

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Health policies and insurance system, as well as the progression of medical knowledge, could affect the epidemiological features of diseases. For example, in the field of gastric cancer, a national screening system using endoscopy is implemented in Japan and South Korea. Attributed to the screening program in Japan, the rate of early gastric cancer was 50% in 1950–1990 and 68% in 2004.1 In Korea, during the past two decades, the proportion of early gastric cancer has increased from 25% to 50%, and 5-year overall survival after surgery was reported to be over 92%.23
In South Korea, the National Health Insurance (NHI) achieved universal coverage of the population in 1989, and finances the Republic of Korea’s health system. The NHI covers approximately 97% of all Koreans. In 2000, all insurance schemes were merged into a single payer. Under a single-payer health insurance system, it could be feasible to collect utilization data of the entire population.4 The National Health Insurance Services (NHIS) has established various big data databases by developing and applying the method of claiming medical expenses as an electronic record requesting method. Therefore, NHIS data of South Korea is highly accessible and suitable for observing overall trends.
Appendicitis is a common surgical disease with natural and independent disease progression compared with other diseases. The disease progresses from early acute appendicitis to perforation and peritonitis, which can lead to significant morbidities.5 For this reason, rapid and accurate diagnosis with early surgery remains the treatment of choice. Among the diagnostic modalities of appendicitis, computerized tomography (CT) is known for its higher sensitivity and specificity rates.67 The insurance coverage of CT in South Korea was initiated in 1996 and expanded gradually to include patients with acute abdominal symptoms. In addition, the number of CT units per million in South Korea increased from 31.0 in 2002 to 37.0 in 2015.8 The present study aimed to investigate the relationship between the incidence of appendectomy and enhanced accessibility to CT scan using a nationwide database in Korea. Economic features and age of patients who underwent appendectomy were also evaluated based on the Korean medical care system.
METHODS
Study population and data source
Appendicitis was defined by the International Classification of Diseases, Tenth Revision, Clinical Modification codes: specifically K35 (acute appendicitis), K36 (other appendicitis), and K37 (unspecified appendicitis). The study population was defined as patients with confirmed appendicitis who had undergone appendectomy between January 2003 and December 2017. Types of appendectomy for the patients with appendicitis were categorized based on Korean procedure codes; Q2580 (incision of periappendiceal abscess), Q2861 (appendectomy for simple appendicitis), Q2862 (appendectomy for perforated appendicitis), Q2863 (removal of appendiceal abscess) (Supplementary Table 1). The patients with Q2861 procedure code were classified as the group of appendectomy for uncomplicated appendicitis (AU) and the patients with other procedure codes were classified as the group with appendectomy for complicated appendicitis (AC). The records of appendectomy patients were provided by the NHIS, which is a government-affiliated agency in Korea. To compute the age-standardized rate (ASR) of appendectomy, we first calculated the age-specific rates for each group by dividing the number of cases by the respective population, and then multiplied the age-specific mid-year population as the numerator. Subsequently, the sum of numerator was divided by the mid-year population and then finally multiplied by 100,000. Since 2011 was the middle of the year between 2003 and 2017,8 we used the mid-year population from the Statistics Korea report in 2011.
Data collection
The NHIS has operated a national health insurance data sharing service since 2014 and provides the eligibility database as both the national health claim database and health care utilization database. Precisely, the NHIS database consists of 4 divisions, including the statement, details of treatment, type of disease, and details of the prescription. The NHIS database includes information regarding demographic variables, such as date of birth or death, income-based insurance contributions, and health screening data. Moreover, the health care utilization database in the NHIS collected data on the process of claiming health care services, length of stay, and treatment costs, etc.
