

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Spinal dural arteriovenous fistulas (SDAVFs) are rare disease entities with an annual incidence of 5 to 10 cases per million, but they are the most common type of spinal vascular malformations [1]. Neurologic symptoms of SDAVFs are attributed to chronic venous congestion of the medulla [2]. The natural history is characterized by a progressive myelopathy, and 50% of untreated patients would be disabled 3 years after diagnosis [3].
The presenting symptoms include lower extremity weakness, gait difficulties, sensory disturbances and bowel/bladder disturbances when myelopathy develops. However, radiating pain or low back pain can be the sole presenting symptom without a focal neurologic deficit. These symptoms commonly lead clinicians to consider many other diagnoses before considering SDAVFs, especially radiculopathies [4]. Therefore, patients with undiagnosed SDAVFs may receive epidural steroid injections (ESI) for relieving low back pain, radiating pain or paresthesia.
In this study, we will present 4 cases of patients with SDAVFs who received lumbar steroid injection. The aims of this study were to review the result of treatment in these patients, and to suggest the possible contributing factor for acute paraplegia after lumbar steroid injection.
CASE REPORTS
Case 1
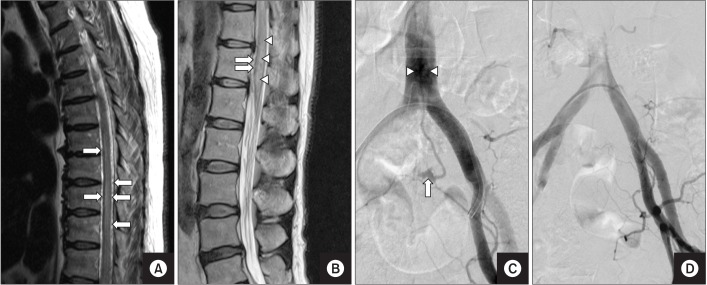
A 54-year-old male complained of paresthesia of both thighs for 1 year. He received transforaminal epidural steroid injection (TFESI) around/into bilateral L5 and S1 nerve roots under the impression of bilateral lumbosacral radiculopathies at his community hospital on January 10, 2015. At each site, a 5-mL mixture of dexamethasone (1.25 mg), lidocaine, bupivacaine, and normal saline was injected. After 8 hours, acute complete paraplegia occurred. On the next day (January 11, 2015), SDAVFs were revealed by magnetic resonance imaging (MRI) (Fig. 1A). Because his symptoms persisted after intravenous steroid therapy, he was transferred to our hospital on January 12, 2015. On physical examination performed in the emergency room, the strength of both lower extremities was 0/5 in the manual muscle test. During sensory evaluation, decreased light touch and pain sensations were identified below the bilateral T11 level. He experienced urinary and fecal incontinence. Contraction of the anal sphincter was absent. Careful history taking revealed a history of voiding difficulty (need for abdominal straining during voiding) for more than one year. While reviewing his initial MRI taken before TFESI (January 9, 2015), tortuous fluid void structures, which were missed before ESI, were noted above the L1 vertebral level (Fig. 1B). On spinal angiography, SDAVFs supplied by the right T6 intercostal artery were noted (Fig. 1C). After glue embolization of SDAVFs at the right T6 level, motor and sensory functions started to improve. On the day of discharge (February 24, 2015), the strength of both lower extremities was improved to 4/5–5/5. However, he was on intermittent catheterization as he could not self-void till that time. When he was followed up after 1 year, it was observed that gait disturbance and failure to void persisted.
Case 2
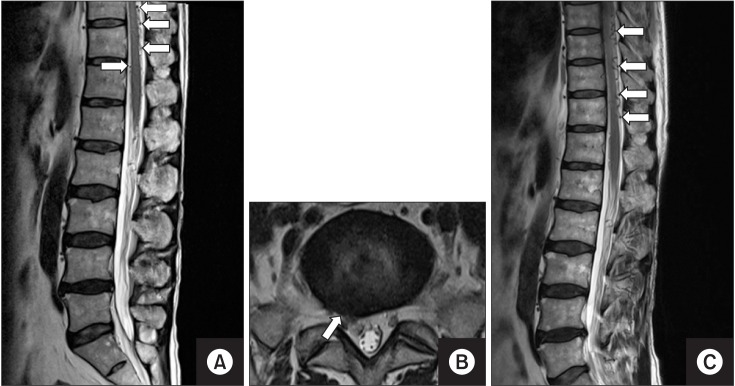
A 64-year-old female complained of low back pain and paresthesia of both lower extremities for 4 months. After caudal ESI of dexamethasone with an unknown total volume of injectate on August 30, 2011, acute complete paraplegia and failure to void developed. Because there was no improvement of symptoms after intravenous steroid pulse therapy, she was transferred to our hospital on September 1, 2011. On physical examination, the strength of both lower extremities was 0/5 in the manual muscle test. During sensory evaluation, the area below the bilateral L1 level was nearly insensitive to touch and pain. On MRI taken 2 days after the injection (September 1, 2011), SDAVFs were detected (Fig. 2A). On review of her initial MRI performed before the procedure (April 18, 2011), tortuous fluid void structures and increased spinal intensity of the spinal cord were noted, which were missed before ESI (Fig. 2B). On spinal angiography, SDAVFs supplied by the sacral branch of the left internal iliac artery were noted (Fig. 2C). After glue embolization of the feeding artery arising from the left internal iliac artery (Fig. 2D), sensory and motor deficits were gradually improved. On the day of discharge (September 13, 2011), the motor strength of lower extremities was 2/5–3/5 in the right leg and 4/5–5/5 in the left leg. When she was followed up after 3.5 years, it was observed that spastic paraplegic features persisted.
