

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Vulvar cancer is a rare gynecologic malignancy and accounts for less than 5% of all gynecologic cancers.1 The incidence rate of vulvar cancer is lower in Asia than in Western countries, in which age-adjusted incidence rates have been reported to be approximately 2 per 100,000.23 While there have been several population-based studies of vulvar cancer in Western countries,1456 due to the rare nature of vulvar cancer in Asia, only one epidemiological study from Japan has been published to date.3 Although it is important to have current data regarding the incidence and treatment of vulvar cancer throughout Asia, no studies have been completed in South Korea.
Human papillomavirus (HPV) is associated with various malignancies, including cancers of the cervix, vagina, anus, and vulva in women. In previous studies, HPV was found in about 40% of vulvar cancers.789 Over the past few decades, not only has the incidence of HPV-related genital/oropharyngeal cancers increased, but also the attributable fraction of HPV to HPV-related cancers has increased. The cause of this increase has been attributed to increased exposure to HPV, especially among younger women.1011 It is expected that the prevalence of vulvar cancer in Korean women will decrease slightly over the next few decades due to the national prophylactic HPV vaccination program; however, this effect will be limited to HPV-associated vulvar cancer. The aim of this population-based study was to assess the prevalence and treatment of vulvar cancer in South Korea between 2014 and 2018.
METHODS
Data sources and study population
The Korean National Health Insurance program provides a wide range of health care services to more than 98% of the South Korean population of approximately 49 million. Medical insurance services are provided to almost all people living in the country through the National Health Insurance Corporation (NHIC). The NHIC provides health insurance services for most diseases, and the NHIC database includes all relevant information, such as age, sex, income, diagnosis, prescriptions, and management (medication and/or surgery). The Health Insurance Review and Assessment Service (HIRA) is an institution that reviews medical expenses charged from medical institutions and supervises whether they are properly paid. Therefore, the HIRA and NHIC share information to a large degree.
The HIRA National In-Patient Sample (HIRA-NIS) database contains a subset of data collected annually from the full HIRA database after stratified randomized selection of applicable patient records. Because new sampling for the HIRA-NIS is undertaken every year, the sample group differs from year to year. The yearly HIRA-NIS sample population includes 1.4 million patients, accounting for 3% of the total HIRA data. For our analyses, we used HIRA-NIS data collected from 2014 to 2018.
Patients with vulvar cancer were defined as having diagnostic codes for vulvar cancer C51.0–C51.9. Patients who underwent surgery for vulvar cancer were defined as having a diagnostic code of C51 with surgery codes including benign vulvectomy (R4066), simple malignant vulvectomy (R4067), and radical malignant vulvectomy (R4068). Patients who were treated with chemotherapy were defined as having a chemotherapy code (KK151, KK151300, KK152, KK152300, KK153, KK153300, KK154, KK154300, KK155, KK155300, KK156, or KK158), and those who underwent radiotherapy were defined as having a radiotherapy code (HD051, HD051300, HD052, HD052300, HD053, HD053300, HD054, HD054300, HD055, HD055300, HD056, or HD056300). Sub-analyses were performed according to age group. Low socioeconomic status (SES) was defined as patients with a non-general insurance code, which is used for recipients of livelihood programs and household individuals.
Statistical analyses
To compare continuous variables during the study period, the t-test was used. The year and age were designated as independent variables. The diagnosis of vulvar cancer and the surgery and treatment codes were designated as dependent variables, for which odds ratios (OR) and 95% confidence intervals (CI) were calculated using logistic regression. A P value of less than 0.05 was considered statistically significant. All statistical tests were two-tailed. Weighted analyses were used to compare the means of continuous variables. The weighted Pearson’s χ2 test was used for statistical analyses of categorical variables. We utilized weighted logistic regression analyses to calculate risks for multiple variables.
Ethics statement
This study was approved by the Institutional Review Board (IRB) of Kangwon National University Hospital (KNUH-2020-05-004-001) in accordance with the Declaration of Helsinki. Anonymized and de-identified information for participants was used for all analyses, so the requirement for informed consent or parental permission was waived.