Statistical analysis
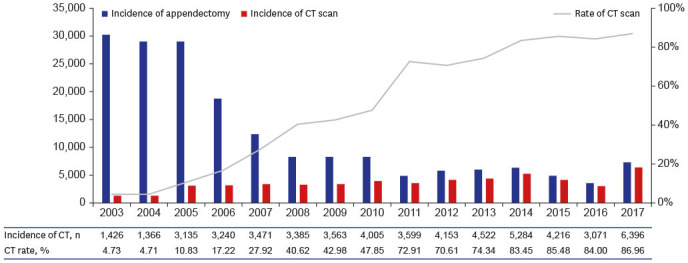
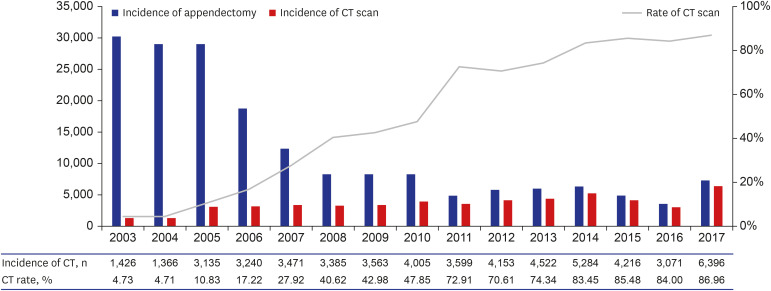
We conducted descriptive analysis for the association between the incidence of appendectomy and CT scan. Using the incidence of CT and CT rate, we showed demographic characteristics of appendectomy by year (Table 1) and conducted Pearson’s correlation analysis to determine Pearson’s r (Fig. 1). The cross-correlation test was used for the correlation analysis considering time-series between the ASR of appendectomy and CT scan (Supplementary Fig. 1).
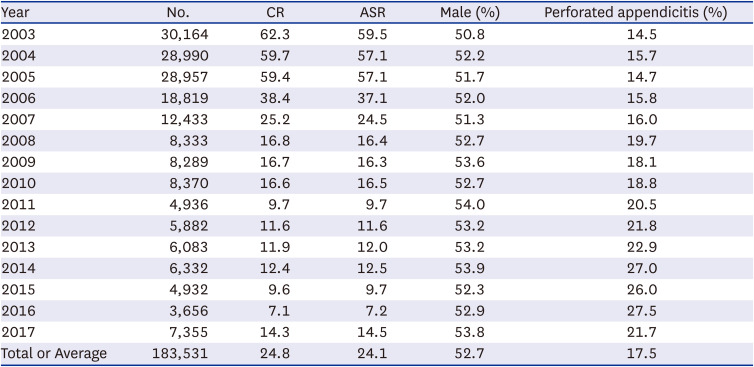
Table 1
Demography of appendectomy in Korea by year
Ethics statement
The study was reviewed by the Institutional Review Board of the Gachon University Gil Medical Center, which waived the requirement for ethics approval in compliance with governmental laws and regulations (protocol GCIRB2019-039), and that of informed consent because only the de-identified historical data were accessed.
RESULTS
A total of 183,531 patients had undergone appendectomy for appendicitis between 2003 and 2017. Crude number of appendectomies tended to decrease from 30,164 cases in 2003 to 3,656 cases in 2016, while in 2017, it slightly increased to 7,355 cases compared to the previous year. Crude rate and ASR showed similar patterns to crude number. The study population comprised of 52.7% men with no significant variation according to the year. The rate of AC had a tendency to increase from 14.5% in 2003 to 27.5% in 2016, while it decreased to 21.7% in 2017 (Table 1).
The relationship between the incidence of appendectomy and CT scan is depicted in Fig. 1. The incidence of CT scan was 1,426 in 2003 and 6,396 in 2017. The rate of CT scan for diagnosis of appendicitis has shown considerable increase (4.73% in 2003 and 87.96% in 2017). The Pearson’s correlation coefficient between the incidence of CT and ASR of appendicitis was −0.760. In addition, according to the cross-correlation analysis, the cross-correlation coefficient was largest at 0 lag (within 1 month) and showed a high correlation up to the 2nd period (within 3 months). The ASR of appendectomy followed the CT scan. It demonstrated that an increase in the incidence of CT scan affected the decrease in the ASR of appendectomy (Supplementary Fig. 1).
