

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Complex regional pain syndrome (CRPS) is characterized by disproportionate pain, allodynia, vasomotor changes, decreased range of motion, hyperalgesia, edema, and skin temperature or color change [1]. In the past, it was called reflux sympathetic dystrophy in acknowledgement that it was primarily an abnormal sympathetic nervous reflex that was involved. However, both sympathetically maintained pain and sympathetically independent pain have been found to exist, and thus the name was ultimately changed to CRPS by the International Association for the Study of Pain (IASP) in 1994. CRPS is divided into type I and type II by absence or presence of peripheral nerve injury [12]; type II generally occurs more frequently, but type I occurs more frequently in stroke patients [3].
CRPS occurs in the affected limbs of stroke patients in the recovery phase. Prevalence differs widely according to diagnostic standards and methods [4] and has been reported to vary from 12.5% to 70% depending on clinical signs and symptoms [56]. CRPS onset time is known to be from 1 to 5 months after stroke, and if it is not treated properly, there is a high possibility of irreversible change [4].
The pathophysiology of CRPS is unclear, but it is usually considered a multifactorial disease with clinical features that range from abnormal reflection to tissue damage causes such as neurogenic inflammation, nociceptive sensitization, vasomotor dysfunction, and maladaptive neuroplasticity [7].
Diabetes mellitus (DM) is a multisystem disease characterized by persistent hyperglycemia that has both acute and chronic biochemical and anatomical sequelae [8]. Glycosylated hemoglobin A (HbA1c) is an index of blood glucose control, and it reflects the average blood glucose level for 2 to 3 months [910]. Normal HbA1c is below 6%, but it exceeds 6% in diabetes and can increase up to 10%–12% [11].
A number of studies have reported that CRPS is one of the musculoskeletal complications in patients with DM [81213], but there are no studies on the relationship between HbA1c and CRPS prevalence. Thus, the purpose of this study was to investigate the relationship between HbA1c and CRPS prevalence in stroke patients with diabetes and to understand how uncontrolled hyperglycemia can affect CRPS occurrence in these patients.
MATERIALS AND METHODS
Subjects
We retrospectively reviewed the medical records of 331 patients who had been admitted to Jesus Hospital (Presbyterian Medical Center) from January 2012 to December 2013. The inclusion criteria for the study were (1) stroke confirmed through either cerebral infarction or cerebral hemorrhage and (2) a diagnosis of diabetes. The following were the exclusion criteria for this study: history of injury in an upper extremity, hyperthyroidism, hyperparathyroidism, peripheral neuropathy (including from diabetes), or previous CRPS.
Methods
Diagnosis of CRPS
The patients were diagnosed using the IASP's proposed revised CRPS clinical diagnostic criteria [14] and diagnosed by a physician in the Department of Nuclear Medicine based on a three-phase bone scan (TPBS) [15]. We divided the patients into two groups, with or without CRPS, and compared them by age, gender, stroke lesion, DM duration, HbA1c (%), National Institutes of Health Stroke Scale (NIHSS) score, affected shoulder flexor muscle strength, Fugl-Meyer Assessment (FMA) score, motricity index (MI), Functional Independence Measure (FIM), Korean version of Modified Barthel Index (K-MBI) score, blood glucose level on admission day, duration from stroke onset to HbA1c check, and duration from stroke onset to the TPBS for CRPS diagnosis (Fig. 1).
