

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A stroke is a major cause of severe chronic disabilities with a high prevalence in the elderly. The Korean National Health Insurance Corporation reported in 2011 that cardiovascular diseases are the second most common disease in the elderly from 65 to 74 years of age. Also, about a half of stroke patients suffer life-long disabilities in spite of relatively successful acute management and advanced multidisciplinary treatments [1]. Consequently, several Western studies had reported on the functioning status after stroke. Some studies monitored the long-term changes of functioning after stroke [2], and some conducted World Health Organization Disability Assessment Scale II (WHODAS II) surveys to evaluate the functioning status of subjects with chronic stroke in a community [34] regarding its conceptual basis in the International Classification of Functioning, Disability and Health (ICF) and a holistic approach to the assessment of impairments and disabilities, as well as activities of daily living (ADL) scales [3].
WHODAS II was recommended by World Health Organization in 2001 for evaluating the ADL of people with chronic disabilities [56]. WHODAS supports and complements the concept of ICF regardless of the types of diseases [3], and its validity and reliability have been proven.
In South Korea, however, there has been no study on the effects of personal background on the long-term functioning of subjects with chronic stroke in a community. Moreover, there has been no study on the subjects with chronic stroke that used WHODAS II. In South Korea, WHODAS has been only used for psychiatric and rheumatological conditions until recently. In addition, there has also been no study on the long-term functioning of subjects with chronic stroke in relation to cognition, independence in daily living, and disease durations.
In this study, we aimed to follow up on the long-term functioning of subjects with chronic stroke by using WHODAS II. We also collected the scores of initial and discharge scores of the Korean version of the Mini Mental Status Examination (K-MMSE), and the Korean version of Modified Barthel Index (K-MBI), and evaluated the effect of cognition and independence on daily living on long-term functioning.
MATERIALS AND METHODS
Enrollment of subjects
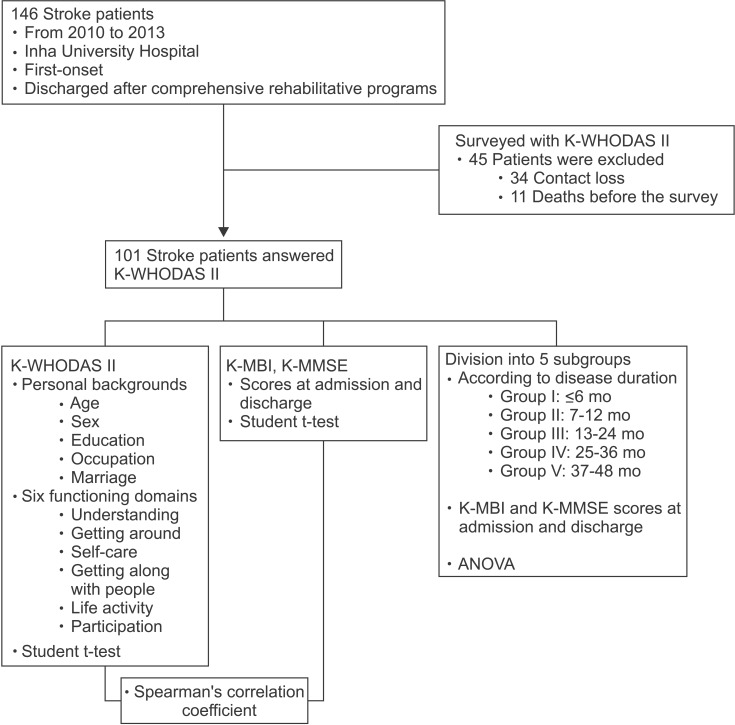
There were 146 subjects with chronic stroke, who were diagnosed at their first-onset acute stroke at Inha University Hospital from 2010 to 2013, and also discharged after they were initially enrolled in comprehensive rehabilitative programs. In total, 101 patients agreed to participate in the survey with the K-WHODAS II (Korean version of WHODAS II).
We retrospectively reviewed their medical records and gathered data on the scores of K-MMSE and K-MBI at admission and discharge, to evaluate functional outcomes in hospital and to assess their relationship with the functioning after discharge. The time of admission was set as the first day the patients were transferred to department of physical and rehabilitation medicine. The time of discharge was set as the last day when the functioning status was evaluated before the discharge, which was mostly within one week from the discharge date.
