

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Many factors have been known as predictors for functional outcome of stroke, including age, stroke mechanism, volume and location of lesion, and comorbidities [123]. Recent studies have focused on the association between cognition and functional status in later life in the normal population [456] and in patients with cognitive impairment such as dementia, schizophrenia or multiple sclerosis [789]. In patients with dementia, schizophrenia or multiple sclerosis, cognitive assessment predicts functional outcome and justifies intervention for cognitive deficits [789101112]. Findings from these studies suggest that cognition has functional implication and can predict functional outcomes in various diseases including stroke.
Cognitive problems such as memory impairment, dyspraxia, deficit of attention, and impaired executive function are frequently observed in patients with stroke [131415]. The association between early post-stroke cognitive deficit and functional outcome has been reported [161718], however, studies on the independent predictive strength of early cognitive function are scarce [1920]. Nys et al. [19] showed that the prediction of long-term functional outcome improved when specific cognitive deficits such as inattention or visual perceptual disorders assessed by broad spectrum of neuropsychological tests in the acute stage of stroke, were added to a model with standard medical variables. Wagle et al. [20] demonstrated that early post-stroke cognitive functioning assessed by the repeatable battery of neuropsychological status is an independent predictor of 13 months' functional outcome. Most of the previous studies that examined the relationship between cognitive function in the acute stage after stroke and long-term outcomes, used global screening measures, such as Mini-Mental Status Examination (MMSE) and Raven's Colored Progressive Matrix (RCPM) [212223]. These screening tests are not expected to be sensitive enough to detect cognitive impairment in patients with stroke, nor precisely identify the domain and severity of cognitive deficits [24]. Considering the complexity of cognitive function, detailed neuropsychological evaluation tools covering different cognitive domains would be necessary to understand the cognitive function in early stage of stroke as an independent predictor for long-term functional outcomes.
The main purpose of this study was to investigate whether cognitive function assessed by domain-specific neuropsychological tests in the acute stage can have prognostic value in predicting functional outcome after stroke.
MATERIALS AND METHODS
Participants
We reviewed medical records of patients with first-ever stroke who received an inpatient care in the Department of Rehabilitation Medicine in Seoul National University Boramae Medical Center from January 2011 to April 2014. Patients who underwent neuropsychological evaluation within 4 weeks were included. Exclusion criteria were 1) recurred stroke, 2) previous history of psychiatric problems (e.g., depression, drug or alcohol abuse), 3) previous history of traumatic brain injury or degenerative brain disease, 4) other causes of disabilities (amputation, bedridden due to medical conditions, etc.), 5) noncommunicable status (e.g., aphasia), and 6) hemineglect. All subjects in this study participated in a comprehensive in-patient rehabilitation program consisting of a combination of physical and occupational therapy for a total of 1.5–2 hours per day, 5 days per week. Fourteen out of 40 subjects were on cognitive enhancing drugs. The mean length of stay in the department of rehabilitation medicine was 21.12±6.88 days.
Predictor variables
Demographic and stroke-related factors such as age, sex, type of stroke (infarction or hemorrhage), hemiplegic side (right, left, or bilateral) and the presence or absence of seizure were obtained as candidate predictor variables. Korean version of the Modified Barthel Index (K-MBI), National Institutes of Health Stroke Scale (NIHSS), Fugl-Meyer scale of affected side (FMSA), manual motor test at knee extensor muscles in the affected side (KEA), MMSE and domain-specific cognitive function in the acute stage of stroke were also included as candidate predictor variables. As only 31 subjects were evaluated with NIHSS in the emergency room, we adopted the NIHSS score, which was assessed on their day of transfer to the Department of Rehabilitation Medicine.
Cognitive function was evaluated with several domainspecific cognitive evaluations such as the Boston Naming Test (BNT), the construction praxis test (CPT), the construction recall test (CRT), and the verbal fluency test (VFT). They were selected for the evaluation of speech and language, visuospatial construction ability, visuospatial memory, and executive function individually.
