INTRODUCTION
Abdominal muscle is one of the most important muscles in rehabilitation of patients with musculoskeletal or neurological problems, and has a variety of functions including body movement, posture control, balance, back pain control and supports for coordination of upper and lower limb movements [
1]. Thus, various exercises are used in different clinical situations in order to strengthen the abdominal muscles. Of those exercises, curl up or leg raise exercise is one of the commonly performed trunk exercises which are publicly well known, and the procedures are not difficult [
234]. However, there are no standard sets for the exercise angles formed by the floor and trunk during the curl up exercise, or by the floor and leg during leg raise exercises. Therefore, the exercise angles differ and are dependent on the performers, or at each trial. If the activation of the abdominal muscles varies with the angle during the two exercises, it can be concluded that the exercise angle is a contributing factor for strengthening of the abdominal muscles. Most of the previous studies have been focused on what kind of exercise is more helpful in strengthening the particular abdominal muscle, by comparing the muscle activities between the kinds of abdominal exercises [
256]. It is important to choose an exercise type for strengthening the abdominal muscles; however, it is thought that it would be helpful in strengthening the abdominal muscles and clinically necessary to understand and take into account the factors affecting muscle activities when prescribing the same kind of exercise. Recently, some papers have articles based on these topics [
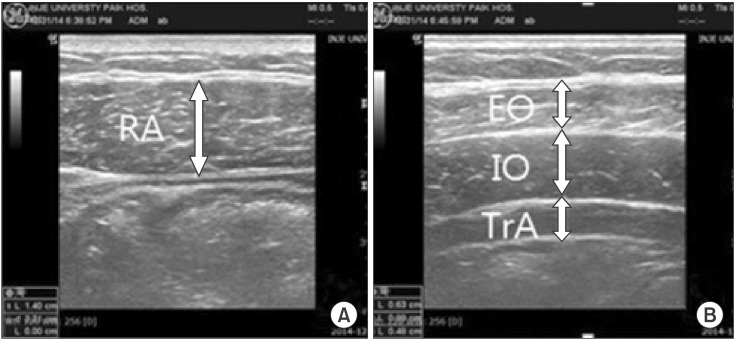
78]. Thus, in this study, we compared the levels of activation of the abdominal muscles depending on angles during the two exercises, by measuring the thickness ratio of abdominal muscles using ultrasonography (USG).
There are several studies that divided the rectus abdominis (RA) muscle into an upper part and a lower part, before comparing the levels of muscle activation according to location during the two exercises, using electromyography (EMG) [
3491011]. However, the results of previous studies were not coincident and we could not find a study using USG. It is considered to be clinically helpful in prescribing individualized exercises for persons relatively weak in particular parts of RA muscle to understand whether the RA muscle is selectively activated according to location; therefore, we thought that a study using USG was necessary. We also compared the activation of upper RA with lower RA during the two exercises using USG, after which we compared our results and the results of previous studies using EMG.
This study aimed to identify whether the exercise angle could be an important contributing factor for strengthening abdominal muscles, and whether the activation of RA is different based on the location, during the two exercises.
Go to :

RESULTS
The thickness ratio of the abdominal muscles at each angle during curl up exercise is shown in
Table 2, and during leg raise exercise in
Table 3. The muscle thickness ratio was significantly different depending on the angles selected for this study (30°, 60°, 90°) in URA and LRA for curl up exercise and leg raise exercise, but not in the lateral abdominal muscles for curl up exercise and leg raise exercise. In URA and LRA, the highest muscle thickness ratio was measured at 60° during curl up exercise, and at 90° during leg raise exercise.
Table 2
Curl up exercise: comparison of the thickness ratio of abdominal muscles by the selected angles and location


Table 3
Leg raise exercise: comparison of the thickness ratio of abdominal muscles by the selected angles and location

