

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cancer is one of the most common causes of death in the world. Recent innovations in cancer treatment have led to increased life expectancies, resulting in much attention paid to cancer rehabilitation therapy over the last 3 decades [123]. However, despite improvements in therapies, brain and other central nervous system tumors are associated with poor prognosis with a 5-year survival rate of 37.5% [4], and the diagnosis of a brain tumor can produce psychological distress. Additionally, the side effects of cancer therapies and brain tissue damage from tumor growth can result in significant neurological impairments and extensive functional disabilities.
Moreover, there are several barriers to overcome in those with brain tumors. First of all, the incidence of brain tumors in Korea is relatively low at approximately 3.4 cases per 100,000 per year [5]. As a result, neurosurgeons, neurologists and neuro-oncologists may not be sufficiently aware of the benefits of rehabilitation, and they may not provide referrals for rehabilitation services [6]. Another barrier is that physiatrists may not prescribe rehabilitation therapy to brain tumor patients with very short life expectancies. Finally, there is a lack of standardized guidelines regarding appropriate rehabilitation therapy for brain tumor patients.
However, as rates of disease-free survival have increased, and interest in the long-term sequelae and the quality of life in brain tumor patients has grown, recent attention has been focused on the importance of rehabilitation of brain tumor patients. Since it is impossible to assign a control group due to ethical issues, several studies have compared brain tumor patients with various neurological conditions that do make significant functional gains following rehabilitation [7,8910111213]. In particular, as disabilities after brain tumors are similar with those after stroke for which rehabilitation has been well established, some reports have compared the functional recovery of brain tumor patients with that of stroke patients [81415]. Kim et al. [15] reported that motor weakness and impaired cognition are the most common symptoms in both groups of patients. Hence, objective evaluation of cognitive dysfunction at baseline may be important to set the rehabilitation goal. The effectiveness of cognitive assessment and rehabilitation has been shown in other types of acquired brain injuries, such as stroke and traumatic brain injury [16171819]. However, in brain tumor patients, there are few randomized controlled trials or systematic reviews about interventions addressing cognitive functioning that include a comprehensive neuropsychological evaluation or assessment of the relationship between cognitive deficits and functional rehabilitation outcomes.
The purpose of our study was to identify the functional improvement in brain tumor patients after 4-week conventional rehabilitation therapy and to compare the cognitive impairment of brain tumor patients with that of subacute stroke patients using computerized neuropsychological testing (CNT) and determine the effects on functional outcomes of daily activity.
MATERIALS AND METHODS
Subjects
From April 2008 to December 2012, brain tumor patients and subacute stroke patients were enrolled in this study. A brain tumor was defined as a primary or metastatic lesion detected by computed tomography (CT) or magnetic resonance imaging (MRI) and confirmed pathologically by biopsy. Stroke patients had suffered a primary ischemic or hemorrhagic stroke as revealed by CT or MRI, and were diagnosed with a first-onset stroke within 3 months of stroke onset. All patients who could follow simple commands and complete the CNT were included. Patients unable to complete a questionnaire because of aphasia, visual and/or auditory problems, neglect, apraxia, or medical instability were excluded. All patients received conventional rehabilitation therapy for 4 weeks. The study protocol was approved by our local ethics committee.
Outcome measures
Assessment of cognitive function
All patients were assessed using a computerized neuropsychological test (CNT; MaxMedica Inc., Seoul, Korea) immediately after they were admitted or transferred to our inpatient clinic. The test was administered by another experienced physiatrist who was blind to the study protocol. The computerized neuropsychological test consists of a forward and backward digit span test, forward and backward visual span test, verbal learning test, visual learning test, visual continuous performance test (CPT), auditory CPT, word-color test, trail making test (parts A and B), and card sorting test [20].
The digit span test evaluated auditory attention and verbal short-term memory. It recorded the longest number that a person could repeat consecutively and in reverse using numbers that were randomly generated using a computer. Visual attention and non-verbal short-term memory, which correlated with visual information, were assessed via the forward and backward visual span test. This test recorded the highest numbers of circles for which a patient could remember the sequence after each of nine circles flashed randomly onto a computer monitor.
The visual and auditory CPT tests were used to evaluate the efficiency of auditory or visual attention. Patients were asked to push a button as soon as possible after the digit '3' was presented aurally or visually during a 9-minute period, and the correction numbers and commission error were recorded by the computer. The verbal learning and visual learning tests were used to evaluate encoding and recall abilities of verbal or visual memory. The computer aurally presented a 15-item word list and visually presented another 15-item figure list over five learning trials, after which the participants were asked to recall the words or figures. The total number of recalled words or figures was calculated by the computer program.