The CPT consists of 4 figures, which are circle, diamond, overlapping rectangles and Necker cube; and the subject is questioned to recall those figures 2 to 2.5 minutes later in the CRT. For the VFT, participants are required to say as many words as possible from a category in 60 seconds. We also used 15-item version of the BNT. The validity of the Korean version of these tests is well-demonstrated and a normative data of each test is reportedly widely utilized in the diagnosis of dementia in Korea [25]. Raw scores obtained from 4 neuropsychological tests were transformed to the z-score, which is age- and education-adjusted value in the general Korean population. The z-score lower than –1.65 was selected for descriptive reports of severe cognitive impairment.
Outcome measures
Functional outcome was assessed with two separate measures: the recovery of K-MBI during the first 3 months ('functional improvement') and modified Rankin Scale (mRS) at post-stroke 6 months ('functional status'). The scores of K-MBI at post-stroke 6 months were not included in the analysis, as many of them were missing. To measure the functional improvement at 3 months after stroke, we calculated how much K-MBI was recovered at 3 months. The recovery of K-MBI (δMBI) was obtained by the following formula:
The value of δMBI could be negative if the subject experienced functional deterioration after stroke. The mRS is a global scale of disability or dependence in daily activities widely used as an outcome measure, where 0 corresponds to no symptoms and 5 to a bedridden status or severe disability [26]. Patients in this study were divided into two groups according to their mRS stage at 6 months after stroke, with mRS ≤3 classified as 'good status' and mRS >3 as 'poor status'.
Statistical analysis
The Shapiro-Wilk test was done to verify the normal distribution of δMBI, and Wilcoxon signed-rank test was done to compare the scores of K-MBI at initial period and at 3 months. To verify the effect of initial cognitive function on functional improvement during 3 months after stroke, multiple linear regression analysis was performed for each domain-specific cognitive function. For predicting functional status at 6 months after stroke, logistic regression analysis was performed with independent variables such as demographic factors, initial motor function, and cognitive function. Independent variables in all above mentioned statistical analysis were selected through Spearman correlation analysis. Statistical analyses were performed using the SPSS ver.19.0 (IBM SPSS, Armonk, NY, USA) and p<0.05 was considered statistically significant.
RESULTS
Subjects demographics and functional evaluations
We initially assessed 414 patients for eligibility, a total of 291 subjects were excluded, and among them, 182 patients did not meet the inclusion criteria, 11 subjects had recurred stroke, 34 subjects had previous psychiatric problems, and 64 subjects were non-communicable. Of the remaining 123 subjects, 7 patients had hemineglect, 31 patients did not visit the outpatient clinic after discharge. Twenty-six patients were not evaluated at 3 months, and 19 patients were not evaluated at 6 months after stroke. Finally, statistical analysis was conducted with 40 subjects.
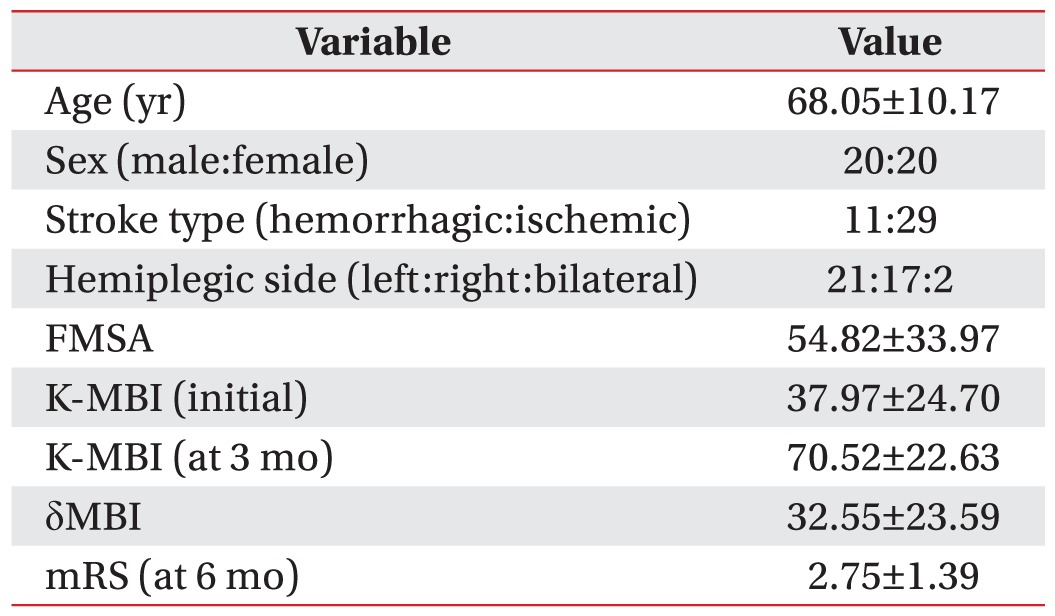
Initial functional evaluation including FMSA, K-MBI was performed within 2 weeks after stroke (11.06±5.63 days), and the follow-up evaluation of K-MBI and mRS were done at 3 and 6 months after stroke (Table 1).
