

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lumbar radicular pain due to a herniated nucleus pulposus (HNP) causes significant morbidity [1]. Lumbar HNP compresses nerve roots and its mechanical and inflammatory mechanisms play a role in causing pain [2]. In patients with small contained herniations, outcomes after microdiscectomy are worse than sequestrated herniations [3]. There are variable treatment options including physiotherapy, medication and epidural steroid injection for symptom relief. If symptoms persist after sufficient conservative treatment, more invasive methods are required. The disadvantage of surgery is potential damage to posterior elements of lumbar vertebra [4]. The advantage of percutaneous procedure is the potential for decreased surgical trauma, quick recovery time, and the low incidence of complications. Therefore, minimally invasive disc decompression procedures for treating a herniated disc have been developed. Percutaneous disc decompression (PDD) methods rely on the principle that small amounts removed from the disc will result in significant pain relief by lowering the intradiscal pressure [5]. Therefore, pressure on the nerve will be removed and radicular leg pain will be relieved. Clinical significant pain reduction and decreased disability for patients and safety of PDD is proved [678] and it is frequently performed for treating radicular pain caused by lumbar HNP.
In order to treat lumbar radicular pain more efficiently, appropriate subject selection for PDD is important. This study aimed to investigate the correlation among clinical and radiological factors and the outcome of PDD in the patients with lumbar HNP.
Go to : 
MATERIALS AND METHODS
Subjects
The study was approved by the Korea University Institutional Review Board in 2015. We retrospectively collected and analyzed data from April 2009 to March 2013. Patients who underwent PDD by L'DISQ (U&I Co., Uijeongbu, Korea) were analyzed. The inclusion criteria of the study were as follows: radicular symptoms and signs with for ≥1 month despite conservative management (e.g., physiotherapy, selective nerve root blocks, and medication), and single-level lumbar HNP with neural contact as seen on lumbosacral spine magnetic resonance imaging (MRI) or MRI evidence of disc herniation with EMG evidence of lumbar radiculopathy. Patients with a progressive neurologic deficit including a cauda equine syndrome, previous lumbar disc operation, history of psychological disorder and radiological evidence of other pathologies that explain the clinical presentation (e.g., spinal stenosis and spinal cord tumor) were excluded.
Review of the radiographic findings and clinical data
We investigated the patients' medical records and MRI. We recorded the clinical characteristics and physical examination of the patients such as sex, age, smoking, duration of pain, and the result of the straight leg raising (SLR) test. The duration of pain that was longer than 6 months was defined as chronic pain. The straight leg raising test was considered positive when pain occurred before 60° passive elevation from horizontal [9].
One independent physician analyzed the MRI without previous knowledge of the patients' symptoms. The MRI images were classified by HNP level, HNP type, HNP zone, nerve root compromise grade, disc degeneration grade, and the high intensity zone (HIZ). Classification of HNP type, HNP zone followed the standards used by the American Society of Spine Radiology, the American Society of Neuroradiology, and the North American Spine Society [10]. HNP type was divided into 'protrusion', 'extrusion', and 'sequestration'. HNP zone consisted of 'central', 'subarticular', 'foraminal', and 'extraforaminal'. Nerve root compromise grade was classified as grade 0 (normal), grade 1 (contact), grade 2 (deviation), and grade 3 (compression) [11]. Disc degenerative grade was assessed by 5-scale degenerative grade by Pfirrmann et al. [12]. Grade 4 and 5 degeneration were defined as severe degeneration. The HIZ was defined as the local area with a high intensity signal in the posterior annulus fibrosus in the sagittal T2-weighted image [13].
Procedure protocol
PDD was performed on an outpatient basis. Preoperatively, prophylactic intravenous antibiotic was administered 30 minutes before the procedure. We monitored patients with electrocardiogram, pulse oximetry, and automated blood pressures. Sedative (20 mg of profopol) was administered as necessary during anesthetization of the skin and subcutaneous fascia.
