

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Congenital muscular torticollis (CMT) is considered as a neck deformity that involves contracture of the sternocleidomastoid (SCM) muscle. The characteristic clinical features of CMT include ipsilateral tilt of head, contralateral rotation of the face and chin, and palpable neck mass [123].
The initial treatment for CMT is physical therapy, including manual stretching exercise and massage. More than 90% of the infants with CMT reach full recovery through physical therapy. Contracture of the SCM muscle can persist despite physical therapy, with consequent craniofacial asymmetry, plagiocephaly, or scoliosis. In refractory cases, surgical intervention may also be indicated [456789].
Conventional B-mode ultrasonography has been used widely for diagnosing mass within the SCM muscle in infants with CMT. Muscle thickness, echogenicity, and transverse and longitudinal extents of involvement are evaluated by conventional B-mode ultrasonography. Many researchers have studied the correlation between the B-mode finding of SCM muscle and treatment duration to investigate the rehabilitation outcomes in infants with CMT. Nevertheless, the results from the previous studies have been inconsistent [9101112].
Sonoelastography has recently been used for evaluating tissue stiffness in real-time. This imaging technique is based on the principle that tissue compression induces strain (displacement) within the tissue and the strain is smaller in harder tissue than in softer tissue [1314].
In this study, we investigated whether the sonoelastography would be beneficial for predicting the outcomes of treatments in infants with CMT.
Go to : 
MATERIALS AND METHODS
We investigated the medical record of 215 infants clinically diagnosed with CMT from January 2013 to December 2014. Inclusion criteria were as follows: 1) infants diagnosed as CMT with a palpable neck mass before 3 months of age, 2) infants evaluated initially by both B-mode ultrasonography and sonoelastography, 3) infants who had received conservative treatment after being diagnosed with CMT. Exclusion criteria were as follows: 1) infants with neurodevelopmental disorders, 2) congenital anomalies of the cervical spine, 3) spasmodic, neurogenic and ocular torticollis, and 4) infants lost to follow-up.
We obtained the data as follows: age at diagnosis, sex, affected side, thickness of SCM muscles and ratio of SCM muscle thickness on the affected to unaffected side (A/U ratio) in B-mode imaging, strain ratio of SCM muscles in sonoelastogram, and treatment duration.
B-mode ultrasonography and sonoelastography were performed by an experienced musculoskeletal radiologist using the Philips iU 22 ultrasound system (Philips Health Care, Andover, MA, USA) with an L12-5 linear transducer. Neck ultrasonography was conducted on infants in supine position following rotation of their head to the opposite side. Both transverse and longitudinal views of the SCM muscle were obtained from conventional B-mode imaging. After B-mode ultrasonographic assessment, the same radiologist conducted sonoelastographic evaluation of the SCM muscle in the transverse and longitudinal views. The force applied to neck with the probe was adjusted in accordance with the indicator on the monitor, which presented optimal strain within the region of interest (ROI) in the color-coded image. The ultrasound images were transferred to a picture archive and communication system and the results were subsequently read by the same radiologist. The affected and unaffected SCM muscles' thickness and the distance from the most superficial to the deepest aponeuroses in the thickest region of the SCM muscle from the transverse view were measured (Fig. 1). For color-coded image in sonoelastogram, the relative stiffness of the neck tissue was represented by the colors ranging from red (soft, high elasticity) to blue (hard, low elasticity) within a continuous spectrum. Strain ratio is the relative stiffness of the SCM muscle compared to that of the subcutaneous tissue. A circular ROI was placed onto the subcutaneous fat layer as reference region and another circular ROI was placed on the SCM muscle in the transverse view. The strain ratio between both the ROIs was calculated automatically by the built-in software in the ultrasound system, which divided the ROI of the subcutaneous tissue by the ROI of the muscle [15] (Fig. 2). The higher value of the strain ratio indicates less elasticity of the tissues.