The Shapiro-Wilk test verified the normal distribution of δMBI (p=0.054), and the Wilcoxon signed-rank test showed that the average value of K-MBI at 3 months after stroke was increased, as compared to the average value of initial K-MBI (p<0.001). According to mRS, 13 subjects were assigned as 'poor status', while 27 subjects were as 'good status'.
Cognitive impairment in 4 specific domains
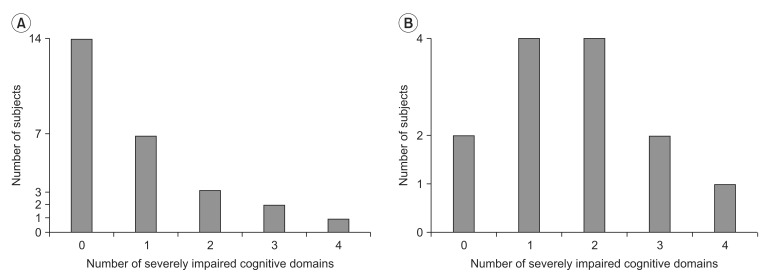
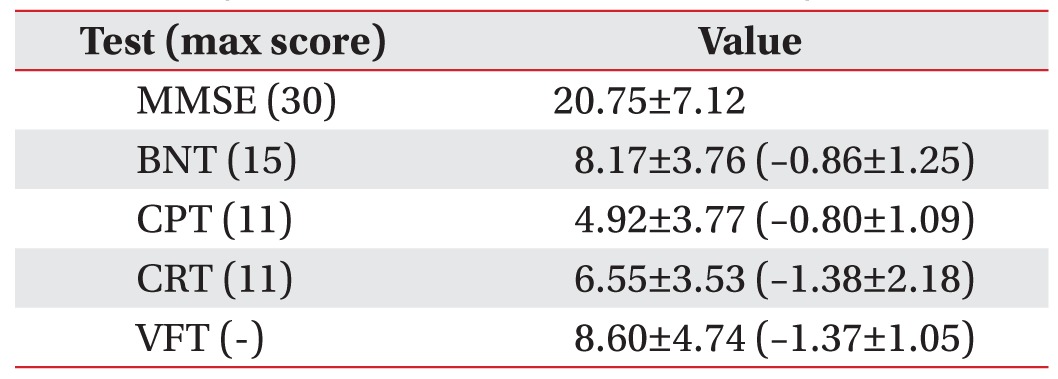
MMSE and 4 domain-specific neuropsychological tests were performed in 3 weeks after stroke onset (19.06±5.17 days). The mean values of MMSE and neuropsychological test scores were shown in Table 2. The number of domains that were impaired severely (z-score <–1.65) was counted (Fig. 1) for each subject. Subjects with hemorrhagic stroke had significantly more domains that were severely impaired than subjects with ischemic stroke (p=0.02, Mann-Whitney U test).
Domain-specific cognitive function and functional improvement during post-stroke 3 months (δMBI)
By the univariate analysis, initial K-MBI and NIHSS were significantly related to δMBI (p<0.05), while age, hemiplegic side, scores of MMSE, FMSA and KEA showed possible relationship (p<0.25) with δMBI.
We selected age, sex, hemiplegic side, scores of FMSA and initial K-MBI along with MMSE or other neuropsychological tests as independent variables in the regression analysis. Although sex showed no relation with δMBI, it was included into the model. NIHSS was not included into the model despite its significant relationship with δMBI in the univariate analysis, because NIHSS of 9 subjects, which were not assessed in the emergency room, could affect the validity of the results. Scores of FMSA were selected instead of NIHSS, because FMSA could represent neurological deficit for minimizing confounding effects. The NIHSS and FMSA were significantly correlated (Spearman rho=–0.660, p<0.001).