HbA1c
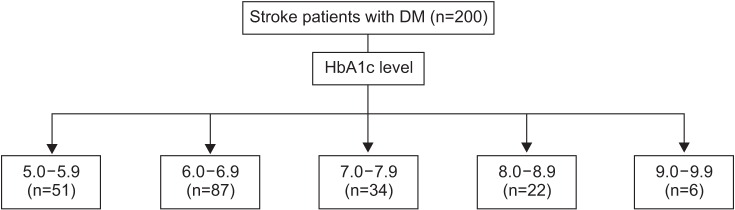
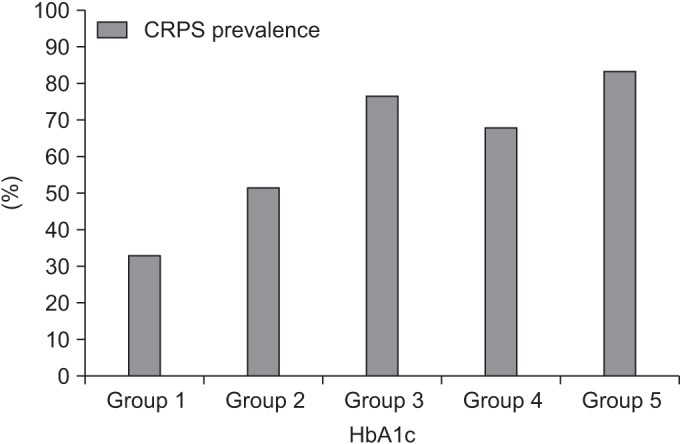
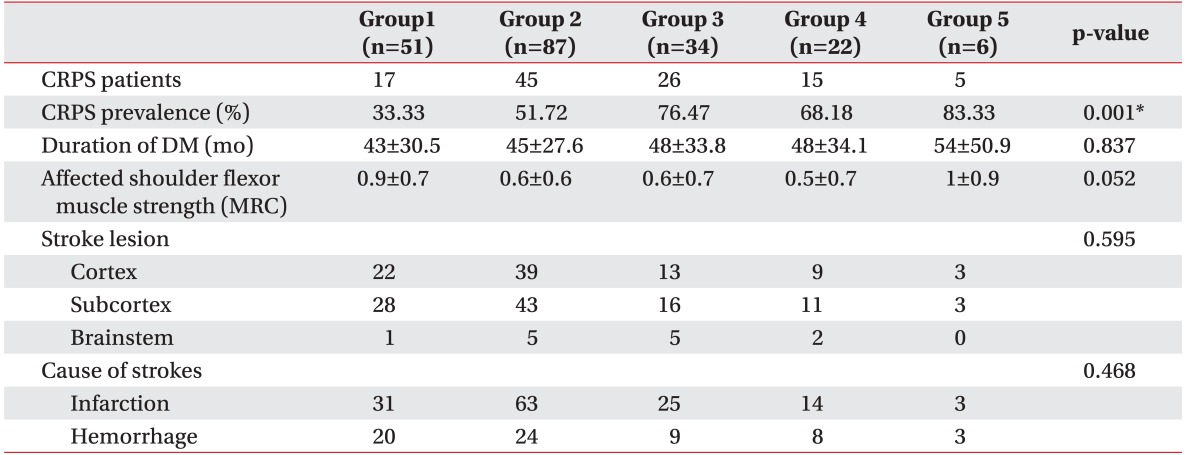
Among the 200 stroke patients with DM, we classified them into five groups by HbA1c value: group 1, 5.0%–5.9%; group 2, 6.0%–6.9%; group 3, 7.0%–7.9%; group 4, 8.0%–8.9%; and group 5, 9.0%–9.9%. Specifically, we compared the CRPS prevalence in each HbA1c group (Fig. 2).
Statistical analysis
Statistical analyses were performed using SPSS ver. 20.0 (IBM SPSS Inc., Armonk, NY, USA). We conducted independent t-tests to compare the CRPS and non-CRPS groups and chi-squared tests to compare CRPS prevalence in the five HbA1C groups. Statistical significance was set at p<0.05 for both sets of tests.