Survey with K-WHODAS II
Furthermore, we surveyed the patients with the K-WHODAS II, which consisted of 12 items. We asked 12 questions on the ADL of subjects with chronic stroke in a community [7], and on personal background, such as gender, age, marital status, educational levels, working status, and marital status. We informed the patients or families about the purpose of the study and also conducted the survey at the outpatient clinic or by phone.
The K-WHODAS II consisted of two main criteria. The first part was about personal background including gender, age, marital status, educational level, and working status. The second part was composed of 12 questions about six domains: two questions for each domain of understanding, getting around, self-care, getting along with people, life activity, and participation. Each question had to be answered according to a 5-Likert scale (1 'no difficulty' to 5 'cannot do'). The total scores of six functioning domains ranged between 12 and 60, with lower scores indicated better functioning. The severity of each domain was graded according to the existing standard; total scores of 1–4 belong to mild disability, 5–9 moderate disability, and 10–48 severe disability [8].
Modifications of the items
In this study, we modified the sub-items of the category of working status and marital status according to what we aimed to investigate. The original version of WHODAS II divided the working status into pain employment, self-employed, unpaid employment, students, housewives, retired, unemployed, and others. The marital status originally included never married, married, separated, divorced, widowed, and cohabiting.
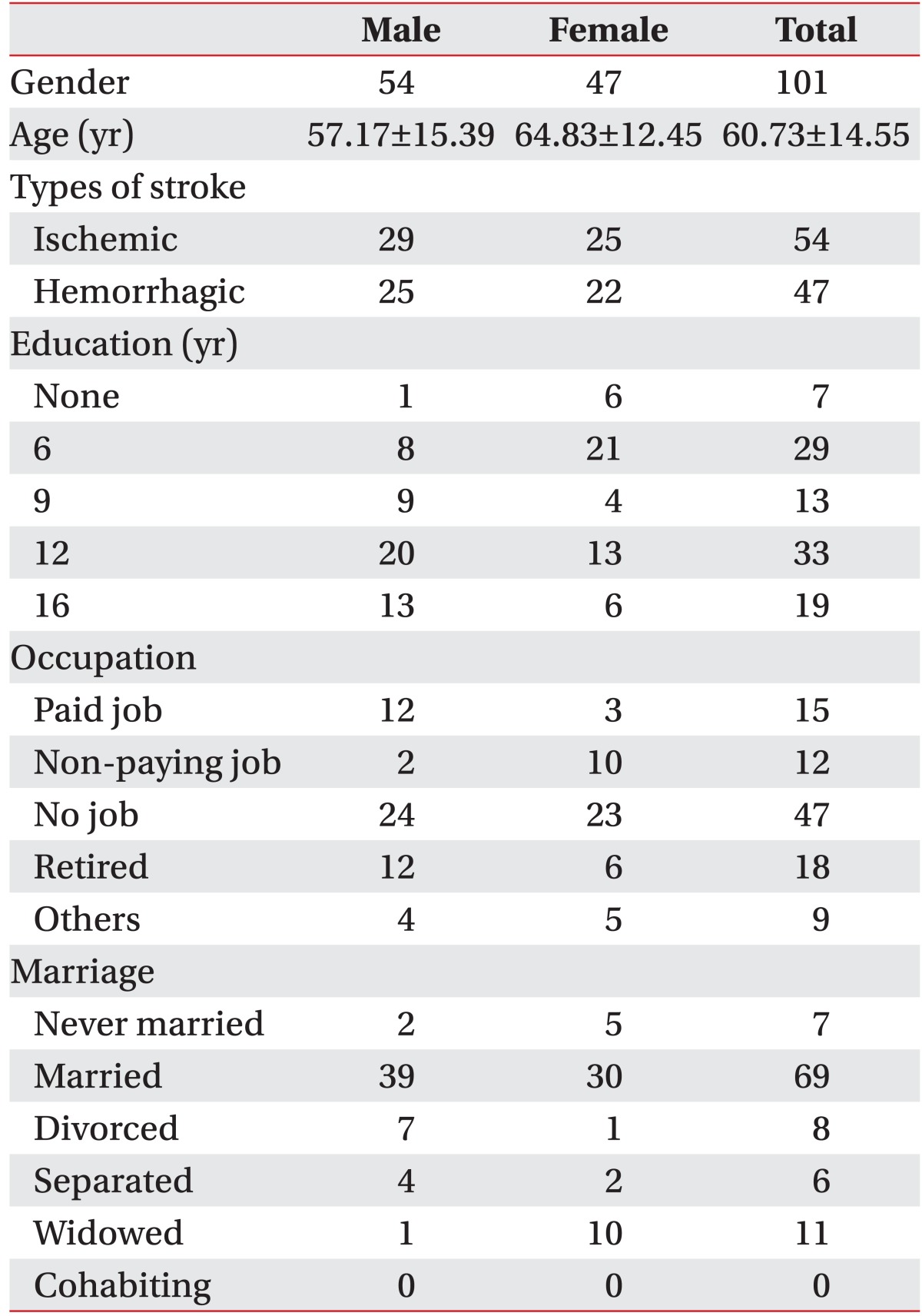
In this study, we defined paid job to include employment and self-employed because they were both currently working statuses with remuneration. Non-paying job was defined to include unpaid work, such as students and housewives because they had a current working status but had no remuneration (Table 1).