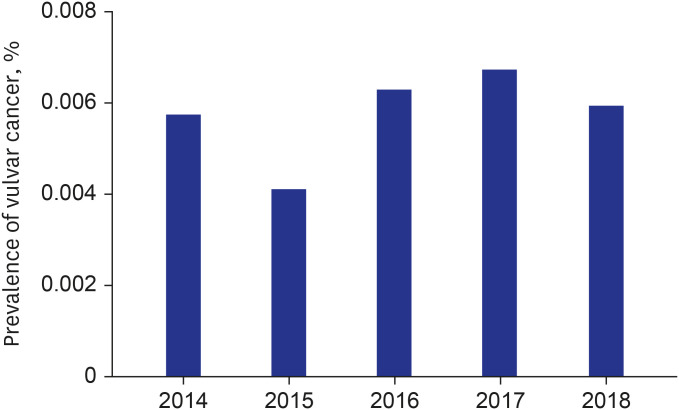
RESULTS
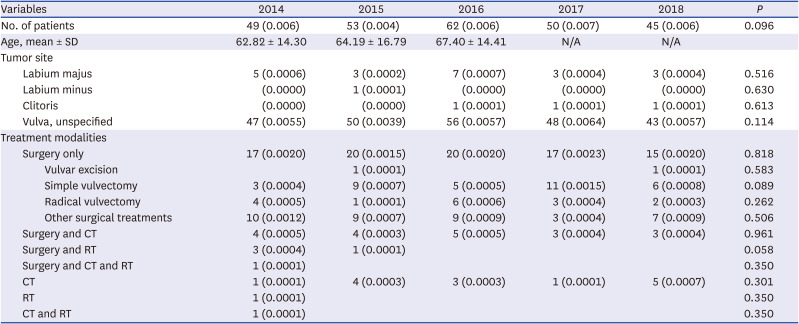
The HIRA-NIS database for 2014 to 2018 included records for 4,636,542 women, among whom 259 met the inclusion criteria for both diagnosis and treatment of vulvar cancer (Table 1). The number of cases (and prevalence) of vulvar cancer in each reporting year was 49 (0.006%) in 2014, 53 (0.004%) in 2015, 62 (0.006%) in 2016, 50 (0.007%) in 2017, and 45 (0.006%) in 2018. There were no significant differences between the annual prevalence of vulvar cancer during the study period (Fig. 1). The median (± SD) patient age at diagnosis of vulvar cancer was 62.82 (± 14.30) years in 2014, 64.19 (± 16.79) years in 2015, and 67.40 (± 14.41) years in 2016. Most patients in 2017 and 2018 were over 75 years of age, and the data were assessed only for that age group, and not by the age of individual patients (Supplementary Table 1). In terms of treatment modalities, the largest number of patients underwent surgery without chemotherapy or radiation therapy (0.0021% in 2014, 0.0016% in 2015, 0.0020% in 2016, 0.0023% in 2017, and 0.0021% in 2018). Patients who underwent both surgery and chemotherapy were the second most common until 2017 (0.0005% in 2014, 0.0003% in 2015, 0.0005% in 2016, and 0.0004% in 2017). In 2018, however, patients who underwent chemotherapy without surgery were the second most common occurrence (0.0007%). The numbers of patients who underwent each of the above treatment modalities for invasive vulvar cancer in each year did not differ significantly from 2014 to 2018.
Table 1
Characteristics of South Korean vulvar cancer patients from 2014 to 2018
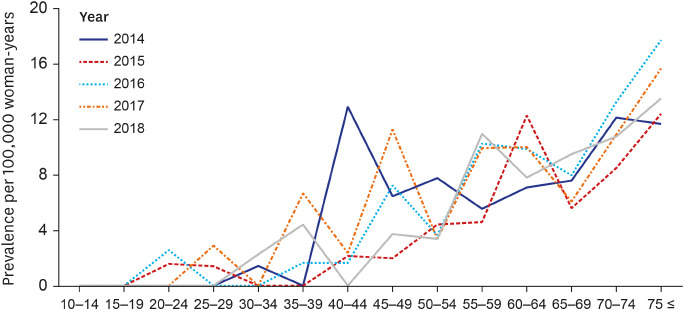
Analysis of the age-specific prevalence according to 10-year age increments indicated that vulvar cancer was most prevalent in women over 70 year of age, while it was the least prevalent in women less than 40 years of age (Table 2). The prevalence of vulvar cancer during study period stratified according to 5-year age increments were shown in Fig. 2.