Also, there was no significant difference in the muscle thickness ratio of URA and LRA for curl up exercise-p=0.35 (30°), p=0.25 (60°), and p=0.13 (90°) by the two-sample t-test-and leg raise exercise-p=0.92 (30°), p=0.35 (60°), and p=0.37 (90°) by the two-sample t-test (
Tables 2,
3).
In the aspect of muscle activity, significant difference was seen in the activation of RA muscle by selected angles, but not according to location during both exercises.
Go to :
DISCUSSION
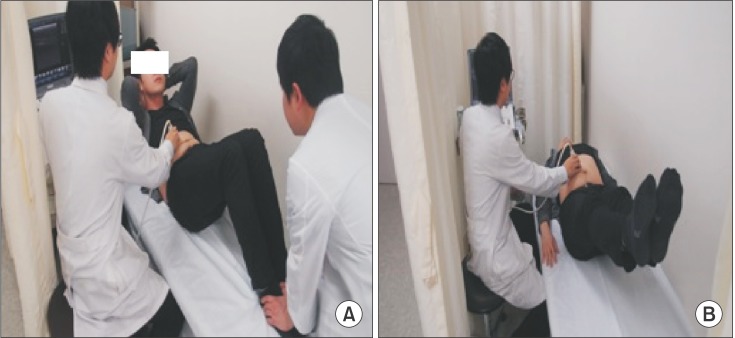
Muscle thickness change, as a surrogate marker for the level of muscle activation, was measured using ultrasound in abdominal muscles of 30 healthy adults during curl up and leg raise exercises performed at three different angles. Depending on different exercise angles, significant changes of muscle thickness was shown in the URA and LRA, but not in the lateral abdominal muscles. The activation levels of URA and LRA were not substantially affected by the two different abdominal exercises.
Based on the results of this study, the exercise angle is thought to be an important contributing factor for strengthening of RA muscle, because the muscle thickness ratio was significantly different, depending on the angles selected for this study (30°, 60°, 90°) in RA muscle. The highest muscle thickness ratio was measured at 60° during curl up exercise, and at 90° during leg raise exercise. It is clear that this study has some limitations in that, while not utilizing EMG, we measured the muscle activities by USG alone, and compared between the selected particular angles; however, it is thought that at least, increasing the exercise angle to more than 30° when doing the two exercises would be helpful in strengthening the RA muscle.
For the lateral abdominal muscles, no significant difference was found in muscle thickness ratio depending on the selected angles (30°, 60°, 90°) during the two exercises. We considered that lateral abdominal muscles might mainly act on the maintenance of trunk stability instead of the exercise motion itself, leading to the results differing from those of the RA muscle [
61216]. In addition, we thought that there might be differences in muscle activities depending on the angles when doing the exercises, including trunk rotation or lateral bending motions; it is considered that additional studies are needed to be conducted in the future.
Some studies have been reported recently on the factors affecting the abdominal muscle activation when performing the curl up exercise [
78]. In this study, we only examined whether the exercise angle is a contributing factor; however, we thought that exercise velocity or the presence of resistance at the time of exercise could also be factors that affect strengthening the abdominal muscles. It is expected that more helpful exercise prescriptions will be possible when prescribing similar exercises, if the studies on the various factors that affect strengthening the abdominal muscles are to be conducted continuously in the future.
We did not observe any difference in the muscle thickness ratio of URA and LRA at each angle in both exercises in this study. According to previous studies, the RA muscle is dominated by not only common nerve branch but also other nerve branches. In other words, each part of RA is controlled by a common part and at the same time, influenced by an independent part [
3]. Based on the above findings, there were several papers which compared the levels of muscle activation using EMG, under the assumption that there might be difference in the levels of RA muscle activation between upper and lower parts while performing curl up or leg raise up exercises [
3491011]. Several studies showed that the URA was more activated than the LRA during curl up exercise; however, the LRA was more activated during leg raise exercise. On the other hand, another study reported that there was no difference in the levels of muscle activation between the upper and lower parts of RA muscle during the two exercise regimens. Subjects, measurement locations, procedures and measurement devices are different in each study. Therefore, a large-scale study in future, which considers this risk of bias, is thought to be required. If difference in activation of upper and lower RA during trunk exercises is scientifically proven in future studies, individualized exercise can be prescribed for strengthening the relatively weak portion of RA muscle intensively.