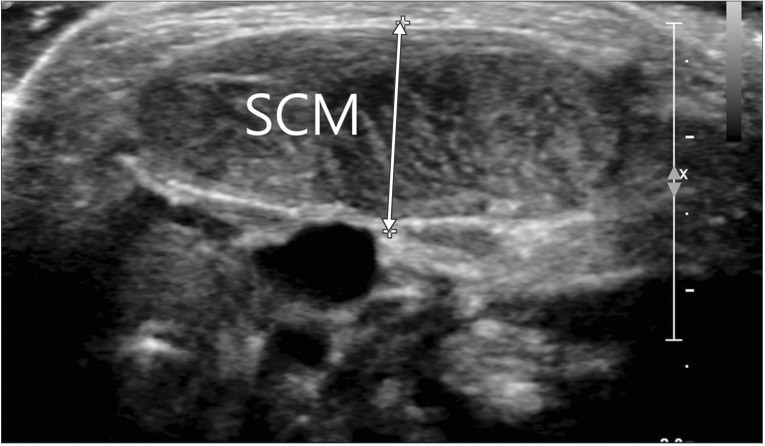 | Fig. 1Transverse view of the sternocleidomastoid (SCM) muscle in B-mode ultrasonogram. White arrow indicates thickness of the SCM muscle.
|
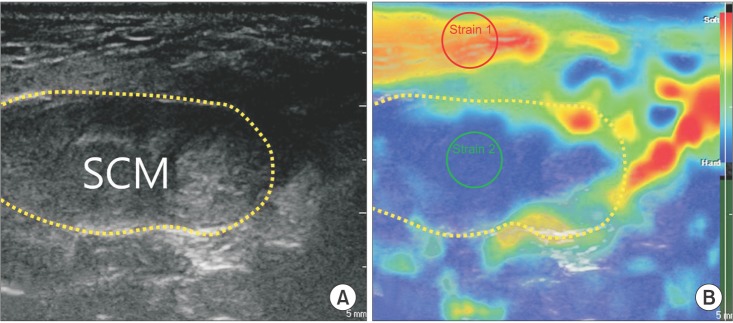 | Fig. 2Transverse view of sternocleidomastoid (SCM) muscle in B-mode ultrasonogram (A) and sonoelastogram (B). Each yellow dotted circle is the cross-sectional area of SCM muscle. In sonoelastogram (B), the colors ranging from red (soft) to blue (hard) represent relative stiffness of the tissue. Red circle (strain 1) indicates region of interest (ROI) of subcutaneous tissue (reference tissue), and green circle (strain 2) is ROI of SCM muscle.
|
For conservative treatment, manual stretching and massage on the affected SCM muscle were performed twice a week for 30 minutes by a specialized physical therapist. In addition, home exercise was performed with the infants' parents. When differences between both sides in the range of motion (ROM) of cervical rotation and side-bending were <5°, the treatment was regarded as successful, and physical therapy was discontinued. Cervical ROM was measured with a Baseline 12-1076 arthrodial goniometer (Fabrication Enterprises, White plains, NY, USA) on infants in supine position. The ROM of cervical rotation was measured by rotating the infants' head to both sides, and the ROM of cervical side-bending was determined by measuring the deviated degree from neutral position. Treatment duration was defined as the period between the first visit day and the last day of physical therapy.
Statistical analysis was performed using the SPSS ver. 20.0 software program (IBM SPSS Inc., Armonk, NY, USA). Difference in muscle thickness and strain ratio between right and left SCM muscles was evaluated by Wilcoxon signed rank test. The Spearman correlation test was used to assess the correlation between treatment duration and the following factors: SCM muscle thickness, A/U ratio, and strain ratio. A p-value of <0.05 was regarded as statistical significance.
The study was approved by the Institutional Review Board and informed parental consent was waived due to the characteristic of retrospective study.