The patients were placed in a prone position with the back mildly flexed on a surgical table. Fluoroscopic examination of the lumbar spine was performed to confirm intervertebral disc level and determine the appropriate level of needle [6]. We used a standard posterior lateral approach to the intervertebral disc, as previously described [14]; however, we modified the technique to approach the intervertebral disc more laterally so that the introducer needle would contact the disc margin rather than the midline.
A 25-gauge needle was first inserted into the ipsilateral side of target disc nucleus and 1 to 2 mL of contrast was injected to outline the disc herniation. Then, C-arm was rotated to position the lateral margin of the contralateral superior articular process as visualized in the oblique position. This typically required rotating the C-arm 15° from a zero-degree lateral projection. The skin and subcutaneous tissue were infiltrated with 1% lidocaine. We manually curved the 16-gauge introducer needle approximately 15° in the distal, 1 cm from the distal tip. The introducer needle was advanced toward the lateral edge of the superior articular process. Once the lateral edge was touched, we rotated the needle to point toward the midline. As the needle tip was directed toward the midline, the antero-posterior (AP) projection was checked intermittently to assure that the needle tip was always lateral of the medial border of the pedicle. The patient was asked to report any buttock or leg pain. The advancement of the needle was controlled by rotating the direction of the bent needle tip. Entering the herniation was identified by a sudden loss of resistance. After confirming the introducer needle position with the lateral and AP view, the wand was advanced to the center of the herniated disc under fluoroscopic monitoring (Figs. 1, 2). Before ablation, motor nerve stimulation was performed to confirm that the needle was not close to the nerve root. During the ablation, the tip of the wand was continuously rotated and moved back and forth to increase the ablated volume of the disc [6]. The entire procedure was monitored and evaluated by the C-arm fluoroscopy.
 | Fig. 1Percutaneous disc decompression was performed using L'DISQ catheter with fluoroscopic guidance. After the injection of contrast media, the C-arm fluoroscopic view shows the tip of wand (arrows) within a posterior lumbar intervertebral disc. (A) Lateral view, (B) anteroposteior view.
|
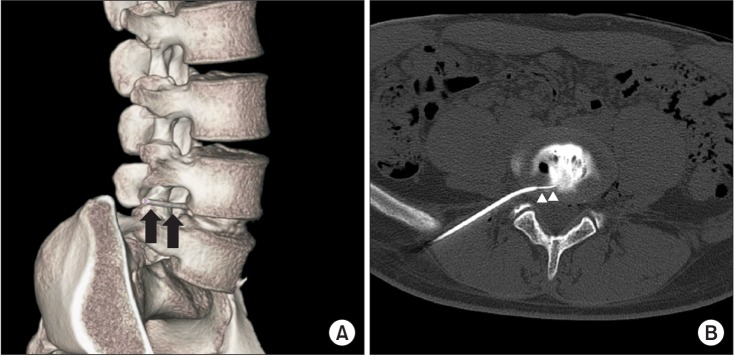 | Fig. 2A computed tomographic reconstruction image of the L'DISQ wand after percutaneous disc decompression (PDD) is shown. (A) The introducer needle (black arrows) was inserted posterior to the annulus fibrosus. (B) From the axial view of computed tomographic image, the tip of the PDD wand (white arrowheads) is seen within the intervertebral disc.
|
Outcome measures
The effectiveness of PDD was investigated using the visual analogue scale (VAS) and the Oswestry Disability Index (ODI). Baseline data was obtained before the procedure. After the procedure, patients visited our outpatient department and answered the VAS and the ODI after 1-, 3-, 6-, and 12-month. We defined the successful outcome as >50% reduction of the VAS.