We further modified the multiple sub-items into dichotomous variables to find out whether the presence of job and a cohabiting companion affected the functioning status. Having a job included paid job and non-paying job; having no job included the retired and unemployed. Living with a partner included being married; living without a partner included never married, separated, divorced, and widowed. Then we compared the total scores of K-WHODAS II between two groups (Table 2).
Subgroups of the subjects
To assess whether the K-MMSE and the K-MBI at the admission and discharge were different according to the disease durations, we further divided subjects with chronic stroke into five subgroups according to the time elapsed after the onset of stroke: shorter than 6 months (group I), 7–12 months (group II), 13–24 months (group III), 25–36 months (group IV), and 37–48 months (group V) (Fig. 1).
Statistics
Statistical analyses were performed with SPSS ver. 18 for Windows (SPSS Inc., Chicago, IL, USA). The Student t-test was applied to compare the scores of the K-MMSE and the K-MBI at admission and discharge. The Student t-test and ANOVA were applied to compare the total scores of K-WHODAS II between different statuses of personal background. A Spearman correlation coefficient analysis was applied to evaluate the relationships between the K-MMSE, K-MBI, and personal background with K-WHODAS II. In addition, the ANOVA was applied to compare the functioning domains among the five groups and to assess the trends of the K-WHODAS II changes among the five groups after stroke onset. The statistical significance was below 0.05 (p<0.05).
RESULTS
Participants
Initially, 146 stroke patients were enrolled. Among them, 45 patients were excluded because there was a loss of contact with 34, and an additional 11 deaths before the survey. Consequently, 101 patients answered the K-WHODAS II questionnaire. Fifty-four patients had an ischemic stroke and 47 had a hemorrhagic stroke.
Personal background