Case 3
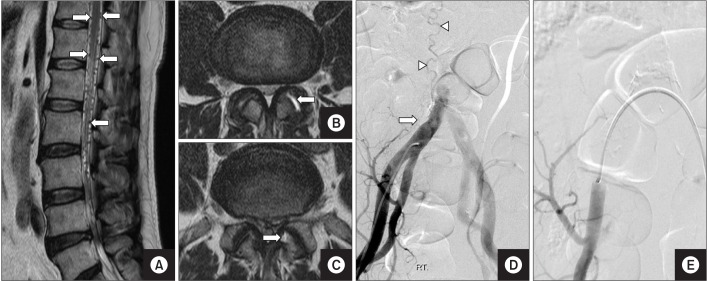
A 67-year-old male complained of radiating pain in the right lower extremity for 1 month. Although SDAVFs (Fig. 3A) as well as a herniated intervertebral disc (HIVD) at the right L5–S1 level (Fig. 3B) was detected on MRI on June 3, 2014, TFESI around/into the right S1 nerve root was performed twice on June 18, 2014 and July 9, 2014 under the impression of right S1 radiculopathy. At each time, a 3-mL mixture of dexamethasone (10 mg), ropivacaine, and normal saline was injected. After the injections, his radiating pain was relieved to a large degree and no weakness or paresthesia was seen. On the followup MRI performed on September 24, 2015 (Fig. 3C), SDAVFs persisted, and the extent of engorged perimedullary veins was similar to that in the previous MRI.
Case 4
A 50-year-old male complained of low back pain and radiating pain in the left buttock, posterior thigh, and calf for 2 weeks. SDAVFs (Fig. 4A) and degeneration of the left L3–4, and L4–5 facet joints (Fig. 4B, 4C) were revealed by MRI on January 19, 2015. He received facet joint injection into the left L3–4 and L4–5 on January 22, 2015. At each site, a 1.25-mL mixture of triamcinolone (10 mg), lidocaine, and normal saline was injected. After the injection, low back pain was relieved only for a while, and no weakness was noted. Spinal angiography showed SDAVFs supplied by the right internal iliac artery (Fig. 4D). After glue embolization of SDAVFs on January 30, 2015 (Fig. 4E), pain was relieved to a considerable degree.