Table 2
Distribution and comparison of age-specific prevalence rates of vulvar cancer from 2014 to 2018 stratified according to 10-year age increments

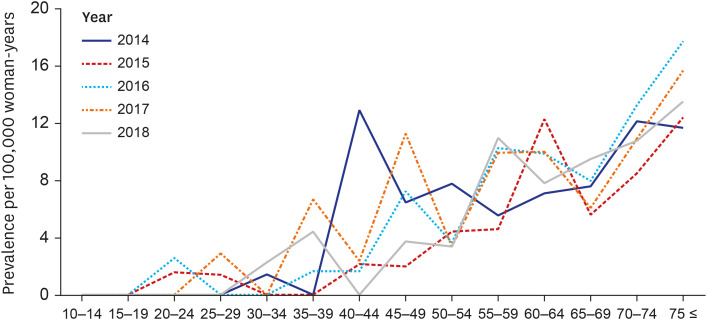
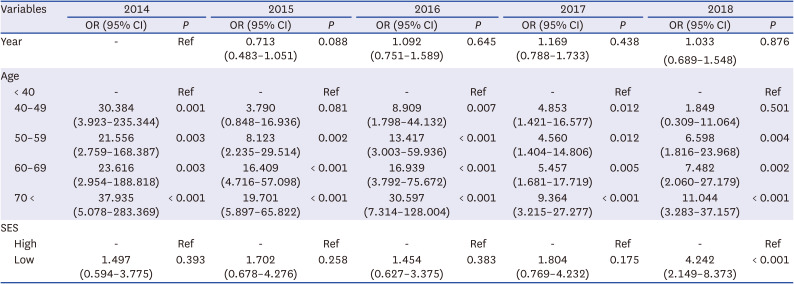
According to the logistic regression analyses, age was significantly correlated with prevalence of vulvar cancer (P < 0.05; Table 3). Compared to the annual prevalence of vulvar cancer in women less than 40 years of age, significantly greater prevalence was noted for almost all age groups. However, in 2015 and 2018, there were no significant differences between the prevalence of invasive vulvar cancer in women aged 40 to 49 compared with women under the age of 40 (P = 0.081 in 2015 and P = 0.501 in 2018). There was no significant change in the prevalence of vulvar cancer from 2015 to 2018 compared to that reported in 2014. Compared with women under 40 years of age, vulvar cancer was significantly more prevalent in women over 40 years of age, and especially among women over 70 years of age: the ORs were 37.935 in 2014, 19.701 in 2015, 30.597 in 2016, 9.364 in 2017, and 11.044 in 2018. Vulvar cancer was more prevalent in women with low SES compared to women with high SES in 2018 (OR, 4.242; P < 0.001); however, similar findings for the 2014 to 2017 years were not statistically significant.
Table 3
Multivariate logistic regression analyses of risk factors for vulvar cancer
DISCUSSION
We investigated trends in the prevalence of vulvar cancer among South Korean women of different age groups between 2014 and 2018. There was no increasing or decreasing trend in the prevalence of vulvar cancer over the study period, and no difference in the median age at diagnosis of vulvar cancer. The treatment modalities included surgery, chemotherapy, and radiotherapy, and the largest number of patients underwent only surgical treatment. There was no year-to-year difference in the choice of surgical methods or treatment modalities. When the data were stratified by 10-year age increments, the prevalence of vulvar cancer in each age group did not differ significantly from year to year. In addition, compared to women under 40 years of age, the prevalence of vulvar cancer was greater in women over 40 years of age, a finding that was consistent from 2014 to 2018. In the multivariate logistic regression analyses, there were no significant differences in the prevalence of vulvar cancer from 2015 to 2018 compared to 2014, and when compared with women less than 40 years of age, vulvar cancer was most prevalent age among women over 70 years of age. The women’s SES affected the prevalence of vulvar cancer only in 2018, in which year the prevalence of vulvar cancer was significantly greater in women of low SES than in those with high SES.
The data analyses for our study indicated no change in the prevalence of vulvar cancer from 2014 to 2018. According to the research on the incidence of gynecological cancer in a single institution in Korea from 1975 to 2000, vulvar cancer accounted for 0.9% of all gynecological cancers. However, this could not be representative of the national incidence, and the trends was not analyzed.12 A previous population-based study of the incidence of vulvar cancer in the United States6 and Norway13 reported the incidence of vulvar cancer was stable. In contrast, the age-standardized incidence rate for vulvar cancer trended upward from 1993 in Japan.3 Bodelon et al.2 also reported that the prevalence of vulvar cancer is increasing in all age groups, while a trend towards an increasing incidence of vulvar cancer among younger women has been reported in Denmark.14 According to a Dutch study,15 the prevalence of vulvar cancer was stable until 2002; thereafter, the prevalence rate increased by about 5% annually between 2002 and 2010. Considering that the prevalence of HPV among young Korean women has been increasing and the introduction of HPV vaccination has been delayed compared to Denmark and the Netherlands,161718 the incidence of vulvar cancer in young Korean women was expected to increase for the time being.