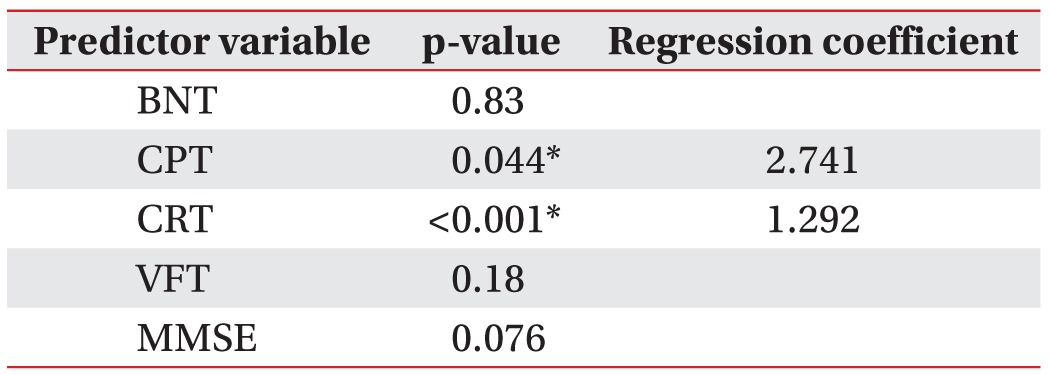
By the stepwise linear regression analysis with independent variables of age, sex, hemiplegic side, FMSA, and MMSE, MMSE (p=0.076) was not a significant independent variable to predict better functional improvement (Table 3). The same analysis with specific neuropsychological tests (BNT, CPT, CRT, and VFT) instead of MMSE showed that the CPT within post-stroke 1 month independently predicts δMBI at 3 months after stroke, even after controlling age, initial scores of K-MBI, and severity of motor impairment. Better functional improvement was anticipated if the patient was younger (p=0.027), had lower scores of initial K-MBI (p<0.001), had higher FMSA (p=0.008) or had higher scores of the CPT (p=0.048, R2=0.496). Independent variables such as hemiplegic side (p=0.575), and sex (p=0.437) were deleted during backward elimination.
The CRT independently predicts δMBI at 3 months after stroke (p<0.001, R2=0.614), while younger age (p=0.001), lower scores of initial K-MBI (p<0.001) and higher scores of FMSA (p=0.022) also assure better functional outcome. Hemiplegic side (p=0.825), and sex (p=0.515) were deleted during backward elimination.
The BNT (p=0.83) and the VFT (p=0.18) were not significant factors to predict δMBI at post-stroke 3 months.
Domain-specific cognitive function and functional status at post-stroke 6 months (mRS)
By the univariate analysis, age and MMSE showed significant relationship (p<0.05), and KEA and FMSA showed possible relationship (p<0.25) with mRS at poststroke 6 months. Hemiplegic side and initial K-MBI scores were excluded because they did not have considerable relationship with mRS in the univariate analysis.
For logistic regression analysis, we selected age, sex, FMSA along with MMSE or other neuropsychological tests as independent variables. The candidates such as KEA were not selected to prevent collinearity between independent variables because they showed significant relationship with FMSA. The Spearman correlation analysis between selected independent variables showed no correlation.