Statistical analysis
The improvement of pain and disability after percutaneous disc decompression were analyzed by the Wilcoxon signed-rank test. The Mann-Whitney U test, the Kruskal-Wallis test were used for analysis of difference between the clinical outcome and the presence of the patients' clinical and radiological data such as sex, smoking, duration of pain, SLR test, HNP level, HNP type, HNP zone, nerve root compromise grade, disc degeneration grade and HIZ. The Spearman correlation analysis was used to measure the correlation between age and the clinical outcomes. Univariate logistic regression analysis was performed on each variables to determine the crude odds ratios of successful outcome. After that, multivariate analysis was performed by logistic regression using the above-mentioned independent variables, and the successful outcome of PDD as the dependent variable. Statistical analysis were performed using SPSS Statistics ver. 20 software (IBM, Armonk, NY, USA). Significance was determined when the p-value was <0.05.
Go to :
RESULTS
Sample characteristics
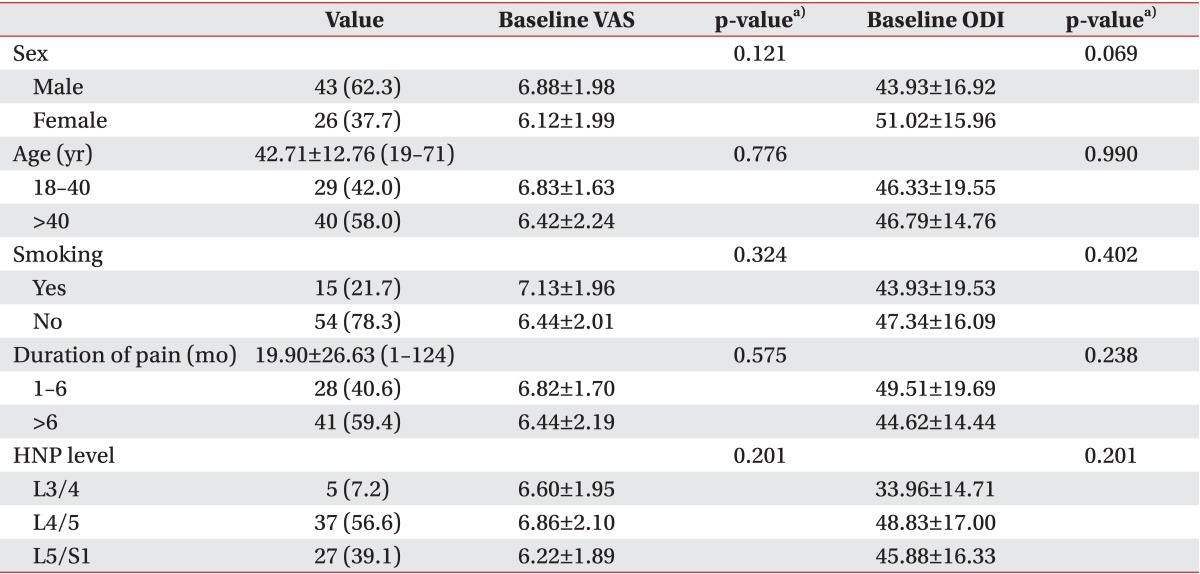
PDDs were performed in 109 patients from April 2009 to March 2013. Follow-up data were obtained in 83 patients. Seven patients were excluded due to prior lumbar surgery and 7 patients were excluded because of multi-level lumbar HNP. Sixty-nine patients, with mean age of 42.71 years (standard deviation of 12.76 years) were included in this study where 43 (62.3%) were male. Mean duration of symptoms was 19.90 months, ranging from 1 to 124 months. The basic clinical characteristics are shown in Table 1. There were no significant differences of baseline VAS and ODI according to subgroup analysis (Table 1).
