

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Phantom limb pain (PLP) refers to the perception of pain in amputated limb or pain following partial or complete deafferentation. PLP is generally difficult to be treated. It often does not react to conventional pain treatments. The pathophysiology of PLP is poorly ascertainable. Peripheral and spinal mechanisms are considered to play a role in pain modulation in affected individuals. However, central mechanisms are also likely to be crucial. Deep brain stimulation has been reported to be effective. However, such procedure is invasive with various results depending on the patients [1]. Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive cortical stimulation tool. A number of studies have shown that rTMS can relieve chronic pain such as PLP [2]. A recent study has shown that amputees with PLP have significantly greater activation in primary motor cortex (PMC) and supplementary motor complex (SMC) of affected hemisphere compared to those without such pain [3]. Down-regulation of activity in PMC or SMC may relieve PLP. However, the effect of low frequency rTMS over PMC or SMC for PLP management remains unexplored. Here, we report the effect of 1 Hz rTMS over PMC and SMC for treating severe PLP by decreasing excitability of the stimulated cortical regions in a specific case.
CASE REPORT
A 37-year-old man visited our clinic with severe PLP on the first toe and dorsal aspect of the phantom foot at visual analog scale (VAS) 7 out of 10 and severe residual limb pain (RLP) at VAS 8 as well as phantom sensation (PSs). Additionally, he distortedly perceived somatic senses as pain. He also had severe constipation. He had a right transfemoral amputation due to an osteosarcoma eight years ago.
While previous pharmacological treatments and local injection therapies resulted in no substantial pain relief, he was treated with fentanyl transdermal patch (25 mcg/hr) and pethidine HCl 200 mg injection 4 to 5 times a week around his first visit to our clinic.
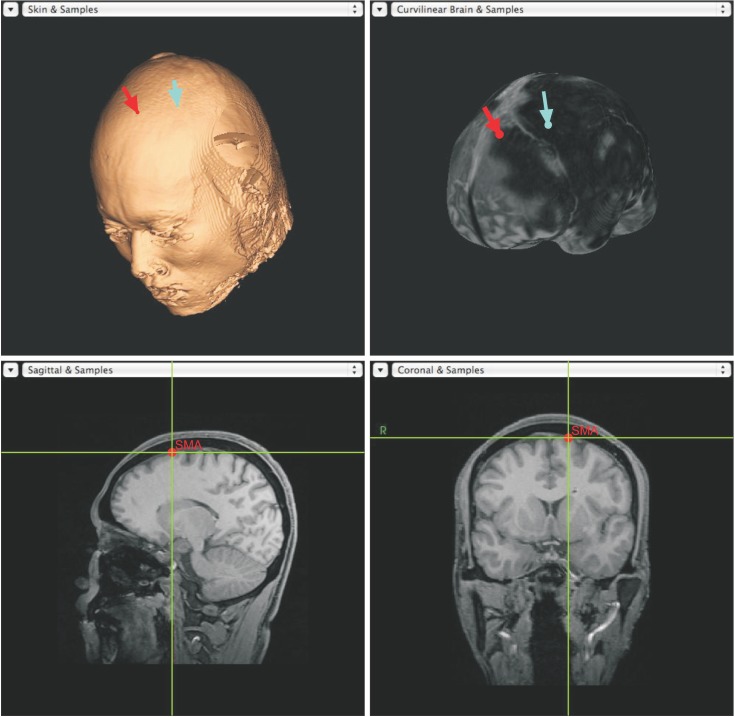
Physical and neurologic examinations and radiologic studies (brain MRI, whole body PET-CT, and ultrasonography on his right stump) showed no abnormality. rTMS was applied through a Double 70 mm Air Film Coil (Magstim Company, Whitland, UK) which was connected to a Magstim Rapid2 and Brainsight Frameless Navigation System (Rogue Research Inc., Montreal, Canada), a neuro-navigation system. Resting motor threshold (RMT) was determined using single-pulse stimulation over the left PMC. Motor evoked potentials were checked at abductor pollicis brevis muscle in the right hand. RMT was defined as the lower intensity required to elicit a motor evoked potential in 50% of successive trials. While measuring RMT, the identified location of PMC was stored and SMC in affected hemisphere was targeted using neuro-navigation system (Fig. 1). A total of 800 stimuli of 1 Hz at 85% of RMT per session were applied. A total of 6 rounds of treatment were performed over more than 1 year. The 1st round was used for PMC and the 2nd to 6th rounds were used for SMC. Each round of treatment consisted of 10 sessions (1 session per day) over 2 weeks. Before treatments, VAS, brief fatigue inventory (BFI), and Beck depression inventory (BDI) were checked. During treatments, VAS and BFI were reported daily while BDI was checked once a week.
For the 1st round of treatment, 1 Hz rTMS on the left PMC was applied. No pain reduction was found during treatment and 5 days or more thereafter.
During the 2nd round of treatment, 1 Hz rTMS was applied on the left SMC. After feeling reduction in pain, he arbitrarily ceased to use fentanyl transdermal patch (25 mcg/hr). Injection frequency of pethidine HCl 200 mg was also reduced. Thereafter, he suffered from rebound pains. Although the 2nd round of treatment showed certain pain relief, it was unreliable enough to explain the effect of rTMS over SMC due to the involvement of medication factor. He regained somatic senses. In addition, his constipation was improved.