RESULTS
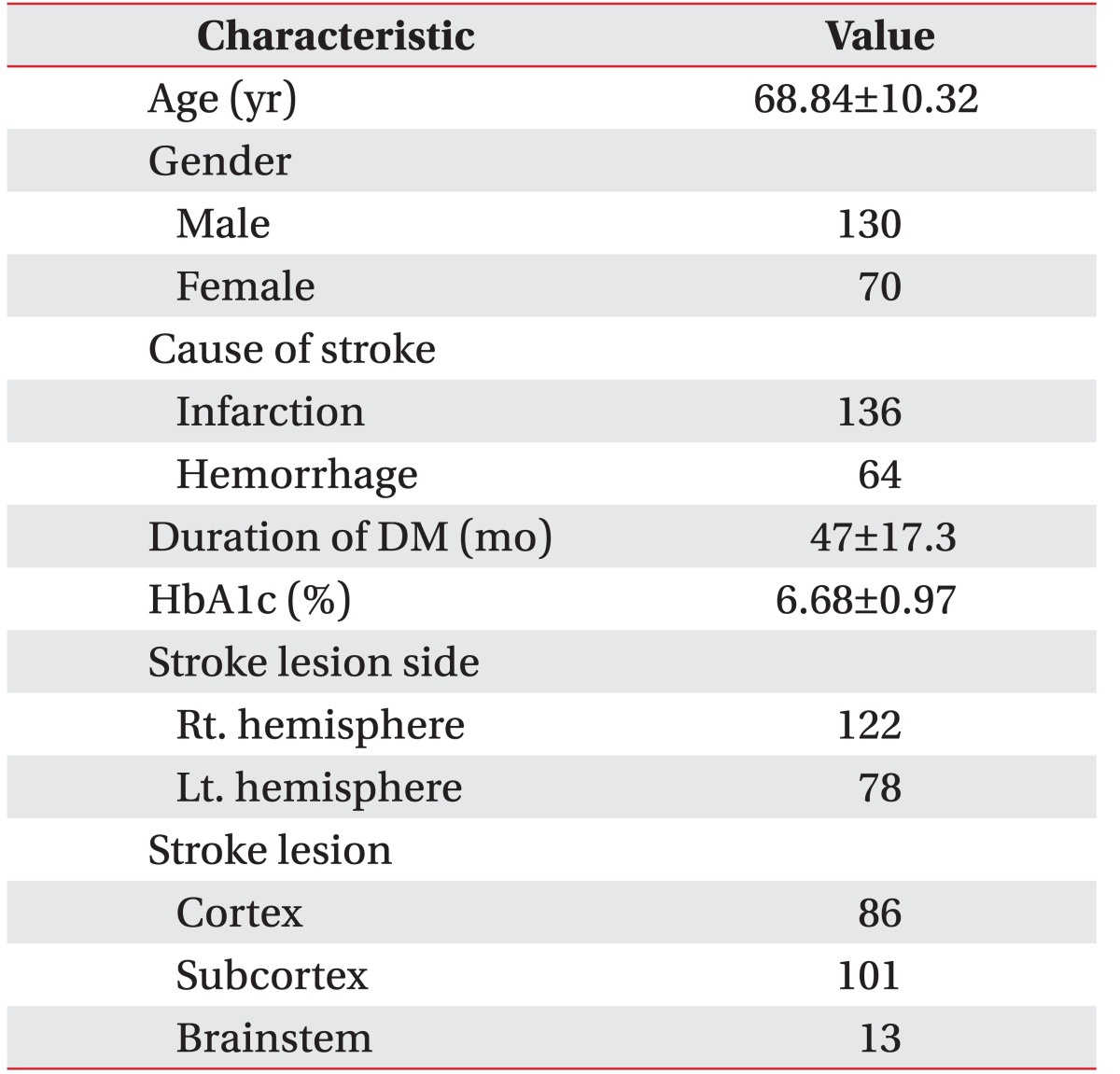
We analyzed the data from a total of 200 stroke patients with DM, 130 males and 70 females; mean patient age was 68.84±10.32 years. The patients comprised 136 with cerebral infarction and 64 with hemorrhagic stroke; mean DM duration was 47±17.3 months and mean HbA1c was 6.68±0.97% (Table 1).