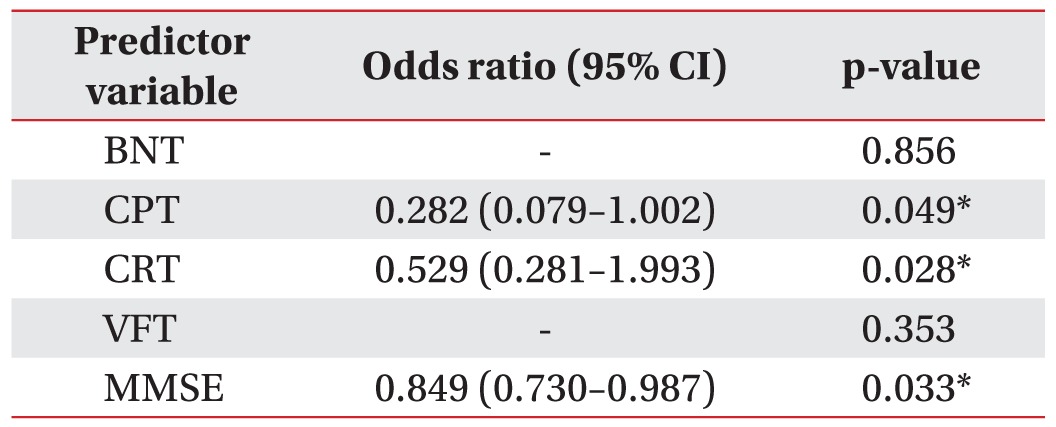
Table 4 showed the results of the stepwise logistic analysis. The patient has higher probability of having good functional status (mRS≤3) if he or she is younger (p=0.003), has higher FMSA (p=0.012) or has higher score of CPT (p=0.049, R2=0.419). Sex (p=0.962) was deleted during backward elimination.
The CRT independently predicts good functional status (mRS≤3) at 6 months after stroke as well (p=0.048, R2=0.411). Younger age (p=0.002), and higher FMSA (p=0.031) also assure better functional status. Sex (p=0.544) was deleted during backward elimination.
Unlike the previous analysis on functional improvement, MMSE (p=0.033, R2=0.438) predicts good functional status (mRS≤3) at 6 months after stroke independently, even after controlling for age and FMSA. Younger age (p=0.009), and higher scores of FMSA (p=0.025) also assure better functional status. Sex (p=0.565) was deleted during backward elimination.
BNT (p=0.856) and VFT (p=0.353) were not significant factors in predicting functional status at post-stroke 6 months.
DISCUSSION
Few studies have focused on the cognitive function as an independent predictor of functional outcome in patients with stroke [20]. Cognitive function can be an important factor affecting functional outcome in stroke patients as in the normal aging population [456] or in patients with other disease with cognitive dysfunction [789]. It can be easily assumed that the cognitive impairment can lower participation in rehabilitation therapy, and impede learning protocols or procedures needed to be independent after stroke. A study showed that the group of stroke patients with higher MMSE score had shown higher MBI and lower mRS after discharge [21]. Another study showed that patients with cognitive impairment required more rehabilitation intervention to obtain significant functional gains [27]. Cognitive impairment such as memory problems and mental dullness are frequently seen in many patients with stroke, and it can cause great negative impact on long-term rehabilitation outcome [2829].
In contrast to the previous studies, in our study, several specific neuropsychological assessments were selected for different cognitive domains instead of simple global screening measures for cognitive function. Furthermore, we used actual scores of K-MBI to measure functional improvement during post stroke 3 months as an outcome variable. Among the previous studies on domain-specific cognitive abilities as the independent predictors for functional outcome, Nys et al. [19] used dichotomized MBI (≥19) and the Frenchay Activities Index (≥15) as the functional outcome measures, and Wagle et al. [20] measured mRS for 13 months' functional outcome.
In this study, the scores of the CPT and the CRT in the acute stage were independent predictors for δMBI at post-stroke 3 months along with other variables such as age, initial K-MBI and FMSA, while MMSE was not significantly related. It is generally accepted that recovery of most of the MBI score occurs by 3 months after stroke [30], hence, subjects in this study showed significantly higher K-MBI at 3 months after stroke, as compared to initial evaluation. The current study included 10 subjects whose K-MBI were assessed at post-stroke 6 months, but there was no significant increase in K-MBI at 6 months, as compared to that of post-stroke 3 months. For functional improvement during the first 3 months after stroke, age and initial K-MBI along with FMSA, which represent initial neurological deficit, were all important predictors, in agreement with other studies [3132].