Go to :
RESULTS
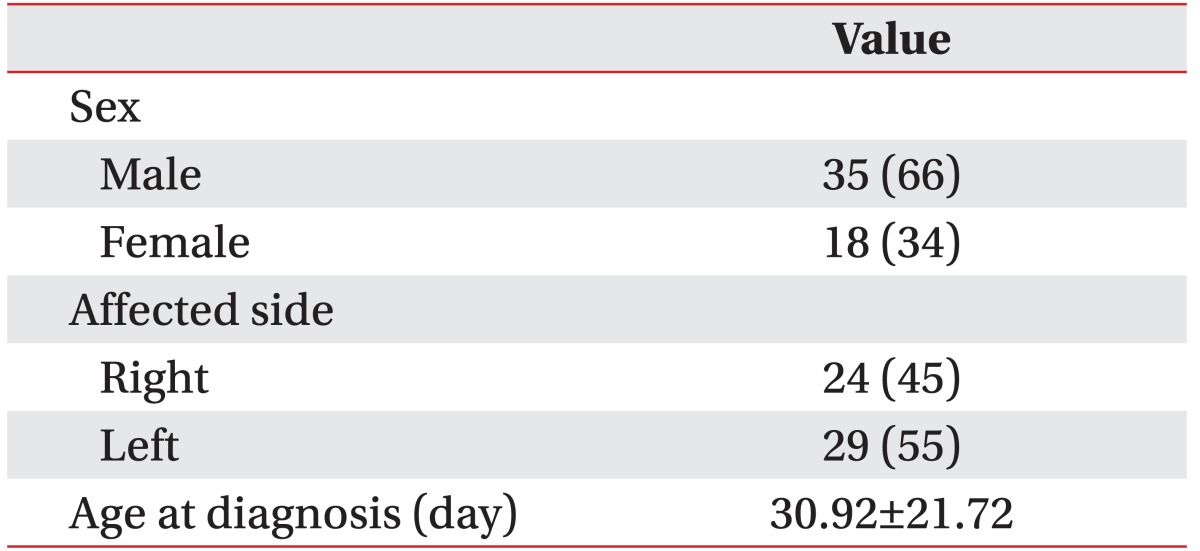
Among the 215 infants, 53 (35 males and 18 females) were enrolled in the study. The mean age at diagnosis was 30.92±21.72 days. Twenty-four infants were affected to right side, and 29 infants were affected to left side (Table 1).
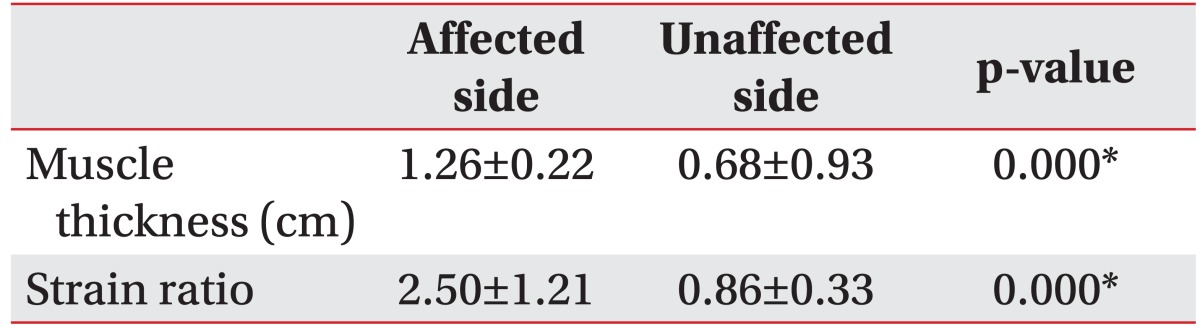
Mean thickness of the affected SCM muscle was 1.26±0.22 cm, and that of the unaffected SCM muscle was 0.86±0.33 cm. A/U ratio was 1.88±0.43. In strain ratio, the affected side was 2.50±1.21, and the unaffected side was 0.86±0.33. Both the thickness and the strain ratio of the affected SCM muscle were significantly greater than those of the unaffected SCM muscle (p<0.001) (Table 2).