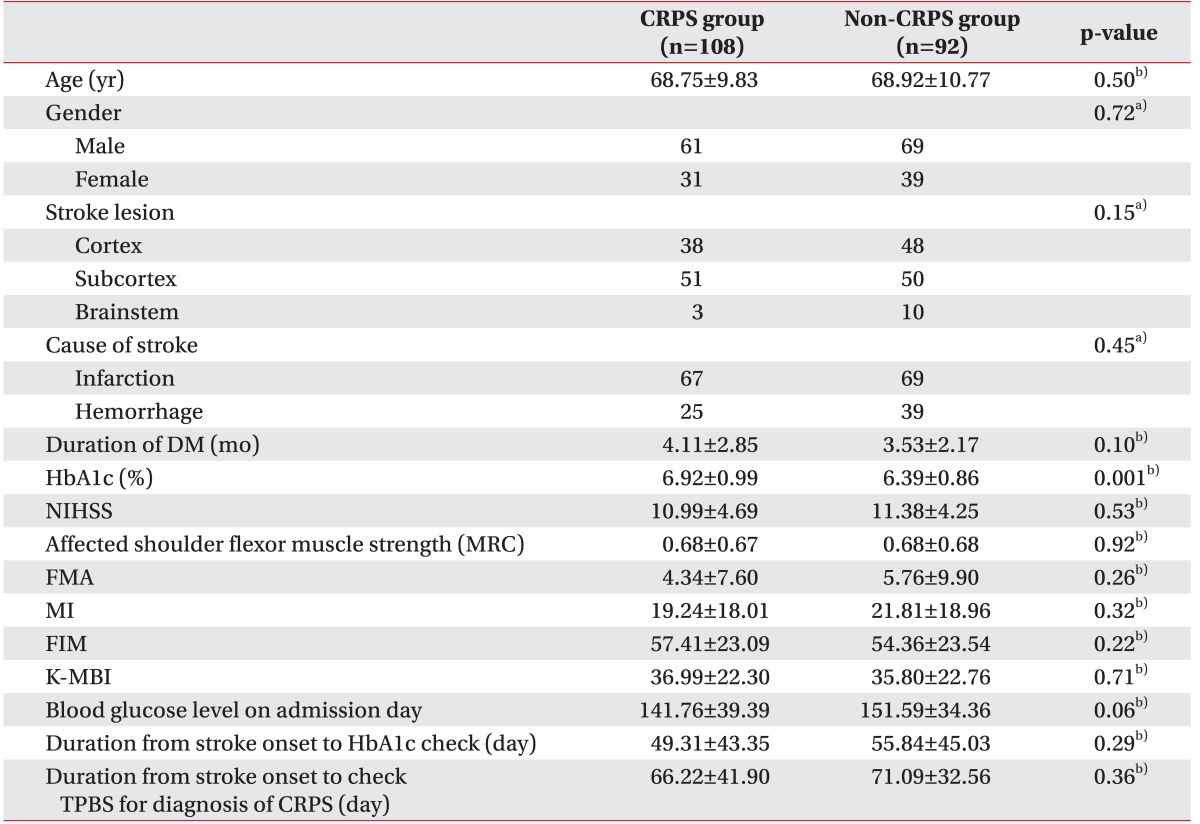
One hundred eight of the 200 subjects were diagnosed with CRPS, with the remaining 92 comprising the non-CRPS group. There were significant differences in HbA1c (p<0.05) but no significant differences between the CRPS groups in age, gender, stroke lesion, cause of stroke, DM duration, NIHSS score, affected shoulder flexor muscle strength, FMA score, MI, FIM, K-MBI score, blood glucose level duration from stroke onset to HbA1c check, or duration from stroke onset to the TPBS for CRPS diagnosis (p>0.05) (Table 2).
DISCUSSION
DM is considered highly related to CRPS occurrence [81213], and thus we attempted to investigate how uncontrolled hyperglycemia can affect CRPS occurrence in stroke patients with diabetes by analyzing the relationship between HbA1c and CRPS prevalence in these patients. In this study, as HbA1c values increased, CRPS prevalence increased as well, and thus we consider that maintaining adequate blood glucose levels is important for reducing CRPS occurrence in stroke patients with diabetes.