Clinical outcome after PDD
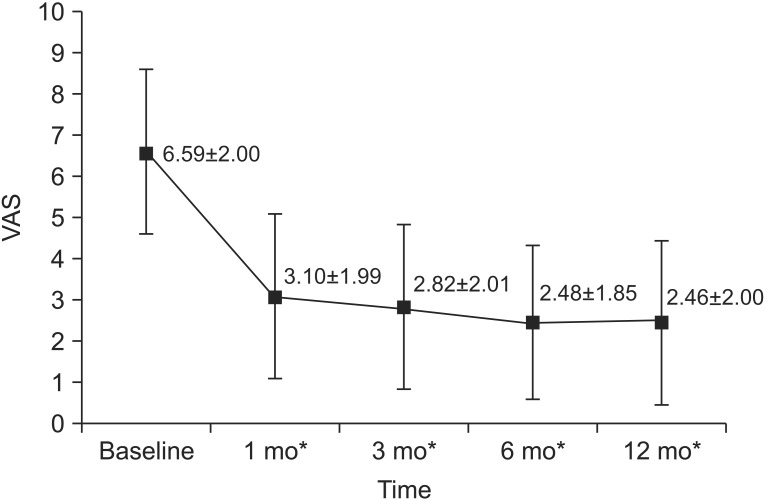
Clinical outcome was investigated through the medical records. The VAS score decreased significantly from 6.59±2.00 to 2.46±2.00 at 1 year evaluation (p<0.01) (Fig. 3). The ODI score significantly decreased from 46.60±16.80 to 25.02±16.68 at 1 year follow-up (p<0.01) (Fig. 4). Eight patients who had prolonged pain underwent conventional microdiscectomy after PDD. There were no major complications including nerve damage, epidural hematoma or spondylodiscitis.

The improvement of pain (ΔVAS) after PDD according to the clinical, radiological factors
The change of VAS according to the factors were presented in Table 2. The improvement of pain (ΔVAS) between the baseline and 1 year follow-up was calculated. There were no significant differences in baseline VAS among subgroups. One year after the PDD, ΔVAS of patients with their pain <6 months was significantly greater than that with chronic pain patients (p=0.03). ΔVAS was significantly different between the 3 groups by HNP zone (p=0.04). Post hoc comparison showed that ΔVAS of the subarticular HNP was considerably better than that of the central HNP (p=0.015). We were unable to compare the effectiveness in the extraforaminal zone since there were no patients enrolled. Difference of ΔVAS by SLR test showed borderline significance between the 2 groups (p=0.06). The following factors showed no significant differences with the ΔVAS: sex, smoking, HNP level, HNP type, nerve root compromise grade, disc degeneration grade, and HIZ. Age was not significantly correlated with ΔVAS by the Spearman correlation analysis (r=0.012, p=0.93).