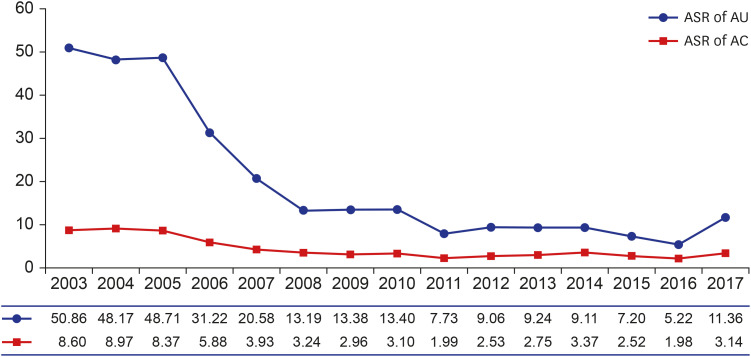
The alterations in ASR of appendectomy in AU and AC are shown in Fig. 2. The ASR in AU decreased between 2005 and 2010. The ASR in 2005 was 48.71, decreased to 13.40 in 2010, and has maintained at or below 10 since 2011. On the other hand, the ASR in AC tended to decrease gradually, from 8.37 in 2005 to 2.96 in 2009, and since 2010, it was maintained at or below 3. In addition, these alterations in the ASR in AC, which gradually increased, was observed in common regardless of income and age of the patients (Supplementary Tables 2 and 3).
Fig. 2
Alterations of ASR of simple and perforated appendectomy.
ASR = age-standardized rate, AU = appendectomy for uncomplicated appendicitis, AC = appendectomy for complicated appendicitis.
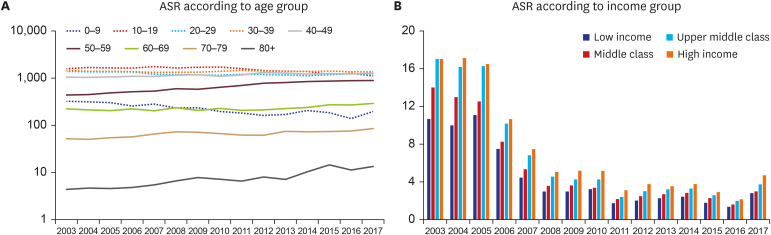
The alteration of ASR based on age and income group are shown in Fig. 3. The ASR in the younger age group decreased and that in the older age group increased steadily with year. For example, the ASR in the 20 to 29 years group was 1,381.9 in 2003 and 1,187.9 in 2017. The ASR in the 70 to 79 years group was 51.8 in 2003 and 85.3 in 2017 (Supplementary Table 4). The age groups with decreased ASR are expressed as dotted line and the age groups with increased ASR as solid line in Fig. 3. On the other hand, in proportion to the income, the ASR was higher in order, and was maintained regardless of the year (Supplementary Table 5).
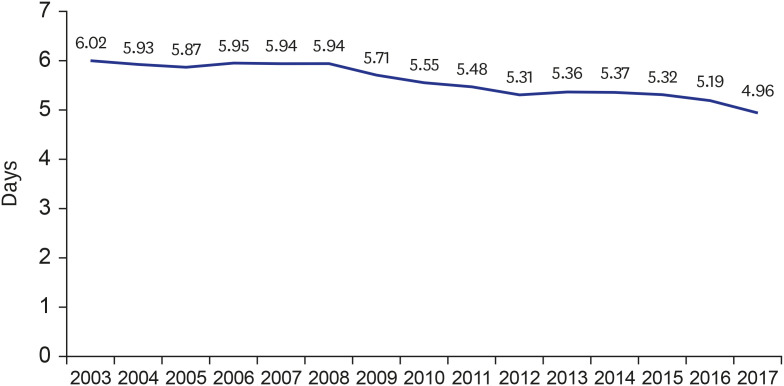
The yearly alteration of admission duration is shown in Fig. 4. The admission duration had significantly decreased from 6.02 in 2003 to 4.96 in 2017 (P = 0.031).