To evaluate selective attention related to frontal executive function, especially inhibition, a word-color (Stroop) test was used, and the time taken to read the word or color of the color word was calculated. The trail making test for visuomotor coordination consisted of two parts (A and B) that were to be performed as quickly and accurately as possible. In the type A trail making test, the patient drew lines sequentially connecting, in ascending order, 25 encircled numbers randomly located on the computer monitor. In the type B trail making test, the participant had to alternate between 13 numbers and 12 Korean letters while connecting them. The score on each part represents the length of time required to complete the task [21].
The card sorting test used a number of stimulus cards. The figures on the cards were different in design, color, and quantity. Four stimulus cards were shown in the upper row of the screen, and four response cards were shown in order in the lower row. By trial and error, the participant was asked to match up each of the stimulus cards. The computer responded to the answer with 'correct' or 'wrong'. Once the participant learned to sort by one rule, after six consecutive correct responses, the initial sorting principle was changed without warning, shifting to a new principle [22].
The cognitive functions of all patients were screened using the Korean version of Mini Mental Status Examination (K-MMSE) at baseline, and patients were followed-up after a 4-week rehabilitation intervention. A score less than 24 was defined as cognitive dysfunction.
Assessment of motor function and activities of daily living
The Motricity Index (MI) was used to assess motor impairment, and the hemiparetic side score (arm score for side + leg score for side) / 2 was measured. The MI of bilateral weakness due to bi-hemispheric tumor involvement was obtained from the average of the MI of both hemiparetic sides [23]. The Korean version of the Modified Barthel Index (K-MBI) was used to measure the functional status of patients in activities of daily living (ADL) [24]. Motor and ADL functions were assessed at the beginning and end of the intervention.
Conventional rehabilitation therapy
Physical therapy by NDT-certified therapists was provided for 1 hour per a day, and neuromuscular electrical stimulation therapy and aerobic exercise were also applied. In addition, patients also received occupational therapy for stretching and strengthening exercises of the upper extremity and task-oriented therapy for ADL, fine motor training, and sensory motor recovery. Generally, a routine rehabilitation program was provided during 4 weeks, but computerized or focused cognitive training on neuropsychological deficits were not prescribed to either group.
Statistical analysis
All statistical analyses were performed using the SPSS for Windows statistical package ver. 12.0 (SPSS Inc., Chicago, IL, USA). A Welch t-test was used to rule out differences between the malignant and benign groups as well as between the brain tumor and stroke groups. For relevant clinical outcomes, descriptive statistics (mean±standard deviation) were computed for each assessment. Pearson correlation analysis was used to assess relationships between daily activity functions and associated factors. Multivariate linear regression analysis (backward selection) was employed to determine whether there was a significant predictable factor of daily activity function before and 4 weeks after rehabilitation. A paired t-test was used to assess the motor (MI), ADL (K-MBI), and cognitive function (K-MMSE) scores at the beginning and end of admission. For a comparison of gender, lateralization, and cognitive dysfunction, a chi-square test was used. A p-value of <0.05 was considered statistically significant.
RESULTS
Demographic and disease-related characteristics at baseline
From April 2008 to December 2012, 29 brain tumor patients (17 females) and 26 subacute stroke patients (11 females) who were admitted or transferred to the Department of Rehabilitation Medicine of Asan Medical Center in Korea were enrolled in this study.
The brain tumor group consisted of 12 men and 17 women, with a mean age of 47.9±16.8 years and a mean interval between surgery or stereotactic biopsy and time of assessment of 25.5±13.4 days. Sixteen (55.2%), 8 (27.6%), and 5 (17.2%) patients had right-sided, left-sided, and bilateral brain lesions, respectively. Thirteen patients (41.4%) had been diagnosed with benign tumors and 16 (58.6%) with malignant tumors, with brain tumor recurrence observed in 10 patients (34.5%). There were no significant intra-group differences of all parameters according to gender and lesion side in both groups.
The stroke group consisted of 15 men and 11 women, with a mean age of 64.1±12.4 years and a mean interval between stroke onset and time of assessment of 28.1±13.1 days. Eleven (42.3%), 12 (46.2%), and 3 (11.5%) patients had right-sided, left-sided, and bilateral brain lesions, respectively. Twenty patients (76.9%) had been diagnosed with ischemic stroke and 6 (23.1%) with hemorrhagic stroke.
There were no intra-group differences except for age (p<0.01) and initial K-MBI (p=0.02) (Table 1). Although there were no significant differences between the motor functions of the groups, the initial K-MBI score of the brain tumor patients was lower than that of the stroke patients (p=0.02) (Table 1).