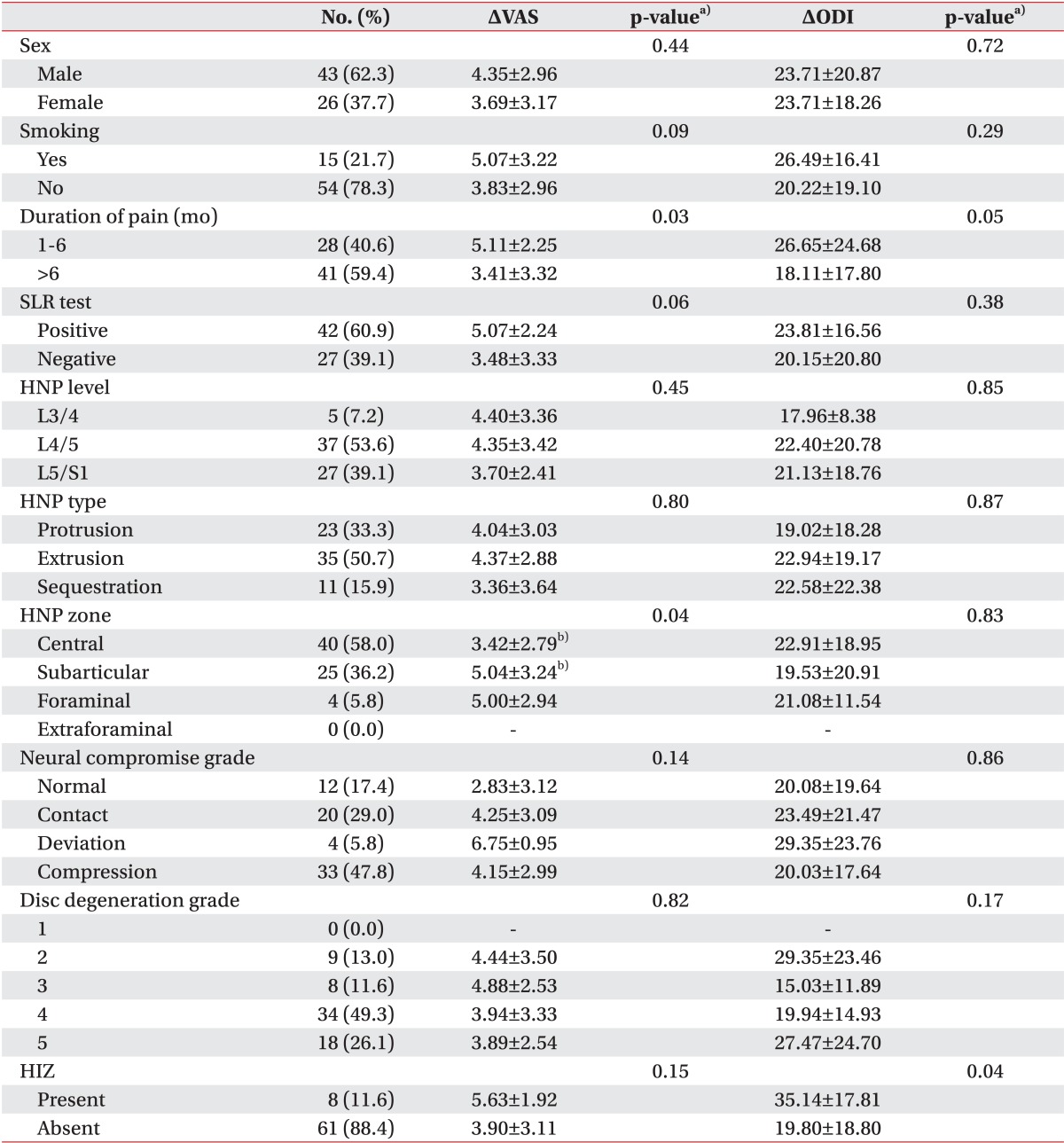
Table 2
The reduction of VAS (ΔVAS) and ODI (ΔODI) between baseline and 1 year follow-up after PDD according to clinical and radiological variables
Values are presented as number (%) or mean±standard deviation.
VAS, visual analogue scale; ODI, Oswestry Disability Index; HNP, herniated nucleus pulposus; SLR, straight leg raising; HIZ, high intensity zone; PDD, percutaneous disc decompression.
ΔVAS = VAS 1 year after PDD - baseline VAS
ΔODI = ODI 1 year after PDD - baseline ODI
a)The Mann-Whitney U test and the Kruskal-Wallis test.
b)Significant difference between two groups by the Mann-Whitney U test (p=0.015).
![]()
The improvement of disability (ΔODI) after PDD according to the clinical, radiological factors
The improvement of disability (ΔODI) between baseline and 1 year follow-up was calculated. The statistical differences of ΔODI among the various factors were analyzed. There were no significant differences in baseline ODI among subgroups. ODI of the patients with HIZ was significantly better than that of the patients without HIZ (p=0.04). Difference of ΔODI by duration of pain showed borderline significance between the 2 groups (p=0.05). ΔODI was not significantly different among sex, smoking, SLR test, HNP level, HNP type, HNP zone, nerve root compromise grade, and disc degeneration grade (Table 2). Age was not significantly correlated with ΔODI by the Spearman correlation analysis (r=-0.156, p=0.23).