Forty-seven patients were female and 54 were male. The mean age of the patients was 60.7 years (women, 64.83 years; men, 57.17 years). Sixty-nine of the patients were married, 8 divorced, 13 unmarried, and 11 widowed. The educational level differed as 29 patients had primary school education; 13, middle school education; 33, high school education, and 19, tertiary education, whereas 7 received no formal education. Sixty-five patients had no jobs at the time of survey, and 27 patients were employed, including unpaid jobs, such as housewives and volunteers (Table 1).
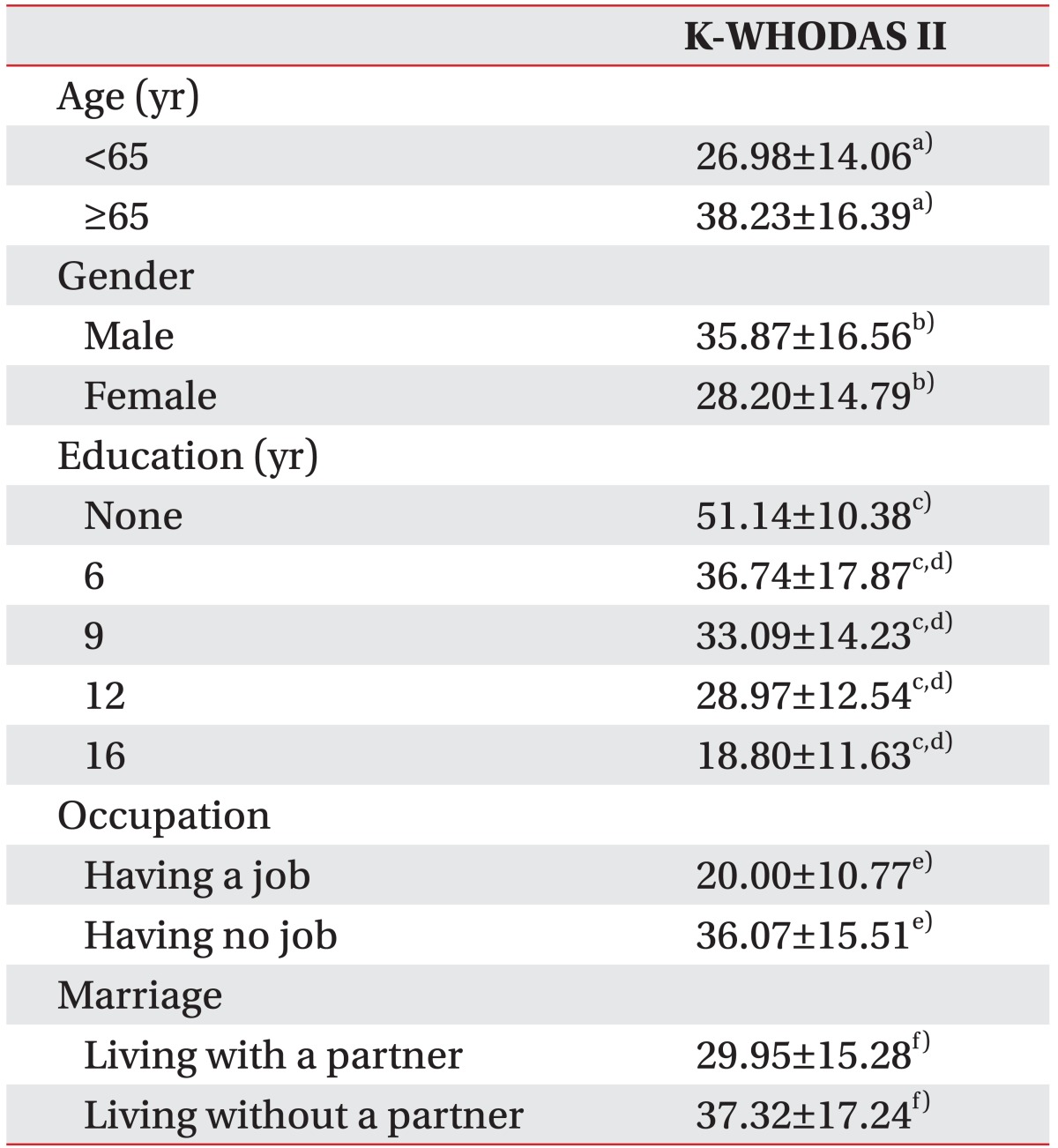
The influence of the personal background (e.g., age, gender, educational level, working status, and marital status) on the K-WHODAS II was assessed. The elderly showed higher scores on the K-WHODAS II (26.98 in <65 years and 38.23 in ≥65 years; p<0.05). Women showed lower scores on the K-WHODAS II (male 35.87 and female 28.20; p<0.05). Higher educational levels positively influenced the K-WHODAS II (no education 51.14, up to 6 years 36.74, 9 years 33.09, 12 years 28.97, and more than 16 years 18.80; p<0.05). Having a job, including paid and unpaid employment, housewives, students, and volunteers, positively influenced the K-WHODAS II (having a job 20.00 and having no job 36.07; p<0.05). Living with a partner, which included married status, positively influenced the K-WHODAS II (29.95 in those who lived with partners and 37.32 in those without partners; p<0.05) (Table 2).
The influence of disease duration on the long-term functioning
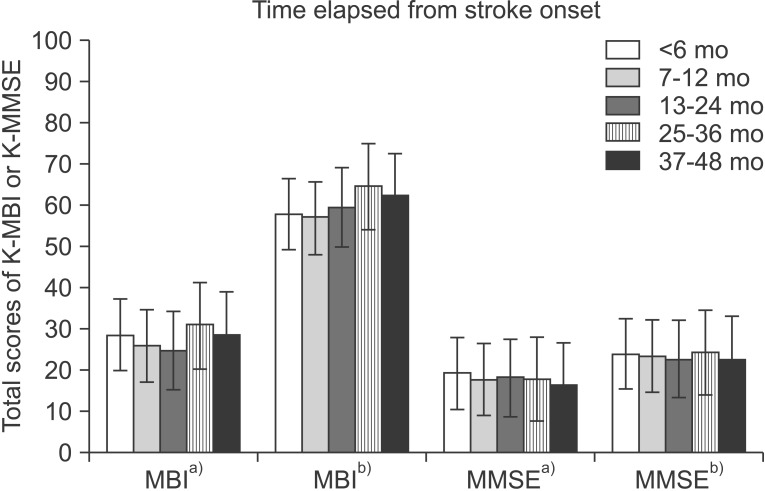
We subdivided the discharged patients into five groups according to the time elapsed from the onset of stroke to when they completed the K-WHODAS II survey. Eleven patients were less than 6 months after the onset of stroke, 26 patients between 7–12 months, 33 patients between 13–24 months, 18 patients between 25–36 months, and 13 patients between 37–48 months. These five groups showed no significant difference as we compared their K-MBI and K-MMSE at admission and discharge, respectively (p>0.05) (Fig. 2).