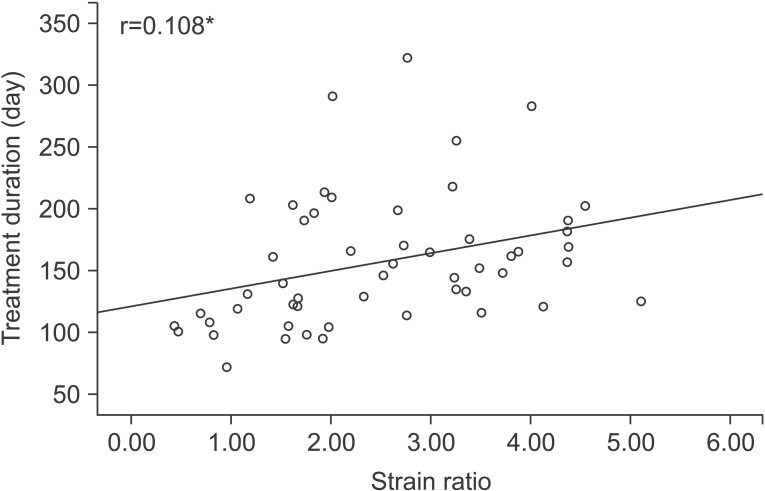
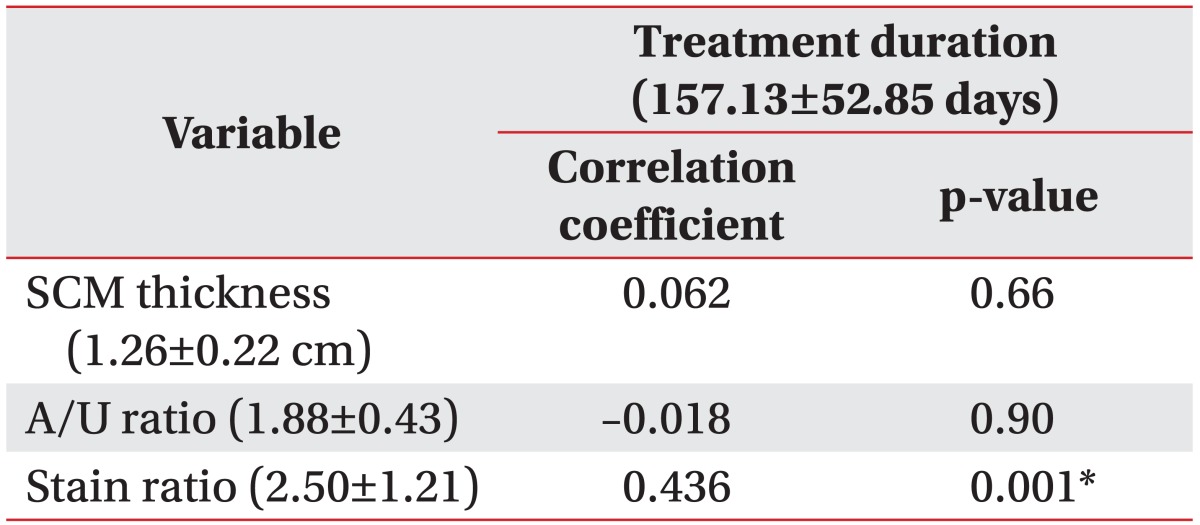
The treatment duration ranged from 72 to 322 days (mean duration, 157.13±52.85 days). The thickness of the affected SCM muscle as well as the A/U ratio did not show significant correlation with the treatment duration (p=0.66, p=0.90). The strain ratio of the affected SCM muscle was significantly correlated with treatment duration (p=0.001) (Table 3, Fig. 3).