DISCUSSION
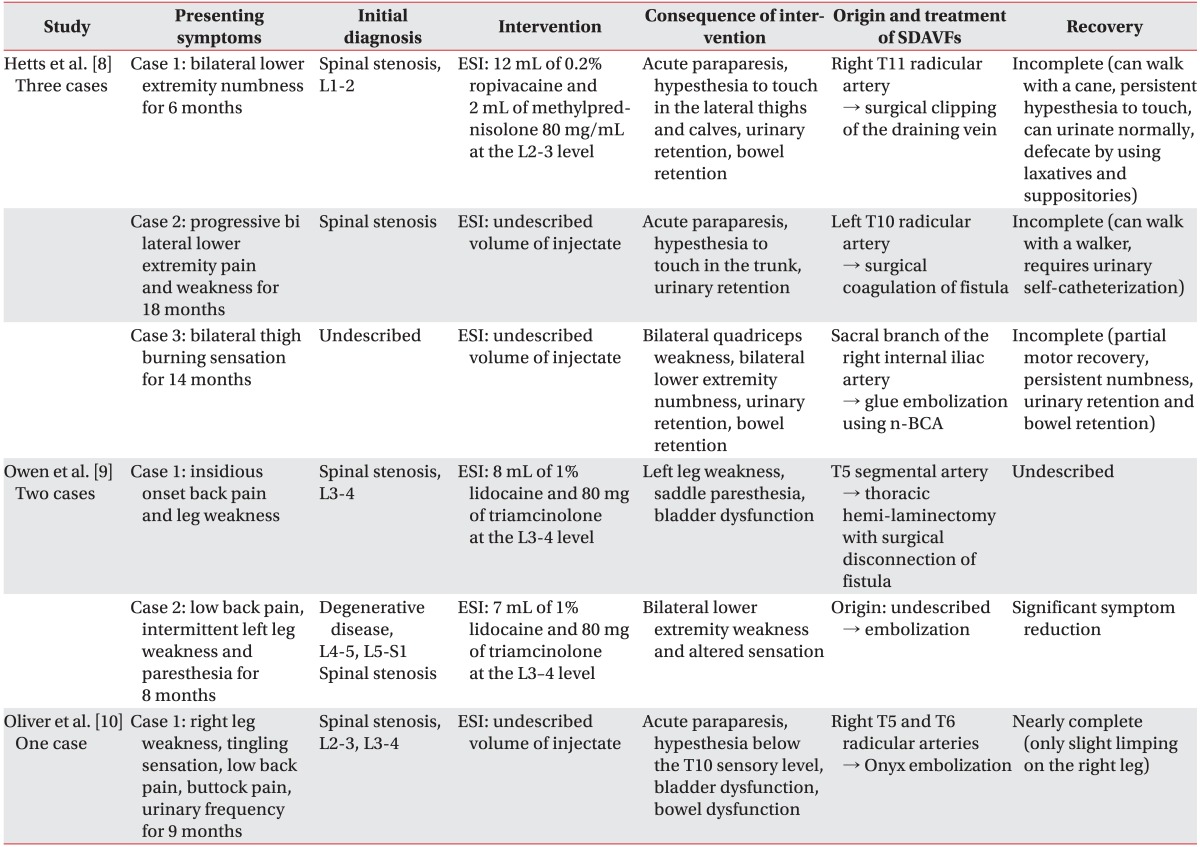
Several studies have demonstrated that arterialization of the spinal venous system plays a major role in the pathophysiology of SDAVFs. Because drainage of spinal venous blood is impaired due to diminished arteriovenous pressure gradient, venous congestion with intramedullary edema occurs. This congestion in turn leads to ischemia of the spinal cord. Generally, venous congestive edema occurs in a caudocranial direction due to relatively fewer venous channels in the lower spinal region compared with the cervical region. However, in a later stage, cranial portion of the spinal cord can also be involved [5]. Several previous reports have documented acute exacerbation of symptoms of SDAVFs in association with use of intravenous steroids [6], and oral steroids [7]. Also, there have been several reports of acute paraplegia after lumbar ESI [8910] (Table 1). Because patients with SDAVFs already have higher intradural and epidural pressure, injection of a relatively small volume of injectate including steroids into the epidural space can lead to aggravation of symptoms [8].
In our report, among the 4 cases of SDAVFs, acute paraplegia developed in 2 cases. The total volume of injectate was 20 mL in case 1, 3 mL in case 3, and 2.5 mL in case 4. Although the total volume of injectate in the second case is not known, considering the method of injection, namely caudal ESI, the volume would be at least 10 mL. In the report by Hetts et al. [8] among the 3 patients, total volume of injectate was 14 mL in one patient and it was not known in the other 2 patients. In the study by Owen et al. [9] when considering the usual concentration of triamcinolone (40 mg/mL), total volumes of injectate were 10 mL and 9 mL in 2 cases, respectively. Based on our cases and literature review, we could draw an analogy that the volume of injectate may be a contributing factor for acute paraplegia after lumbar ESI in patients with SDAVFs.
In cases 1 and 2, it might have been difficult to identify tortuous structures suggestive of SDAVFs as their initial MRI examinations only covered the lumbar spine area and the quality of images was not good. However, a careful review of the initial MRIs revealed tortuous signal-voided structures and increased spinal cord signal at the upper lumbar vertebral level on T2-weighted images. Since SDAVFs can be easily misdiagnosed as radiculopathy, and ESI for relieving radicular pain can cause serious adverse effects such as paraplegia, clinicians should always keep in mind the possibility of SDAVFs and review the MRI before ESI, especially when the symptoms of myelopathy coexist.
However, there is a limitation since the modes of injection and the types of corticosteroids vary among the cases presented in this report. Therefore, further studies are needed to examine the correlation between the volume of injectate and acute paraplegia, and also to explore other potential contributing factors.

 XML Download
XML Download