.780 (95% CI, 0.674–0.886) with a positive predictive value of 80.65% and negative predictive value of 66.67%.
DISCUSSION
The results demonstrate that sudomotor evaluation through SUDOSCAN can help discriminate outpatients with dysesthesia of the lower extremities attributable to LS radiculopathy or PPNP. Although similar in clinical pain intensity, ESC values in the feet were significantly lower in patients diagnosed with PPNP, whereas the SUDOSCAN-risk score was higher in patients with LS radiculopathy or PPNP. The feet-ESC values at cut-off value of 48 µS, showed high specificity of 94.2% with 57.1% sensitivity to discriminate those with normal electrophysiologic findings and without PPNP. The sensitivity and specificity of the SUDOSCAN-risk score to detect abnormal electrophysiological findings (LS radiculopathy or PPNP) was 64.1% and 82.4%, respectively, at a 29% cut-off value. Overall, lower feet-ESC and higher SUDOSCAN-risk scores were found in those with PPNP, whereas higher SUDOSCAN-risk scores and normal feet-ESC values were found in those with LS radiculopathies. Findings of this study are relevant that SUDOSCAN may be a rapid, objective, and noninvasive method to evaluate sudomotor dysfunction and discriminate patients with LS radiculopathies and PPNP.
Recent studies have confirmed the diagnostic validity of ESC values, with a sensitivity of 73% to 78%, and specificity of 62% to 100% to screen PPNP in patients with diabetes as well as idiopathic and chemotherapy-induced PPNP [1213141524]. Previous studies evaluating the SUDOSCAN-risk score reported 65%–92% sensitivity and 49%–80% specificity to detect cardiac autonomic neuropathy [1425]. But, whether this score is helpful in radiculopathy has not been studied. Presently, we decided to determine whether patients with LS radiculopathies would have abnormal ESC values. The rationale was based on the possible association of sympathetic nerve dysfunction and LS radiculopathy previously suggested in studies that used SSR, an assessment tool similar to the SUDOSCAN, which evaluates sudomotor function [1161718].
Immunostaining revealed an increase of sympathetic fibers in radiculopathy lesions of dorsal root ganglia (DRG) at L4 and L5 in an animal model of spinal root-constriction [26]. Possible mechanisms involve inflammatory neuropeptides, such as substance P, calcitonin, and neuropeptide Y, which may spread from the spinal roots to the DRG at each spinal nerve level. Interactions in the vicinity of sinuvertebral nerves formed by sympathetic postganglionic and afferent sensory fibers [27] would result in sympathetic dysfunction in patients with LS radiculopathies. The abnormal stimuli would then be conveyed to the central nervous system from the dorsal horns of the spinal cord to generate hypersensitive autonomic reflex arcs resulting in low back and referred pain in the involved dermatomes [2728]. The role of abnormal autonomic reflexes in pain generation has also been confirmed in previous studies of the clinical benefits of spinal cord stimulators that help stabilize aberrant sympathetic responses in FBSS [2930].
Of clinical interest, our results revealed that SUDOSCAN-risk score in those with LS radiculopathy was increased although ESC values showed no differences compared to the normal group in NCS and EMG. This interesting result might be explained by past SSR studies that showed abnormal sudomotor functions in patients with lumbar lesions involving only they latency but not involving SSR amplitudes [1617]. SSR latency reflects peripheral C fiber function and conduction in long multi-neuronal pathways and SSR amplitude reflects the density of sweat glands [31]. Considering that ESC value reflects only the density of sweat glands, but not the latencies, involved in multi-neuronal pathways with the autonomic system, it is reasonable to conclude that the abnormal autonomic dysfunction involved in LS radiculopathies, related to delayed latencies of SSR, were reflected only in the SUDOSCAN-risk score . Therefore, the exception of abnormal SUDOSCAN-risk score with normal ESC values in patients with lumbar lesions may be a useful marker to detect abnormal sympathetic dysfunction. The clinical significance of SUDOSCAN-risk score abnormalities related with SSR latency is a topic that warrants more rigorous research.