CRPS is characterized by severe pain, allodynia, hyperalgesia, and motor and autonomic signs and symptoms [7]. With regard to the pain itself, Calder et al. [16] and Van der Laan and Goris [17] reported that inflammatory response is the primary pain mechanism in CRPS patients. In addition, the activation of skin nociceptor that we can see in these patients induces retrograde depolarization of primary afferent nerves with small diameters, increasing the secretion of neuropeptides such as substance P and calcitonin gene-related peptide (CGRP) in the sensory endings of the skin [18]. These neuropeptides evoke vasodilatation and protein extravasations in the tissue, and the resulting signs such as reddening, warming, and edema are called neurogenic inflammation [18]; most inflammatory changes from CRPS are mediated by CGRP and substance P. Serum concentrations of both of these substances are higher in CRPS patients than in healthy control individuals [1920].
The concentrations of cytokines also show differences. In skin biopsy results, the concentrations of tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) were much higher in upper extremities affected by CRPS than in normal upper extremities [2122]. In early-stage CRPS (3 months on average), water-soluble TNF receptor and pro-inflammatory cytokines (TNF), IL-1, and IL-8 increased in blood serum whereas anti-inflammatory cytokines (IL-4, IL-10, and transforming growth factor-beta1 [TGF-β1]) decreased [2324]. It was reported that these pro-inflammatory cytokines caused sensitization and hyperalgesia [25], which indicates that neurological inflammatory response plays an important role in the occurrence of CRPS.
Type 2 diabetes mellitus (T2DM) is an inflammatory disorder that develops when there is a pathologic problem in the immune system [26], and it features high blood concentrations of congenital immune mediators due to the occurrence of pathologic consequences [927]. It has been reported that compared with control groups, the serum levels of pro-inflammatory cytokines (IL-1β, IL-6 and TNF-α), sialic acid and C-reactive protein, and malondialdehyde were significantly higher in T2DM patients [92627282930313233]. As glycemic control in these patients worsens (HbA1c >6.5%), serum TNF-α appears to increase proportionally [28].
These secretions of pro-inflammatory cytokines in diabetes play an important role and could be associated with neurogenic inflammation and vasomotor dysfunction in CRPS. Classically, CRPS is subdivided into three phases (acute, atrophic, and dystrophic). Among these, the primary acute inflammatory phase can last for weeks up to 6 months and is characterized by painful range of motion, edema, warmth, and erythema of the hand and wrist [34353637]. Therefore, we consider that worsening glycemic control is associated with the acute inflammatory phase of CRPS.
According to the result of this study, the higher the HbA1c in stroke patients with diabetes, the higher their CRPS prevalence. HbA1c values reflect hyperglycemia, during which pro-inflammatory cytokines and acute-phase reactive proteins increase, resulting in increased neuroinflammatory reactions and CRPS.
However, our study was limited by a number of important factors. The study was cross-sectional and thus it was limited to inferring causal relationships. Second, shoulder joint subluxation, which is known a factor in CRPS occurrence, was not included in the study; instead we substituted shoulder muscle flexor strength and motricity index, neither of which controlled for the shoulder subluxation. Finally, the number of CRPS patients was small for the comparison between CRPS prevalence and HbA1c. These limitations suggest possible directions for future study. Furthermore, long-term follow-up research on the relationship between decreased HbA1c and improved CRPS is considered necessary. Then, we can suggest physiological grounds for any causal relationships between blood glucose level and CRPS through studies about improved CRPS symptoms or reduced absorption ratio on TPBS with lower HbA1c.
In this study, we concluded that uncontrolled hyperglycemia is related to CRPS occurrence in stroke patients with DM by comparing their HbA1c values with their CRPS prevalence; because CRPS prevalence increased as HbA1c increased, we considered that uncontrolled hyperglycemia affects CRPS occurrence. Therefore, it is necessary to maintain adequate blood glucose control in stroke patients with diabetes in addition to providing range of motion exercises and medical, physical, and occupational therapy.

 XML Download
XML Download