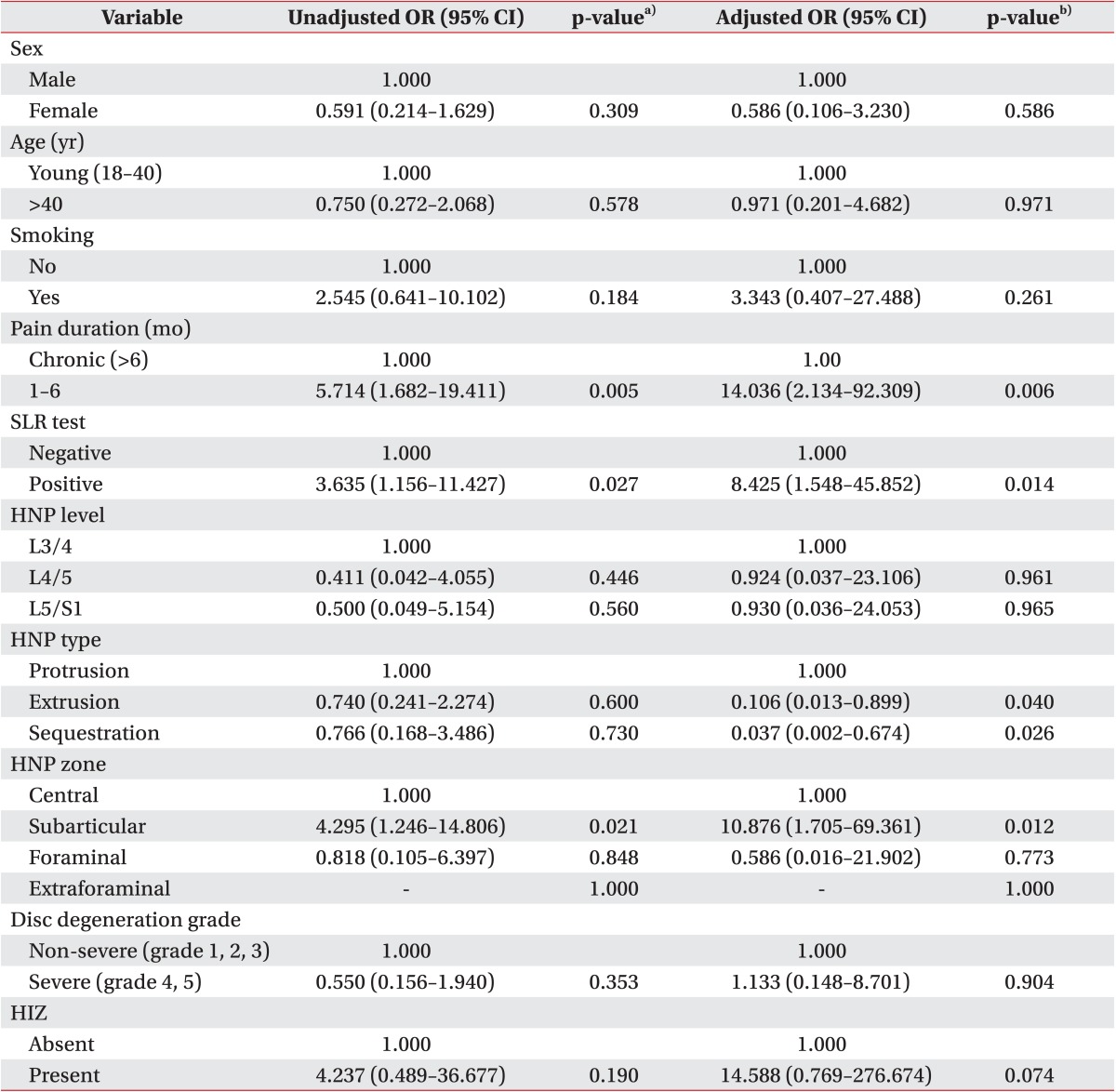
Associations with patient's clinical and radiological characteristics and the successful outcome of PDD
The associations between the successful outcome of PDD and patients' clinical and radiological characteristics were summarized in Table 3. Univariate analysis indicated significant differences for pain duration, SLR test, and HNP zone. Nerve root compromise grade was not calculated for the analysis because of small sample size in the deviation grade. When a dependent variable was set as a binary outcome by the presence of successful outcome after PDD, multivariate binary logistic regression analysis identified 5 independent predictors: pain duration of <6 months (odds ratio [OR], 14.036; 95% confidence interval [CI], 2.134-92.309), positive SLR test (OR, 8.425; 95% CI, 1.548-45.852), the extruded HNP (OR, 0.106; 95% CI, 0.013-0.899), the sequestrated HNP (OR, 0.037; 95% CI, 0.002-0.674), and the subarticular HNP (OR, 10.876; 95% CI, 1.705-69.361). HIZ (OR, 14.588; 95% CI, 0.769-276.674) showed borderline significance (p=0.074). No significant associations were observed for sex, young age (<40 years), smoking, HNP level, and severe disc degeneration.
Go to :
DISCUSSION
The factors that affect the success of PDD are still being studied [1]. To the best of our knowledge, this is the first study to analyze various clinical and radiological factors for predicting outcome after lumbar PDD. In this study, we evaluated the treatment outcomes of the PDD and investigated several clinical and radiological factors for predicting successful response of PDD. We found that VAS and ODI were significantly reduced after PDD for patients with lumbar HNP at 1 year follow-up. Pain improvement was better in patients with non-chronic pain and the subarticular HNP. Disability improvement was better in patients with HIZ. Patients with pain for <6 months, positive SLR test and the subarticular HNP were more likely to achieve the successful outcome after PDD. Patients with the extruded and sequestrated HNP were less likely to get the successful outcome after PDD.