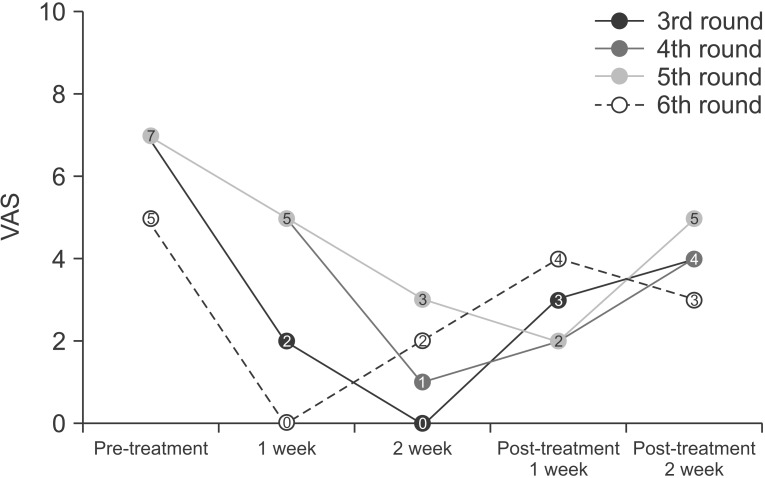
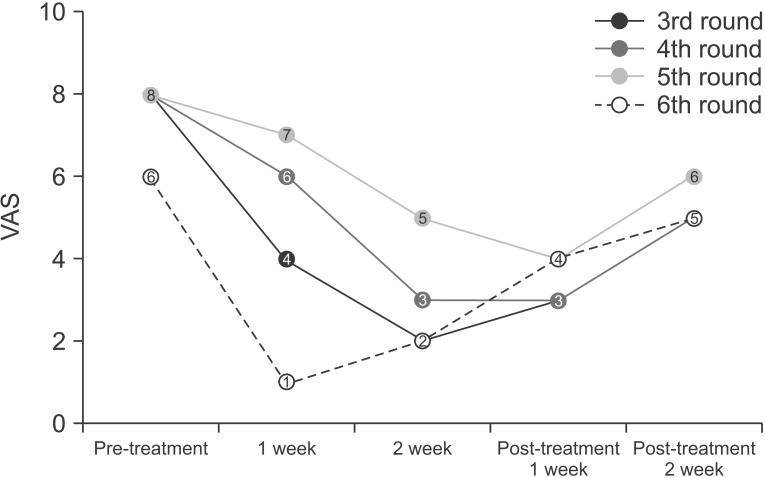
One and a half months later, he revisited our clinic due to uncontrollable PLP and recurrent RLP. Since he felt apparent positive effects of the 2nd round of treatment, the same treatment was applied onto the left SMC for the 3rd round. Result showed a dramatic decrease in VAS of PLP (from 7 to 0) and RLP (from 8 to 2) during treatment with slow return to pre-treatment condition for several months (Figs. 2, 3). Additionally, the treatment led to reduction in BDI (from 28 to 8) and BFI (from 74 to 38) as well as a disappearance of PSs (Table 1). Again, he reported recovery of somatic senses and improvement in constipation. He was advised not to cease drugs without clinical consultation. He would receive the rTMS treatment again if he suffered severe pains.
About 3 months later, he revisited our clinic. He reported that the pain relief effect was gradually diminished for 2 to 3 weeks after completion of the 3rd round treatment. The pain sustained at a tolerable level (VAS 4 or 5) for about 2 to 3 months. Thereafter, the pain started to increase up to VAS 7 to 8. His somatic senses were distortedly perceived as pain for a few weeks before his revisit to our clinic. Thus, the same treatments on SMC were performed. Previous positive effects were found. They sustained for about 2 to 3 months (for the 4th to the 6th rounds) (Table 1 and Figs. 2, 3).
DISCUSSION
Romero-Romo et al. [4] have proposed that the awareness of phantom limb is caused by activated basal ganglia-thalamocortical pathway due to the absence of afferent somatosensory-proprioceptive input from amputated limb. In their report of fMRI, increased excitability of contralateral SMC was found while basal ganglia-thalamocortical pathway was overactivated. According to Diers et al. [5], amputees with PLP have significantly greater activation in SMC compared to those without such pain. These reports indicate that there is a correlation between generation of PLP and excitability of basal ganglia-thalamocortical pathway and SMC. Therefore, we hypothesize that a vicious cycle of PLP operates as follows: 1) the awareness of the phantom limb is caused by activated basal ganglia-thalamocortical pathway; 2) the overactivated pathway increases the excitability of SMC; and 3) SMC reinforces the activation of basal ganglia-thalamocortical pathway, resulting in a vicious cycle of PLP.
In our case, it is possible that the down-regulation of SMC by application of 1 Hz rTMS might have broken the vicious cycle of PLP, thus leading to decreased PLP. In fact, the 3rd to the 6th rounds of treatment showed that application of 1 Hz rTMS over SMC reduced the PLP accompanied by reduction in RLP and PSs. Interestingly, suppression of SMC also led to the regaining of somatic senses, suggesting that down-regulation of SMC could affect functions of thalamus. Moreover, pain reduction continued for about 3 months after the treatment, suggesting that 1 Hz rTMS over SMC has relatively long-lasting analgesic effect. No specific side effect including impaired motor function was identified except blurred vision of the right eye which recovered soon after 1 Hz rTMS treatments. Such visual symptom could be due to inhibition of supplementary eye field related to eye movement.
Although there are some limitations such as absence of radiological proof showing activation of SMC and PMC and absence of focal selection of PMC related to the right amputated leg, this report suggests that application of a 1 Hz rTMS over SMC in affected hemisphere could be used as an effective treatment for severe PLP, RLP and PSs. Further studies with this approach are necessary to confirm its therapeutic results.

 XML Download
XML Download