Functional status in hospital
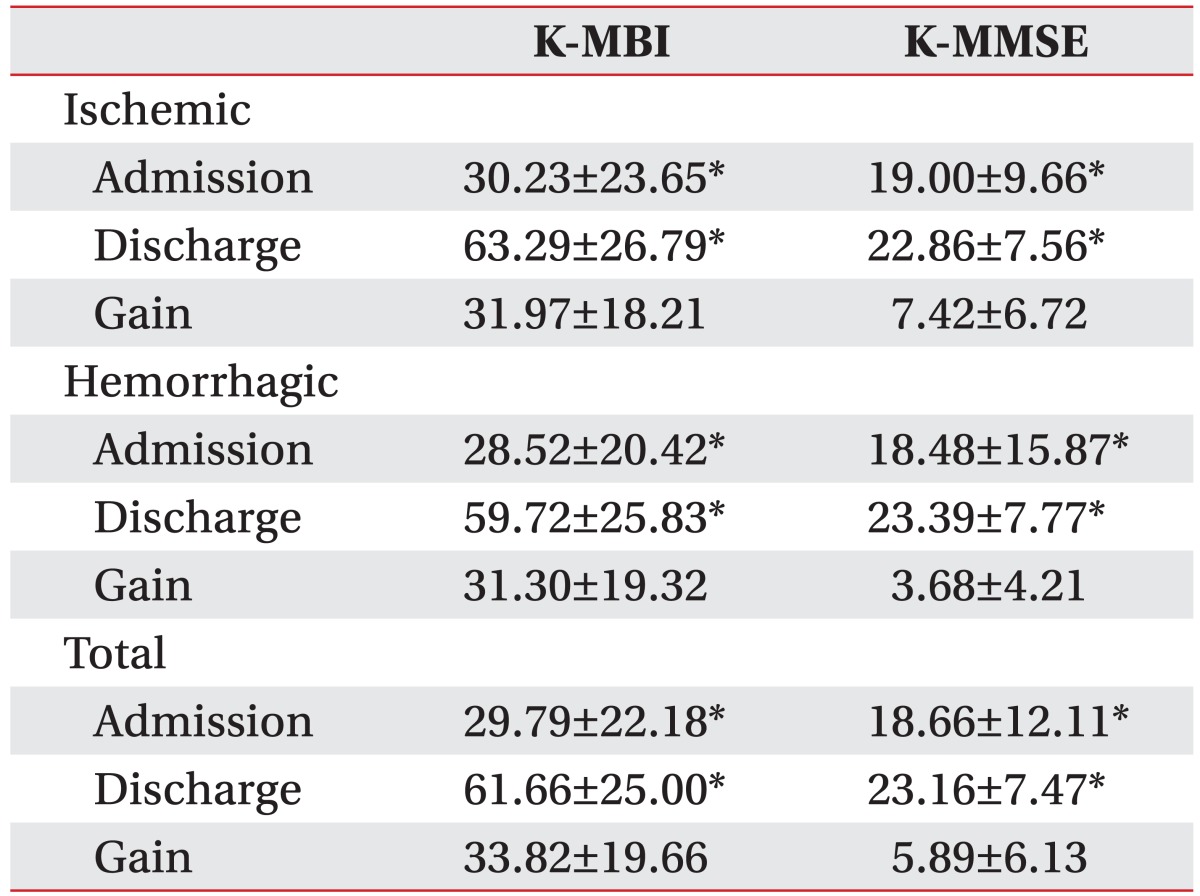
We compared the K-MBI and the K-MMSE on admission and discharge, and all stroke patients showed significant improvements on the K-MBI and the K-MMSE at discharge (p<0.05) (Table 3).