Go to :
DISCUSSION
Many researchers have studied the relationship between rehabilitation outcome and variables associated with SCM muscle in B-mode ultrasonography. Some studies have correlated thickness of SCM muscle with treatment duration, whereas the results of some studies have been inconclusive. Jung et al. [10] reported that the thickness of the SCM and A/U ratio showed significant correlation with the treatment duration. Han et al. [11] demonstrated that the treatment duration was not affected by the thickness of SCM muscle, while A/U ratio affects the treatment duration. Lee et al. [9] founded that both the thickness of SCM muscle and A/U ratio did not significantly correlate with the treatment duration. In this study, both SCM muscle thickness and A/U ratio were not related to treatment duration. Han et al. [11] reported that the relationship between SCM muscle thickness and rehabilitation outcome in infants with CMT is inconsistent, because thickness of the SCM muscle can be influenced by development and age.
The cause of CMT is considered as contracture due to fibrosis of SCM muscle. In histologic studies, resected surgical specimens of SCM muscle have demonstrated fibrosis of muscle fibers, and the basic abnormality is known as endomysial fibrosis caused by migration of fibroblasts and deposition of collagen around individual muscle fibers [161718].
Sonoelastography is a recently developed technique for evaluating tissue elasticity in real time. This technique has been applied based on the pathogenesis associated with tissue stiffness in various musculoskeletal disorders. Drakonaki and Allen [19] reported that sonoelastography could be used for evaluating the change of muscle stiffness in congenital muscular dystrophy. Sconfienza et al. [20] reported that in patient with plantar fasciitis, sonoelastography increases diagnosis with B-mode ultrasonography, and assists in cases of equivocal B-mode ultrasonographic findings. Klauser et al. [21] reported that sonoelastography is useful for predicting the histopathological degeneration in Achilles tendinosis.
While there have been studies on the application of sonoelastography in infants with CMT, they have been limited in number and method. Lee et al. [22] studied the role of sonoelastography for diagnosing CMT by using a scoring system based on colors in the color-coded image of sonoelastogram. They reported that SCM muscle in infants with CMT had lower elasticity, as compared with normal SCM muscle, and sonoelastography could differentiate a subtle change of echogenicity on B-mode image. Kwon and Park [23] evaluated the role of sonoelastography for predicting the outcomes of rehabilitation in infants with CMT by using a scoring system based on colors and intensity of pixels in the color-coded image of sonoelastogram. In their study, the infants with CMT were divided into 2 groups based on findings of both Bmode image and sonoelastogram, and the results indicated that both thicker mass in B-mode image and higher scoring and intensity of pixels in sonoelastogram had poorer treatment outcome.
Sonoelastography can be conducted along with the B-mode ultrasonography, which is useful for evaluating mass of SCM muscle. In our study, we aimed to determine the factor that correlated with rehabilitation outcome of infants with CMT, using sonoelastography as an adjuvant tool to B-mode ultrasonography. We evaluated stiffness of SCM muscle in infants with CMT by using strain ratio, the semi-quantitative ratio scale instead of the scoring system. This study indicated that the affected SCM muscle in infants with CMT had lower elasticity than unaffected SCM muscle, and the SCM muscle with lower elasticity had longer treatment duration in infants with CMT. This is the first study that evaluated the direct relationship between elasticity of SCM muscle and treatment duration in infants with CMT. Therefore, sonoelastography ancillary to B-mode image provides more information for planning the diagnostic and treatment strategy in infants with CMT.
This study had a few limitations, including the small number of infants and retrospective design. Furthermore, ultrasonographic measurement was conducted by a single operator without evaluating inter-rater reliability.
In conclusion, sonoelastography may be a useful adjunctive tool to B-mode ultrasonography for evaluating infants with CMT, especially when predicting the rehabilitation outcomes of infants with CMT.
Go to :
 XML Download
XML Download