DISCUSSION
The current study has indicated that the incidence of appendectomy in South Korea showed a considerable decrease from 2003 to 2017. The proportion of patients who underwent appendectomy with CT increased rapidly. The increased accessibility to CT has made it possible to diagnose appendicitis more accurately and easily. In addition, considering the results of the rapid decline in the ASR in AU compared with the ASR in AC, it could be suggested that negative appendectomy, which is appendectomy in patients with normal appendices, can be avoided with an increase in CT scans. This result is consistent with that of previous studies. In a large multi-center retrospective analysis in the USA, imaging studies, including CT, were associated with lower negative appendectomy rate. The rate of negative appendectomy was 3.5% and 19.2% in patients with and without preoperative imaging, respectively.7 A single-center study in adult patients with suspected acute appendicitis reported that the annual rate of use of preoperative CT increased from 20% in 1996 to 85% in 2006, and the overall rate of false positive diagnosis of appendicitis decreased significantly, from 24% to 3% in the same period.9
According to the conventional pathophysiologic model of acute appendicitis, time elapsed from onset of disease to treatment has a relationship with disease progression, including perforation. Several observational studies have demonstrated the association between accessibility to health care and increased risk of perforation. If appendicitis progressed, the scope of surgery may be expanded beyond appendectomy, including resection of ileum or colon. It is known that the occurrence of acute appendicitis is generally independent of income level.10 Therefore, the different ASR based on the income group in the present study could be affected by the difference in medical accessibility. Low-income groups may have a low level of medical service utilization, more infectious microorganisms, and a high prevalence of unhealthy lifestyles, such as smoking, or a decrease in immunity due to chronic stress.1011 In addition, the NHI system of South Korea has a major drawback that requires a relatively high out-of-pocket cost. These high co-payments can act as a factor that restrains financially burdened patients from using hospitals, thereby eventually allowing disease progression.12 Previous studies revealed that patients who cannot afford commercial insurance are more likely to present with complicated appendicitis in adults and children, and are consistent with the results of the present study.1314
In the present study, the length of hospitalization (LOH) for appendectomy significantly decreased with years. Considering that the average time to surgery (door to incision time) in previous large-scale studies was approximately 7 to 8 hours, decreased LOH might be the result of advances in postoperative care.1516 The LOH after appendectomy can be affected by postoperative pain and diet schedule. Although not covered in this study, in Korea, the rate of laparoscopic appendectomy gradually increased. A Korean single-center retrospective study reported that 2,587 cases of appendectomy were conducted in laparoscopic setting among consecutive 2,600 cases between 2008 and 2013.17 Laparoscopic appendectomy has the advantage of less postoperative pain and short hospital stay.18 In addition, development of multimodal pain managements, such as rectus sheath block and preoperative pain education, can contribute to the reduction in LOH.1920 In a recently conducted randomized clinical trial, it was demonstrated that enhanced recovery after surgery program can be applied in the field of laparoscopic appendectomy. In this program, patients advanced to their regular diet in 6 hours after surgery.21
In addition to the development of operative techniques and postoperative care, advances in emergency medicine for emergency surgery, including appendectomy, has been demonstrated to reduce LOH in recent studies. In the traditional on-call system (TROS) in which doctors covered outpatients, inpatients, and emergency room (ER), emergency surgery or treatment can be delayed do to workload of doctors. To overcome these limitations, acute care surgery (ACS) system was introduced, in which a specialist doctor stays in the ER and covered only emergent patients. In a previous study applying ACS system on the management of acute appendicitis, LOH was significantly shorter compared with TROS group (4.3 days vs. 7.2 days, respectively).22
This study has limitations. First, the imaging diagnostic tools for appendicitis includes not only CT scans, but also ultrasound (US) and magnetic resonance imaging (MRI). CT scans confer the risk of exposure to ionizing radiation. For this reason, US and MRI could be useful for appendicitis in pediatric and pregnant groups. However, the data of US and MRI were not included in our nationwide dataset because they were recently covered by insurance in South Korea. In addition, peri-appendiceal abscess arising from appendicitis and extended surgery beyond appendectomy, including ileo-cecectomy and colectomy, were not investigated. Second, medical cost, including out-of-pocket cost, was not analyzed in the present study, although medical cost is one of the important factors related to medical accessibility. Third, the impact of diagnosis-related group (DRG) payment system was not evaluated in the present study. In the field of appendectomy, DRG payment system began with clinics and smaller hospital in July 2012, followed by the larger general and tertiary hospitals in July 2013. Although no drastic changes were observed for the incidence of CT scan and LOH in 2012 and 2013 in the present study, future research will be needed to evaluate the impact of DRG for the trend of appendectomy. Finally, as this study used NHIS data, it is difficult to explain a direct causal relationship or mechanism, and there is a limitation that it can show only the current situation. However, the results of the present study would help establish future health care policies by understanding the current situation.
In conclusion, with the development of the economy and medical system in Korea, accessibility to medical care has improved. Accurate and rapid diagnosis of appendicitis, performed through readily available CT scans, could reduce the incidence of appendectomy with time. Advances in the perioperative system and modalities decreased LOH gradually. Policy makers should pay special attention to social groups with poor medical accessibility and ensure that all people can receive proper diagnosis and treatment of various diseases.
 XML Download
XML Download