Long-term functioning and contributive factors
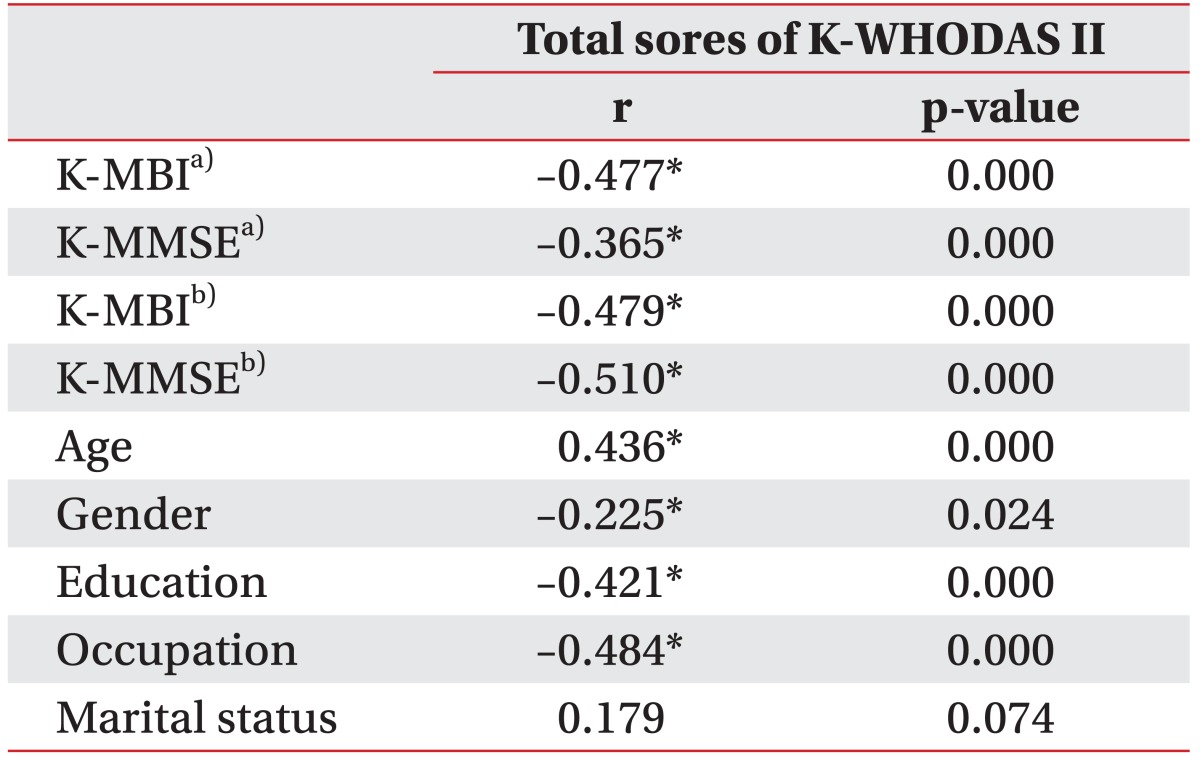
We also assessed the correlations between the total scores of K-WHODAS II with the K-MBI, the K-MMSE, and personal background. The K-MBI and the K-MMSE had correlations with the total scores of K-WHODAS II. The K-MMSE scores at discharge showed the strongest correlation with total scores of K-WHODAS II (r=–0.510); then K-MBI at admission (r=–0.480), the K-MBI at discharge (r=–0.477), and the K-MMSE at admission (r=–0.365), respectively (p<0.05). Concerning personal background, the educational level and having a job also had a strong correlation with the total scores of K-WHODAS II (r=–0.421 and r=–0.484, respectively; p<0.05). Furthermore, those younger than 65 years old and women had a correlation with lower scores of K-WHODAS II (r=0.436 and r=–0.225, respectively; p<0.05). Whether or not one lived with a partner did not have a correlation with the total scores of K-WHODAS II (r=0.179, p>0.05) (Table 4).