In this study, we used USG to compare muscle activity instead of EMG. In many previous studies, abdominal muscle activation was evaluated by measuring the signal amplitude of EMG with surface EMG electrodes or needle electrodes. However, USG can also be a useful tool for evaluation, and has some advantages compared to EMG. Very few studies reported that it can be evaluation can be done based on changes in the thickness of abdominal muscles measured by USG. One study showed that changes in the thickness of TrA and IO muscles, as seen on ultrasound imaging, have statistically significant relation to the recruitment of TrA and IO muscles, as seen on EMG [
14]. Another study reported that the relationship between TrA muscle activation measured by EMG and its thickness change measured by USG was statistically significant [
15]. According to the study by Hodges et al. [
17], they ascertained that USG quantifies morphological changes in the muscle, including a change in thickness, and this quantified value can be a mean to define the levels of muscle activation. One more study showed that the relative change of the muscle thickness could be used as the indicator of the muscle activity in TrA and lumbar multifidus muscles [
18]. Two other studies also used USG as a tool for measuring abdominal muscle activation [
612]. Moreover, USG has several advantages compared to EMG. First, it is a non-invasive procedure and easy to perform when compared to needle EMG. Second, USG is able to measure changes in the abdominal muscle in a large area, and not just in a localized area. EMG is capable of detecting only those signals close to surface EMG electrodes or needle electrodes in a localized area. Third, needle EMG has a potential risk for subjects, such as pain and infection. Also, some factors exist that can influence the magnitude of the surface EMG signal. These factors include subcutaneous tissue under the electrodes, and muscle movement relative to the electrodes [
4]. In addition, USG turned out to be a reliable test in several studies because there was no statistically significant difference in the results of measuring the muscle thickness between the evaluators and during repeated measurements [
61214]. Although, it is still controversial whether USG is able to fully reflect the actual levels of muscle activation or not, we used USG in this study since it is non-invasive, easy to perform, and can reflect muscle activation of larger area than EMG.
In this study, standard deviations of the TrA muscle thickness ratio were relatively higher than the results of other muscles during both exercises, but especially during leg raise exercise. That is, the rates of change in muscle thickness were largely different among the subjects. From the results generated, we assumed that there might be differences in the levels of activation of TrA muscle depending on breathing and abdominal movements, as was observed in previous studies. One study reported that the TrA muscle was more highly activated by abdominal draw in maneuver for lower abdominal region, compared to other exercises [
5]. In another study, the TrA muscle was highly activated during the peak expiration [
6]. Therefore, even if the same exercise is performed, the exercise could be more effective depending on breathing and abdominal movements for TrA muscle.
There are several limitations in this study. First, the sample size of our study was small and most of the subjects were men. Since the subjects were only a small number of young men and women, is the data is insufficient to be generalized. Second, only muscle thickness was measured in this study, instead of other various morphological changes of muscles including cross-sectional area, length, and pennation angle. Third, we could not compare the levels of muscle activation appearing on USG and EMG, since we did not use EMG in this study. Further studies are required to measure the levels of muscle activation at different angles during both the above exercises using EMG, and compare with the results of this study. Lastly, we did not measure the muscle thickness by subdividing exercise angles more in detail during both exercises.
Based on the results of this study, the exercise angle is thought to be an important contributing factor for strengthening of RA muscle. Both exercises are thought to have no property of strengthening RA muscle selectively according to location.
Go to :


 PDF
PDF ePub
ePub Citation
Citation Print
Print



 XML Download
XML Download