

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Axial mesodermal dysplasia complex (AMDC) is a combination of various malformations of musculoskeletal structures and internal organs, including the branchial, cardiovascular, pulmonary, gastrointestinal, and genitourinary system, which is caused by abnormal fetal mesodermal development [1]. As suggested by the definition, AMDC can occur as a wide spectrum of clinical manifestations ranging from rostral craniofacial anomaly to caudal sacral deformity including multiple forms of axial skeletal anomalies. Owing to this clinical manifestation of anomaly, AMDC includes many syndromes such as Goldenhar, Klippel-Feil, VACTERL, and MURCS [2]. Among these clinical syndromes, a few have been reported to be associated with central nervous system (CNS) anomalies. Klippel-Feil syndrome, which was recently classified as AMDC [1], has been widely recognized as a cervical vertebral anomaly and is often associated with cervical spinal cord anomaly including cervicomedullary junction, and sometimes mirror movements [34]. Similarly, there have been several reports of Goldenhar syndrome accompanied by CNS dysplasia, including not only facial skeletal deformities but also cranial nerve anomalies [56]. Taken together, in the AMDC syndromes, CNS malformations appear to be frequently enrolled. Thus, AMDC could be considered as a complex of deformities that occurs as a combination with not only musculoskeletal deformities, but also CNS developmental disorders. In line with this suggestion, here, we report a case of a complex form of AMDC involving musculoskeletal deformities such as right facial deformities, submucosal cleft palate, cervical spine and rib malformations, right scapular deformities, and the rhombencephalic anomaly of medullary neuroschisis with left infranuclear-type facial nerve palsy.
CASE REPORT
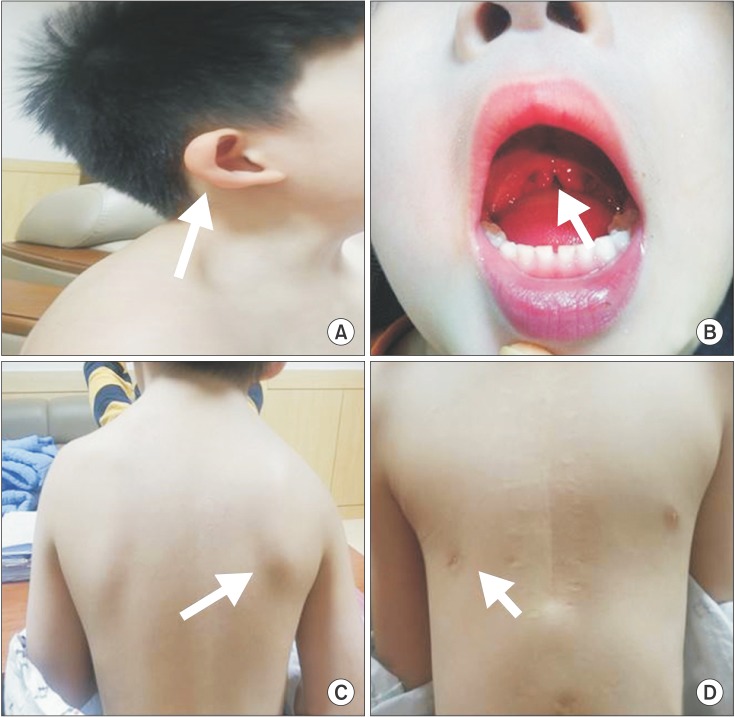
The patient, a 4-year-old boy, was referred to the rehabilitation medicine department for evaluation of facial deformities and posture abnormalities. He was born prematurely at 35 weeks via cesarean section due to the premature rupture of fetal membranes. The mother was healthy and did not report the use of alcohol, tobacco, or drugs during pregnancy. The family history was non-contributory. At birth, it was noticed that he had a congenital cardiac defect; ventral septal defect, atrial septal defect, and patent ductus arteriosus, for which he underwent surgical treatment 6 months after birth. According to his mother's description, he was otherwise healthy with normal development. After performing a careful physical examination, several dysmorphic features were noted including asymmetrical facial skeleton, left facial weakness, and right microtia (Fig. 1A). Additionally, uvular bifida was noticed when the inside of his mouth was examined (Fig. 1B). His neck was relatively short, the right shoulder blade was located relatively more superior than the left, and the range of motion of the shoulder was limited during abduction (Fig. 1C). Moreover, the right pectoralis major appeared shrunken, and thoracic asymmetry was confirmed, where the right nipple was relatively lower than the left (Fig. 1D). In addition to these malformations, the mirror movements of the opposite hand during voluntary movements of each hand were observed. Additional neurological examination of the patient showed left facial palsy, but no ocular movement disorder was observed. Furthermore, muscular strength of the limbs was normal, and pathological reflexes and upper motor neuron signs were not observed.