The changes of long-term functioning status
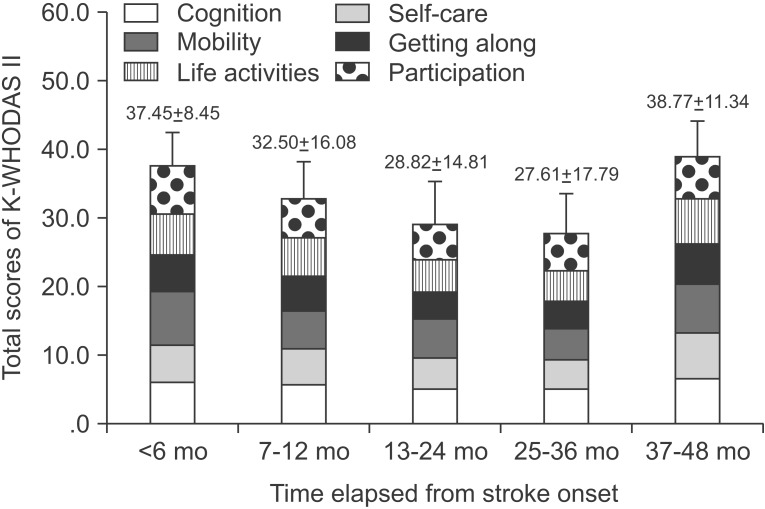
The trends of the changes of the K-WHODAS II among the five groups after stroke onset were analyzed. The sustaining trends of the scores of each of the six functioning domains of the K-WHODAS II and the sum of them (total scores of K-WHODAS II) were maintained until about 3 years after the stroke onset, but declined thereafter. Group I (less than 6 months since stroke onset) showed the highest total scores of K-WHODAS II (37.00±8.45), whereas group IV (25–36 months) showed the lowest total scores of K-WHODAS II (27.61±17.79). Group V (36–48 months) showed increased total scores of K-WHODAS II (38.77±11.34) compared to group IV. The difference of scores between groups I and IV was about 9.84, and that between groups IV and V was 11.15. However, all these differences had a p-value >0.05. Therefore, these score changes, as in functional changes, were not statistically significant but only trends. The social participation, which was one of five domains of the K-WHODAS II, showed an exceptionally earlier decline; it was maintained until 13–24 months but declined from 25 months after onset (Fig. 3).
DISCUSSION
The necessity of long-term monitoring of functioning status
Comprehensive, intensive, and task-orientated rehabilitation is crucial for recovery in stroke patients. Early stroke recovery occurs within 3 months after onset, and therefore acute rehabilitative treatment reinforces the maximal recovery from stroke impairment in this period. Subacute stroke recovery partially continues after 6 months, and chronic rehabilitative treatment focuses on the maintenance of functional status and on the use compensation techniques. Therefore, the long-term follow-up of functioning for subjects with chronic stroke is important to find out whether patients are able to adjust to their daily lives in a community.
However, there is a lack of reports to assess the longterm status of the functioning of subjects with chronic stroke returning to a community, especially in South Korea.
The recovery of stroke patients is affected by not only the initial severity of brain injury and rehabilitation therapies but also personal background, such as familial support, socio-economic status, and accessibility to rehabilitation facilities [1]. Hence, this current study surveyed the K-WHODAS II to follow-up on the trends of the functioning of stroke patients.
Long-term functioning and contributive factors
We assessed the extent of recovery in cognitive function and ADL by comparing the K-MMSE and K-MBI at admission and discharge. In this study, the cognitive function and ADL markedly improved through rehabilitative programs. These functional outcomes consequently had long-term effects on the lives of subjects with chronic stroke after discharge, and that was proven by the negative correlations between the K-MMSE and the K-MBI with the total scores of K-WHODAS II in which lower K-WHODAS II scores meant a better state of ADL. As stated in previous studies, cognition deficit negatively affected the instrumental ADL and their social life [9], thus resulting in poor long-term functioning. Furthermore, the dependency in daily living and poor functional performances also led to a decline in long-term functioning status [10].
Concerning the personal background, the education level and working status were strongly correlated with functioning in long-term lives after discharge. This suggests that a higher educational level or working status helps patients to sustain better self-care and social life by providing them with more benefits from medical insurance and their higher socio-economic status [1]. Similarly, a previous study reported that stroke patients in a higher socio-economic status received better medical treatment and showed better functional outcomes [2].
A South Korean study had previously reported the positive influence of a family, the most influential social supportive system, on the psychosocial function and ADL of the subjects with stroke [10]. Although the current study showed that marital status had no correlations with total scores of K-WHODAS II, living with a partner still had significantly lower total scores of K-WHODAS II compared with living without a partner thus reinforcing the positive effect of living with a companion on the functioning status of the subjects with chronic stroke.
In addition, gender and age were correlated with the functioning status after discharge. A previous study had reported that elderly patients and female patients were functionally more disable. In fact, the old age was the more impact factor for the functioning status because of its age-related comorbidity that decreased the ADL abilities [11]. Women were shown to be functionally more disabled than men but that was actually because of their old age and comorbidity at stroke onset, rather than gender [11]. The current study showed that the elderly and male patients were correlated with higher total scores of K-WHODAS II. Considering South Korean cultures and its stratified gender roles, we assume that South Korean male patients were unfamiliar with independent households and self-care and were more vulnerable to social isolation because of the cessation of socio-economic activities, which eventually affected their long-term functioning status in a community.