An absolute indication for lumbar disc surgery is a progressive neurologic deficit including a cauda equine syndrome [15]. Except in that case, we should choose a proper management method to treat patients' pain and disability. A drawback of lumbar spine surgery is that it can damage posterior elements of lumbar vertebra by muscle dissection, bone removal or long surgical incisions [4]. PDD is performed with local anesthesia, so it is useful for those patients who cannot undergo conventional open discectomy under general anesthesia. Patients can also resume daily life activities more quickly.
Patients with lumbar HNP can undergo conservative treatment or epidural steroid injection to control symptoms. Conservative care provides resolution of symptoms, often coinciding with regression of HNP [16]. However, the natural history of HNP is often self-limited and pain gradually progresses over weeks or months. Erginousakis et al. [17] reported that PDD shows greater amelioration of symptoms at 12- and 24-month follow-up than conservative therapy. Another study showed that patients with a contained lumbar HNP who were treated with PDD had significantly reduced pain and disability than those treated using repeated transforaminal epidural steroid injection [7]. Therefore, better long-term outcome after PDD is expected. In the current study, the pain and disability were significantly reduced after PDD in lumbar HNP patients after 1 year follow-up. Thus, PDD can be recommended as an alternative treatment option after sufficient conservative treatment to treat radicular pain related to lumbar HNP in patients without progressive neurologic deficit.
Our study included patients with pain duration of >1 month. There are several studies to evaluate the efficacy of PDD that include patients with persistent symptoms for >4 weeks [6718]. We aimed to verify the effectiveness of PDD as a treatment options in patients with acute lumbar HNP. There were 14 patients whose pain duration was <3 months. Eight patients had epidural steroid injections but injections were not helpful. Six patients had severe pain (>7 VAS) and they were recommended surgery at other clinics. Because of severe pain, they could not tolerate conservative treatment and opted for non-surgical method. However, further study is needed to distinguish the effect of PDD and the natural history of lumbar disc herniation.