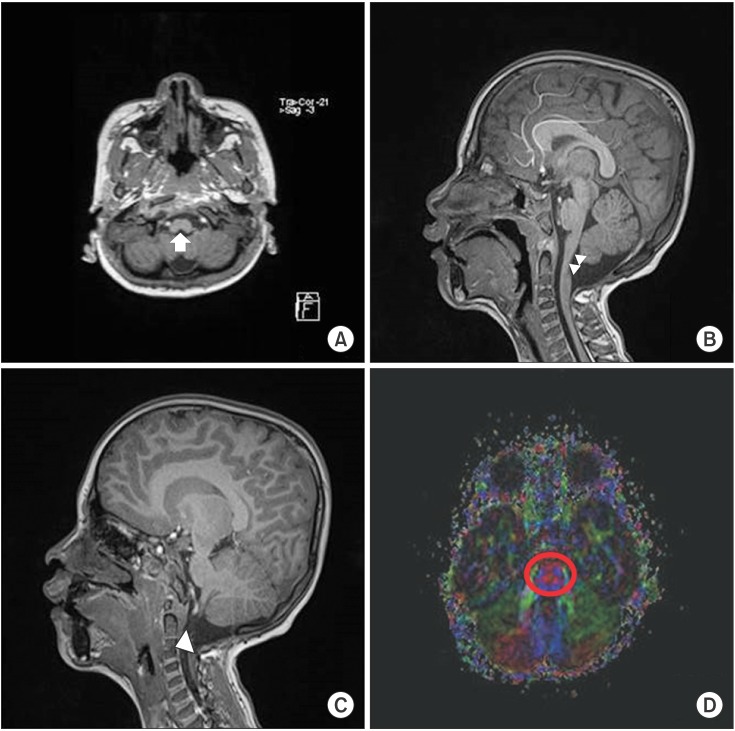
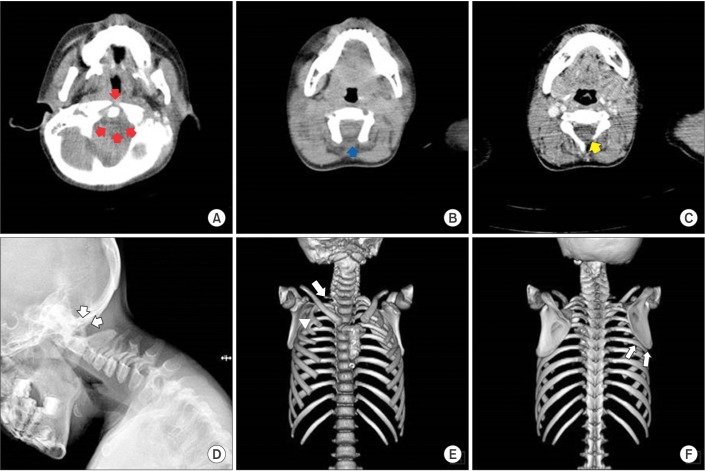
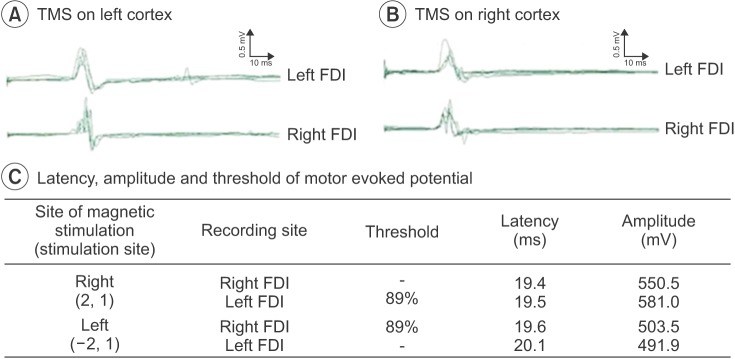
According to the Korean-Wechsler Intelligence Scale administered to evaluate the cognitive function of the patient, verbal intelligence quotient (IQ) index was 71, performance IQ index was 86, and the overall IQ index was 76. Cervical spine and brain magnetic resonance imaging (MRI), and cervical and thoracic computerized tomography (CT) were performed to rule out the additional CNS malformations and musculoskeletal anomalies. Cervical spine and brain MRI showed medullary neuroschisis without pontine or cerebellar hypoplasia, and there was no evidence of abnormalities of descending tracts and transpontine fibers in the basis pontis in the diffusion tensor MRI (Fig. 2). In the cervical spine, vertebral body fusion at the level of C3 and C4 was observed (Fig. 2C), and cervical and thoracic CT images showed dysplasia at the posterior cervical spine (Fig. 3A–D). In addition, fusion deformities of the right 2nd and 3rd rib, incomplete development of the right 1st rib were observed (Fig. 3E), and the right scapula was elevated compared with the left (Fig. 3F). To reveal the motor organization pattern of both hands associated with mirror movements, motor evoked potentials (MEP) study was performed with transcranial magnetic stimulation. The optimal stimulation coordinate was selected if a MEP of 50 µV or more was evoked at least 5 times from 10 stimulations of transcranial magnetic stimulation with the lowest excitation threshold. The optimal stimulation position for the left cortex was (–2,1) according to the 10–20 system, MEPs were simultaneously evoked at the right and left first dorsal interossei muscles; the threshold was 89% of the maximum stimulus intensity. Similarly, the optimal stimulation position for the right cortex was (2,1) MEPs were simultaneously evoked at bilateral first dorsal interossei muscles (Fig. 4). Facial motor nerve conduction studies showed a delayed latency and low amplitude of the left facial nerve compared with the right, where facial skeletal deformities were observed.