The K-MBI is a practical tool to evaluate ADL, but it is an in-hospital tool to measure the capacity of ADL rather than the actual performance of ADL in a community. Therefore, the K-WHODAS II would be a more informative instrument to evaluate the actual status of the functioning of stroke patients in a community.
The changes of long-term functioning status
Using the K-WHODAS II, we followed up on the changes of functioning status for 4 years after the onset of stroke and discovered that functioning status was maintained until 24–36 months but declined thereafter. A previous study published in 2009 reported that the functional independence of stroke patients annually decreased up to 5 years, and 3 years after stroke onset was the point of greatest change [2]. Hence, our study showed similar results to this previous study.
Several factors may cause a decline of the functioning status from 36 months after stroke onset. First, the socioeconomic status of patients and family may be involved in the maintenance of functioning for a certain period of time. A higher socio-economic status motivates patients for rehabilitative treatment and provides them with sufficient rehabilitation services, information about health, and ongoing management of risk factors and chronic conditions [1]. Second, limited accessibility and the supply of community-based rehabilitation may restrict the interventions and thus cause a decline of functioning status.
Our study implies that stroke patients had severe mobility limitation, and that this finding was contradictory to a previous study, which had reported that the patients who received interventions for 6 months after discharge maintained favorable mobility compared with those who received only conventional managements [2]. This might be because of a lacking welfare system in South Korea, including traditional house structures, inconvenient roads, and dependency on the caregivers. Consequently, the renovation of the environmental state, reinforcement of community-based rehabilitation, caregiver education, and regular intervention by physicians after discharge would promote the early detection of changes in the health condition and maintenance of functioning.
Comparison of WHODAS with other disability measures (Why WHODAS?)
Various types of questionnaire have been developed to evaluate the influence of ill health status on one's life and the outcomes of care. Among them, the short form 36 health survey questionnaire (SF-36) and the EuroQoL five dimensions questionnaire (EQ-5D) have occasionally been used for the evaluation of disabilities.
SF-36 is an abbreviated generic measure of 149 questions [12] that evaluates 8 health domains of the general population as a form of patient reported outcome measures (PROM). EQ-5D is an international measure of health that evaluates 5 functioning domains including clinical and economic aspects of the health status. Both are well-known and frequently used but do not evaluate personal background.
Nonetheless, we used WHODAS II in this study because WHODAS II best supports the ICF, the standard of functioning or disability measure. Furthermore, WHODAS can be applied to any kinds of illness, including physical, psychological, or substance-use disorders [3].
Subjects with chronic stroke have difficulties because of not only the disease progression but also concomitant physical, psychological, or substance-use disorders; thus, we applied WHODAS II, which could evaluate overall functioning difficulties in a community.
Future strategy
The OECD Healthy Care Quality in 2012 reported that South Korea needs to improve its long-term management of cardiovascular diseases, including the prevention, education, and after-discharge rehabilitation [13]. Because of a decline of functioning after 36 months of stroke onset in this study, regular monitoring of functioning or disabilities with a reliable international tool, such as the WHODAS II, would help to improve the effects of long-term management. Furthermore, community-based rehabilitation services with appropriate evaluation and remodeling of environmental structures would ensure maintenance of functioning and the decrease of medical expenditures.
Limitations
We enrolled stroke patients whose onset was up to 48 months and asked them to complete the K-WHODAS II questionnaire. However, the current study was not a cohort study, hence some limitations were inevitable. First, we could not investigate changes of personal background before and after the stroke onset. Second, we could not clarify the causal relationships between the personal background and the long-term functioning status. We could only find out that some aspects of personal background, particularly having a job and living with a partner, positively affected the functioning status at the time this K-WHODAS II survey was conducted. Thus, it is necessary to carry out a longitudinal study with a long-term follow-up of patients after disease onset. Moreover, it is necessary to conduct a future cohort study on the trends of the long-term status of functioning and disability.
Furthermore, we could not rule out the confounding effects of personal background and K-MBI and K-MMSE. The logistic regression should have been applied to evaluate the confounding effects personal background and K-MBI and K-MMSE on the total scores of K-WHODAS II.
Conclusion
The long-term functioning after stroke was related not only with cognitive and motor status in hospital, but also with some salient aspects in the personal background of the patients. K-WHODAS II may be used to monitor functioning status in a community and to assess personal background in subjects with chronic stroke.
 XML Download
XML Download