The results can be applied meaningfully to clinical approaches to outpatients with dysesthesia in lower extremities. First, while previous studies focused on patients who had already been diagnosed with PPNP, this is the first study to evaluate SUDOSCAN in a cross-sectional study of outpatients with dysesthesia of the lower extremities. Our results show that sudomotor assessment may be used as a complimentary test to standard NCS and EMG studies. Secondly, previous studies on the diagnostic validity of ESC compared it with the vibration potential threshold, quantitative sudomotor axon reflex testing, and symptom scales like MNSI as references [32]. But, there is no report about SUDOSCAN with direct NCS and EMG results, which are the gold standard tools to detect PPNP [5678]. Our study validates ESC values and SUDOSCAN-risk scores to NCS and EMG values, and shows the high specificity diagnostic power in PPNP.
Unlike past studies on the diagnostic validity of SUDOSCAN, our results revealed lower levels of sensitivity but higher levels of specificity. This discrepancy may be attributable to different patient populations with the main objective to validate it in mostly outpatients with lower extremities dysesthesia due to more heterogenic causes. The 94.2% specificity level, which is indicative of low false negativity rates, is preferable to diagnose those without the disorder [3334]. High levels of specificity are necessary for the gold standard tests that may be expensive, time-consuming, and invasive such like NCS and EMG [35]. Because SUDOCAN exclusively assesses the small fibers function of the sweat glands and reflects sudomotor dysfunction, it cannot in principle reflect the large fibers dysfunction and denervation potentials obtained from NCS and needle EMG, and so cannot replace these two tests. However, considering the high level of specificity with the minimal false positive rate, it may help expedite the diagnosis of those who may show negative results in NCS and needle EMG in a rapid, low-cost, and non-invasive manner.
From this point of view, SUDOSCAN, which is a simple, quick, and non-invasive test, can be advantageously and effectively used in outpatient clinical situations. Especially, our SUDOSCAN-risk score results suggest the appropriate applicability of LS radiculopathy as well as PPNP. In addition, considering that normalized SSR latency in FBSS was reported in the use of SCS to stabilize sympathetic dysfunctions [29], the clinical utility of sudomotor evaluation as a measure of pain improvement or therapeutic response would be an interesting topic to investigate. Future studies of the relationship between LS radiculopathy and sudomotor dysfunction will be wise to expand the scope of the SUDOSCAN test.
There are several limiting factors of this study. This study is limited by its small size, despite statistically reliable and meaningful results. Small sample sizes can produce statistically unintentional errors because of heterogeneous patient populations. Second, group B with LS radiculopathy included uneven involved levels of distribution. Almost all subjects in group B were diagnosed as lower LS radiculopathy involving L4, L5 or/and S1, except for one involving L2 nerve root with 55 µS on feet ESC, which was lower by 10 points than the average in the LS radiculopathy group. Therefore, further study of sudomotor dysfunction using SUDOSCAN for LS radiculopathy undoubtedly needs to be done with a large population including upper lumbar radiculopathy. Third, patients with lower extremity dysesthesia may have the sudomotor abnormality even if they are not diagnosed with peripheral neuropathy or radiculopathy in NCS and EMG. Also, SUDOSCAN may not detect subtle sudomotor changes depending on the severity of radiculopathic lesions. Since group A as a control group did not exclude other causes of pain, it is necessary to compare group B with the healthy control group without pain symptom and patients with herniated disc lesion or spinal stenosis of group A.
In conclusion, this cross-sectional study is the first report of the usefulness of SUDOSCAN in outpatients with lower extremities dysesthesia including those with lumbar lesions and PPNP. Results obtained from preliminary SUDOSCAN evaluation may help complement NCS and EMG testing. Abnormal ESC and SUDOSCAN-risk scores indicate not only involvement of sudomotor in these patients but may also reflect the need of additional NCS and EMG to further confirm the presence of LS radiculopathy or PPNP. Normal ESC and SUDOSCAN-risk scores increase the probability of normal NCS and EMG results. Subsequent studies that expand the application of sudomotor dysfunction using SUDOSCAN testing and how this new assessment tool could complement with current NCS and EMG evaluations are warranted.

 XML Download
XML Download