We verified that the z-scores of the CPT and the CRT, not MMSE, strongly predicted functional improvement after stroke. These results indicated the necessity of acute phase domain-specific neuropsychological assessment to predict functional improvement. Many studies on the link between cognitive impairment and functional outcome in stroke patients had limitations, as they used screening measure such as MMSE as a means of cognitive function. Even though MMSE is widely used for screening cognitive problems, its value in the screening of cognitive impairment in stroke patients is under debate. MMSE is dependent on age, language and education, and is not sensitive to right hemisphere lesions. Moreover, the limitations of MMSE also include inability to differentiate between diffuse and focal lesions [33], and insensitivity to domainspecific impairments such as abstract reasoning, executive functioning and visual perception and construction [24]. Our results could strengthen the proposal that tests that assess domain-specific cognitive function such as the CPT and the CRT can be used for better prediction of functional improvement during the first 3 months after stroke.
We also divided the subjects into two groups according to their mRS at post-stroke 6 months mRS≤3 as 'good status' and mRS>3 as 'poor status'. This dichotomization of functional outcome was adopted in previous studies [3435], and the cutoff value of independent walking in mRS is 3. Analysis of the relationship between the results of acute phase domain-specific neuropsychological assessment and the functional status at 6 months, indicated that the CPT and the CRT were independent predictors of good functional status (mRS≤3).
In this study, several tests were selected for the evaluation of cognitive function of patients with stroke. The CPT was selected for evaluation of visuospatial construction ability and the CRT was selected for the memory function. The results indicated that the CPT and the CRT independently predict functional outcomes after stroke after controlling for age, sex and initial neurological deficit. The visuospatial construction impairment is expected to hinder the ability of performing tasks in a 3-dimentional environment. The CRT with previous CPT can be a learning task that is adequate for the evaluation of learning ability, which may play an important role in functional progress in stroke patients. The function of memory in rehabilitation process of patients with stroke could be clinically important, because the ability to manipulate and maintain information might provide better performance in rehabilitation [36]. Memory deficit can influence the learning process. Decline in memory impairs activities in daily lives, ability to be independent and secure, and the capacity of learning skills to overcome their neurological deficit. In rehabilitation training, memory can play an important role in learning how to act with devices, and following stepwise instructions.
The BNT and the VFT showed no relation with functional outcomes. The BNT is used for the evaluation of speech and language, while the VFT is used for executive function; and both tests are based on the language function. The negative result of BNT and VFT in this study should be interpreted with caution. Because we excluded patients who were non-communicative, patients who were enrolled in this study would have had relatively good language function, and this could be the reason that z-scores of the BNT and the VFT were not related significantly to functional outcomes.
This study had some limitations. First, this was a retrospective study; hence, the inpatient rehabilitation therapy of each subject was not controlled. However, the amount and detailed contents of therapy were not significantly different between subjects. Moreover, some factors are reportedly related to cognitive impairments in stroke such as age, sex, fever or recent infection, hyperglycemia, previous stroke, presence of APOE ε4 allele, size or location of stroke, amygdala volume, hemorrhagic stroke, and cortical hypoperfusion [37]. To control for the effect of those factors, we excluded patients with depression, hemineglect, or pre-existing cognitive impairment such as Alzheimer disease and traumatic brain injury. However, we could not control every factor because of the retrospective study design. A well-designed prospective study with detailed neuropsychological evaluation will provide a more meaningful estimate of the relationship between cognitive ability and functional outcomes after stroke. Second, despite review of a large amount of medical records, only 40 subjects were included in the analysis. Further study with a larger sample may present more meaningful information. Third, since only subjects who completed neuropsychological tests were included in this study, there is a risk of selection bias. However, many patients with stroke could not perform the detailed neuropsychological evaluation because of poor general medical condition, severe motor deficit, and limited endurance with deficit in attention [38]. Our study also showed that an early detailed neuropsychological evaluation was applicable to patients with relatively mild stroke. The average initial NIHSS score was 6.25±4.24. Therefore, our findings may not be directly generalized to the entire population of stroke patients. Fourth, initial cognitive evaluation was not done in the very early period, because it usually takes several days to weeks before patients are transferred to the Department of Rehabilitation Medicine after onset of stroke. In our study, neuropsychological evaluations were performed in about 19 days after stroke onset.
In conclusion, visuospatial construction and memory assessed by the CPT and the CRT in the acute phase can predict functional outcomes after stroke. Therefore, domain-specific neuropsychological assessments could be considered in patients with stroke in the acute phase to predict long-term functional outcome.
 XML Download
XML Download