In this study the prevalence of vulvar cancer increased with age, and was most prevalent in women over 70. Our results indicating a greater prevalence of vulvar cancer in older patients are broadly comparable to the results of population-based studies in other countries.3514 Lichen sclerosus and differentiated vulvar intraepithelial neoplasia are risk factors for the development of vulvar cancer in elderly women.19 Although the decrease of prevalence in vulvar cancer in older women was not significant in our results, it was reported as a decreasing trend in previous study.15 It reflects that early diagnosis and treatment became easier clinically. Vulvar cancer has typically been associated with a relatively poor prognosis because it is usually diagnosed in older women and at an advanced stage.520 In addition, older women have higher mortality rates due to increased co-morbidities.21 However, since the incidence of vulvar cancer in older aged women has been gradually decreasing, the prognosis of vulvar cancer is expected to improve in South Korea.
Squamous cell carcinoma (SCC) accounts for 80% of all vulvar cancers, and 20% of them are related to HPV infection. The HPV-related type of SCC is associated with vulvar intraepithelial neoplasm (VIN) as a precursor lesion, and generally affects relatively younger women. Most SCCs are not related to HPV infection, and these occur in a relatively older age group, with lichen sclerosus as a common precancerous lesion.2223 In recent years, vulvar cancer has been increasing among European women under the age of 60,14 likely due to an increase in HPV infection in younger women, which is associated with changes in sexual habits and smoking. A similar trend is expected to be ongoing in South Korea.2425 In previous studies in Western countries, the analyses indicated women currently tended to have earlier first intercourse and more sexual partners during their lifetime than was previously reported.26 Furthermore, the number of women diagnosed with genital warts has increased over the last few decades.27 Genital warts are strongly associated with developing HPV-related malignancies including vulvar cancer.28 Although only 20% of all vulvar cancers are associated with HPV infection, HPV is considered a major cause of vulvar cancer in younger women. It is expected that the prevalence of HPV-related vulvar cancer will decrease in Korea due to the recent introduction of an HPV vaccine; however, the effect is not yet evident.
Lower SES is associated with HPV-related cancer, including vulvar cancer.2930 Our study showed that lower SES was associated with a greater prevalence of vulvar cancer in 2018, which is comparable to the findings of a previous study in Japan.3 In Japan, the prevalence of vulvar cancer decreased from 1979 to 1992,3 which may have been related to the rapid economic growth of Japan during that period. It has been postulated that women with lower SES, including lower levels of education and lower income, were more likely to have more frequent sexual activity or have delayed access to screening services. These characteristics are not limited to vulvar cancer but also other HPV-related carcinomas, including cancers of the cervix, vagina, and anus.303132 Nevertheless, from 2014 to 2017, there were no significant associations between the prevalence of vulvar cancer and SES in our study, possibly because various confounding factors other than HPV can affect the occurrence of vulvar cancer.
Treatment trends for vulvar cancer have changed over the past 30 years.33 About 30 years ago, radical vulvectomy with en bloc bilateral inguinofemoral lymphadenectomy was the standard surgical treatment. However, in recent years, the preferred surgical treatment method has gradually become more personalized,34 such that unilateral or bilateral inguinofemoral lymphadenectomy is typically executed by way of a separate incision with wide local excision. According to past domestic studies, it has been reported that radiotherapy alone could achieve excellent local control and less complications in vulvar cancer.35 Although there were no changes in the types of surgical procedures employed during our study period, previous studies have shown changes due to the introduction of less radical surgery.333637
There were several limitations of our study. First, it was impossible to obtain information on the patients’ medical history, so we could not analyze the risk factors for vulvar cancer except for age and SES. Second, because information regarding surgical procedures was obtained from the codes entered by the institutions, detailed surgical data could not be assessed. Third, due to the characteristics of the HIRA-NIS data, the patients’ long-term survival data could not be obtained, but should be studied in the future. Despite these limitations of our data, the major strengths of our analyses were the use of national population-based data. To our knowledge, our detailed analysis of prevalence by age group is the first such study investigating the prevalence and treatment of vulvar cancer over time in South Korea.
In conclusion, we assessed the prevalence and treatment of vulvar cancer among South Korean women from 2014 to 2018. There were no significant differences between the prevalence rates of vulvar cancer from 2015 to 2018, as compared to 2014; however, the prevalence of vulvar cancer was significantly greater in women over the age of 70. Considering the high prevalence rate in elderly South Korean women, strategies for targeted screening and management of vulvar cancer should be established. Our findings highlight the importance of domestic epidemiological data when developing policies to reduce the vulvar cancer in South Korea.
 XML Download
XML Download