DISCUSSION
This report describes a patient who simultaneously showed musculoskeletal deformities of AMDC such as unilateral facial skeletal deformities, submucosal cleft palate, cervical spine deformities, and scapular anomaly, congenital heart disease, and the rhombencephalic anomaly; medullary neuroschisis with associated mirror movements and unilateral facial palsy. The patient described herein presented with various defects extending to the craniocaudal level with various gradations of severity, and a wide range of CNS malformations, which were detected by physical and neurological examinations, radiological findings, and electrophysiological evaluations. These occurrences of various combinations and the various severity gradations for congenital anomalies have not yet been reported from a Klippel-Feil syndrome 'plus' point of view [7]. We think that from a Goldenhar syndrome point of view, this co-occurrence of CNS malformations; rhombencephalic anomaly in Goldenhar syndrome may also be a very unusual case.
From the present case, we suggest that these complex malformations with various gradations of severities reflect sequential disruption of the tissues derived from one or more of three germ layers during embryogenesis. Generally, deformities accompanying AMDC are believed to arise from the failure of mesodermal cell migration around the 4th week of embryogenesis [2]. However, this prevailing hypothesis has a limitation in explaining the pathogenic mechanism of this case, because rhombencephalic malformations, which arise from abnormalities in neuroectodermal development, cannot occur in this period. In particular, the co-existing dysplasia of the musculoskeletal system including cranial and postcranial regions and cranial nerve system may have been derived from sequential disruption of the tissues during extended periods from the early stages of neural tube formation to the period of neuroectodermal differentiation. From previous studies of the period of the occurrence of these anomalies, we found that cervicomedullary neuroschisis occurs during neural tube formation [8], and brainstem anomaly below pons appears to occur during rhombencephalic development [69]. A previous study reported that neuroschisis at the level of the cervical spine, induced by neural tube malformation, may affect the sequential development and migration of neural crest cells after neural tube formation, and may induce anomalies in musculoskeletal and CNS maldevelopment [2]. Moreover, another previous study regarding Mobius syndrome with musculoskeletal deformities, which is believed to be a complex developmental disorder in the period of the 3rd and 8th week of embryogenesis [10], is in accordance with our observation. Considering these previous results, the present case of dysplasia may result from a failure in neural tube fusion and mesodermal cell migration, which takes place during the 3rd to 4th week of gestation, and the failure of sequential rhombencephalic segmentation after neural tube formation in the 5th week, as well as the abnormal differentiation of the metencephalon and myelencephalon, especially myelencephalon dysplasia. From the point of view of the various combinations and the gradations of anomalies, we can deduce that when abnormalities occur during the vulnerable stages of embryonic development (e.g., neural tube formation, mesodermal migration, and rhombencephalon segmentation), discrete or continuous associated developmental disabilities can occur. Depending on the severity of damage and the ability of the embryo to restore itself, phenotypes after birth can be accompanied by abnormalities of different degrees in internal and external structures of mesodermal origin. We cannot conclusively exclude the AMDC spectrum with dysplasia of the CNS. Therefore, when examining patients with sporadic phenotypes of AMDC, hidden axial mesodermal dysplasia must be closely observed, and neurological screening including CNS examination should be performed simultaneously. In addition, we also suggest that the neurophysiological mechanism of the hind brain abnormality, the medullary neuroschisis, which could lead to the abnormal pyramidal decussation, may induce the neural substrate for the motor organization of the bilateral mirror movements. In accordance with this suggestion, a previous study revealed an association between cervicomedullary neuroschisis and mirror movements in Klippel-Feil syndrome patients [4]. Therefore, we can propose that the unknown origins of congenital mirror movements may be the result of developmental abnormalities at the cervicomedullary junction occurring as early as the embryonic period.
In conclusion, cases of AMDC with minor sporadic dysplasia should be examined for various anomalies for musculoskeletal structure and internal organs or dysplasia of neural structures that cannot be noted through simple physical and neurological examination. Among the various abnormalities accompanying AMDC, CNS malformations can be encountered. Since CNS malformations with mild symptoms can be easily overlooked, neurological examination, including brain imaging, should be recommended for patients suspected of having AMDC. Further studies on larger cohorts are needed to reveal the underlying cause of this syndrome and to better understand its pathological mechanism.
 XML Download
XML Download