Karaman et al. [8] proved the effectiveness of PDD for chronic radicular pain. In our study, the patients with chronic radicular pain also showed significant pain and disability improvement 1 year after PDD (p<0.01). However, there was a significant difference of ΔVAS between chronic and non-chronic patients. One possible explanation is that chronic pain itself can modify sensory processing in the somatosensory system. Increased excitability, decreased inhibition and structural reorganization process in the spinal cord occur in chronic neuropathic disorders [19].
The SLR test as performed in clinical practice has a strong correlation with various parameters that signify the pain level of the patient [20]. A direct mechanical pressure by the lumbar HNP is the proposed explanation of positive SLR test. Positive SLR test was one of the factors associated with the successful outcome in our study. It can be explained by the effectiveness of PDD. By lowering intradiscal pressure and removing herniated disc, mechanical compression causing positive SLR test was thought to be successfully relieved after PDD.
From our study, the subarticular HNP showed better improvement of pain than the central HNP. Patients with the central HNP also showed significant pain and disability improvement 1 year after PDD (p<0.01), but the ΔVAS were different between the central and subarticular HNP groups. Knop-Jergas et al. [21] reported a poorer clinical outcome of central lumbar HNP than other HNP after lumbar discectomy. The reason seems to be the difficulty of approaching the central disc with a peculiar derangement of disc architecture. Approaching central HNP during PDD, also needs more effort because of its deep location. If we use conventional PDD devices, the difference of ΔVAS between the subarticular HNP and central HNP could have been greater than the result of this study. In contrast to most PDD devices, navigable PDD device (L'DISQ) has a flexible navigable tip that can be directed to the desired position by rotating control wheel, and this direct approach to the herniated disc material allows effective disc decompression [6].
Bokov et al. [18] studied that the size of the disc protrusion does not significantly affect the outcome of PDD, but PDD performed in cases of uncontained disc herniation have a significantly higher rate of unsatisfactory results versus microdiscectomy. Our study likewise showed that the successful outcome was associated with the HNP types by multivariate logistic regression. Patients with the extruded or sequestrated HNP also showed significant pain (p<0.01 and p=0.021, respectively) and disability (p<0.01 and p=0.026, respectively) improvement 1 year after PDD, however, they were less likely to achieve the successful outcome after PDD than patients with the protruded HNP. This result supports the previous principal that PDD is more useful in the contained disc. The decrease of pressure inside extruded and sequestrated disc could be lower than in cases of protruded disc herniations. The amount of ablated disc material could be different, but further research is needed for this hypothesis.
Our study showed that patients with HIZ had more disability improvement than those without HIZ after PDD. Kim et al. [22] reported that the incidence of HIZ was significantly higher in patients with acute severe lower back pain than in patients in the control groups. Kang et al. [23] also showed HIZ has meaning when it accompanies disc protrusion. On the basis of these studies, we can assume that HIZ with disc protrusion is associated with acute inflammatory process causing pain. Therefore, prompt removal of pathologic disc material could contribute to a better clinical outcome in this study.
There were some limitations in our study that should be considered in the interpretation of results. First, this was a retrospective study with a small sample sized; the VAS and ODI of 26 patients could not be evaluated because of lack of medical records. Secondly, we did not analyze patients' socioeconomic state or other comorbidity such as diabetes mellitus. Additionally, we did not measure herniation size, since all the patients had HNP less than 1/3 of spinal canal. Lastly, we used navigable PDD device, which may affect the clinical outcomes.
Our analysis identified the pain duration of <6 months, positive SLR test, the subarticular HNP, and the protruded HNP as predicting factors associated with the successful response of PDD in the patients with lumbar HNP. However, no significant associations were observed for sex, young age (<40 years), smoking, HNP level, and severe disc degeneration. We also confirmed the effectiveness of PDD in lumbar HNP patients with radicular pain. Further prospective studies should be undertaken to define this correlation.
Go to :
 XML Download
XML Download