Comparisons of rehabilitation outcomes according to tumor grade (malignant vs. benign)
The histological findings of the malignant tumor (mean age, 43.3±15.9 years; 5 males and 8 females) and benign tumor (mean age, 47.1±18.3 years; 7 males and 9 females) groups were also compared. In the benign tumor group, 6 (46.2%), 4 (30.7%), and 3 (23.1%) patients were confirmed to have meningioma, low-grade glioma, and other tumor types, respectively. Six (46.2%), 5 (27.6%), and 5 (27.6%) patients had right-sided, left-sided, and bilateral brain lesions, respectively. In the malignant tumor group, 6 (37.6%), 5 (31.2%), and 5 (31.2%) patients were confirmed to have metastatic lesions, glioblastoma multiforme, and other tumor types, respectively. Ten (62.4%), 3 (18.8%), and 3 (18.8%) patients had right-sided, left-sided, and bilateral brain lesions, respectively. There were no intergroup differences except for the initial MI at baseline (p=0.017). All baseline variables are shown in Table 2.
Rehabilitation outcomes of cognition, motor, and daily activity functions
All brain tumor and stroke patients significantly improved after 4 weeks of rehabilitation treatment. Scoring of parameters associated with rehabilitation outcomes is shown in Table 2.
In addition, all malignant and benign tumor patients significantly improved after 4 weeks of rehabilitation treatment. Scoring of parameters associated with rehabilitation outcomes is shown in Table 3.
Computerized neuropsychological testing
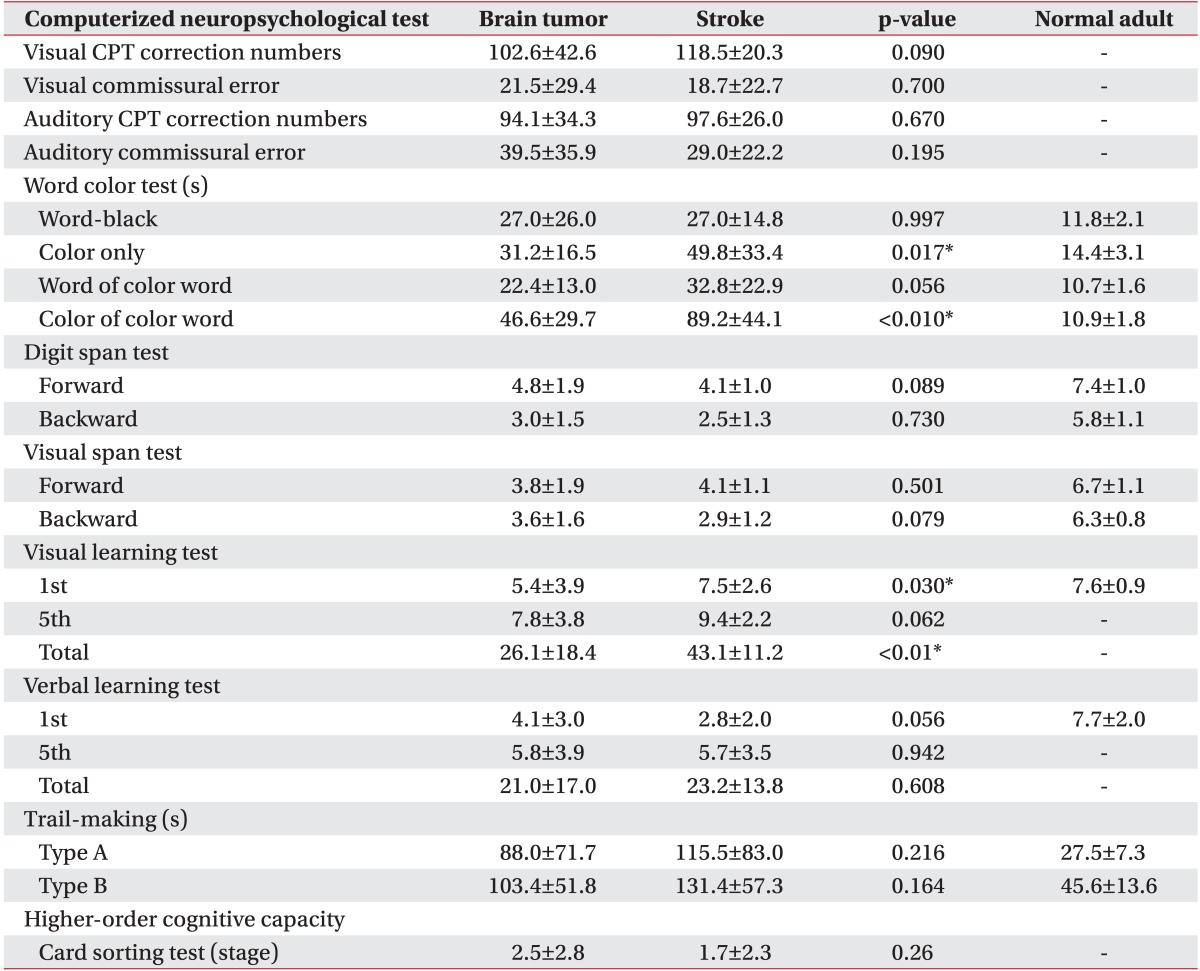
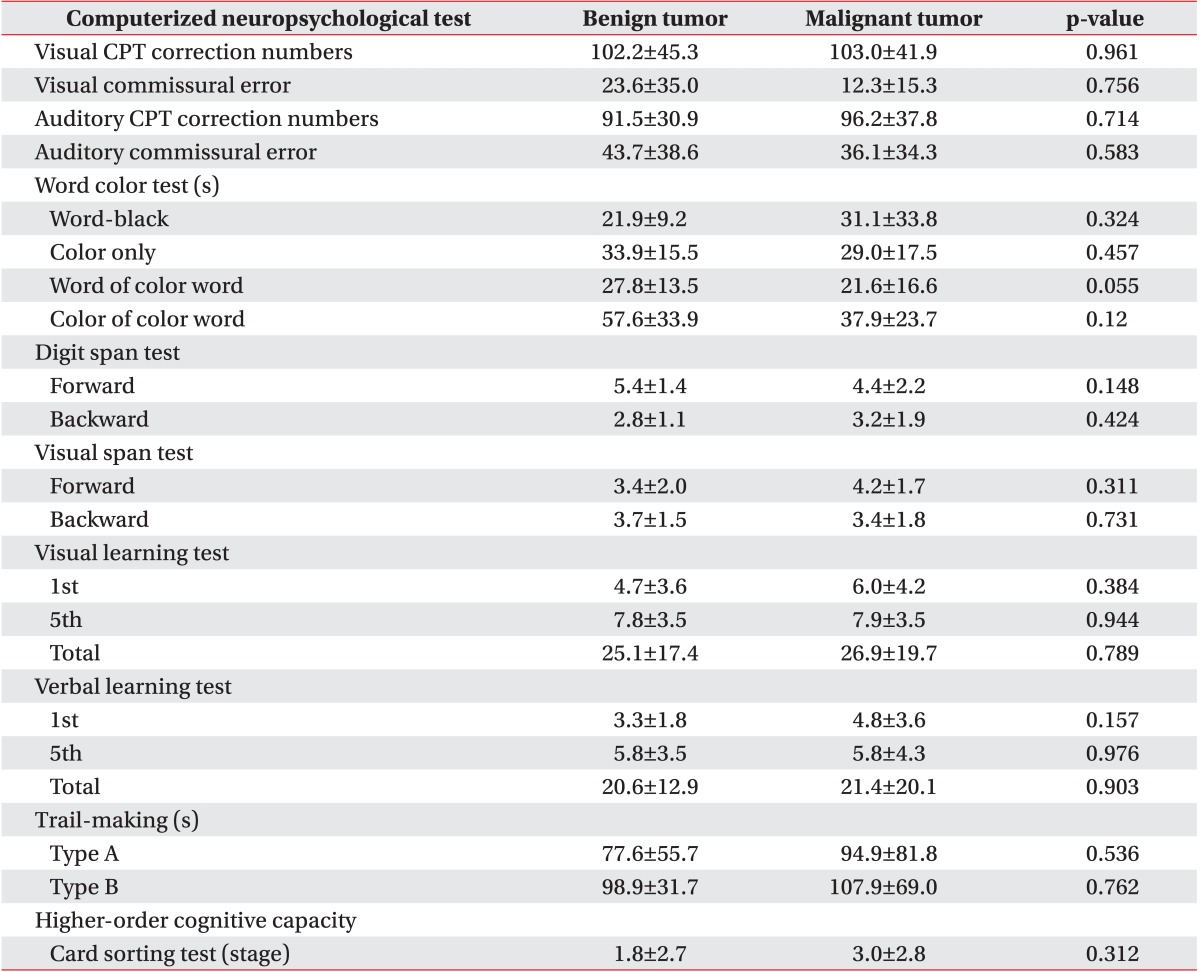
All variables of the computerized neuropsychological test in both brain tumor and stroke groups are shown in Table 4 and indicate cognitive impairment compared with normal adults. There were no statistically significant differences between the stroke and brain tumor groups in all tests except for the color only test, the color of the color word test, and the first and total visual learning tests. All variables of the computerized neuropsychological test in both benign and malignant tumor groups are shown in Table 4 and indicate cognitive impairment compared with normal adults. There were no statistically significant differences between the two groups according to tumor grade in all parameters of CNT (Table 5).
Correlation between daily functional outcomes and associated factors
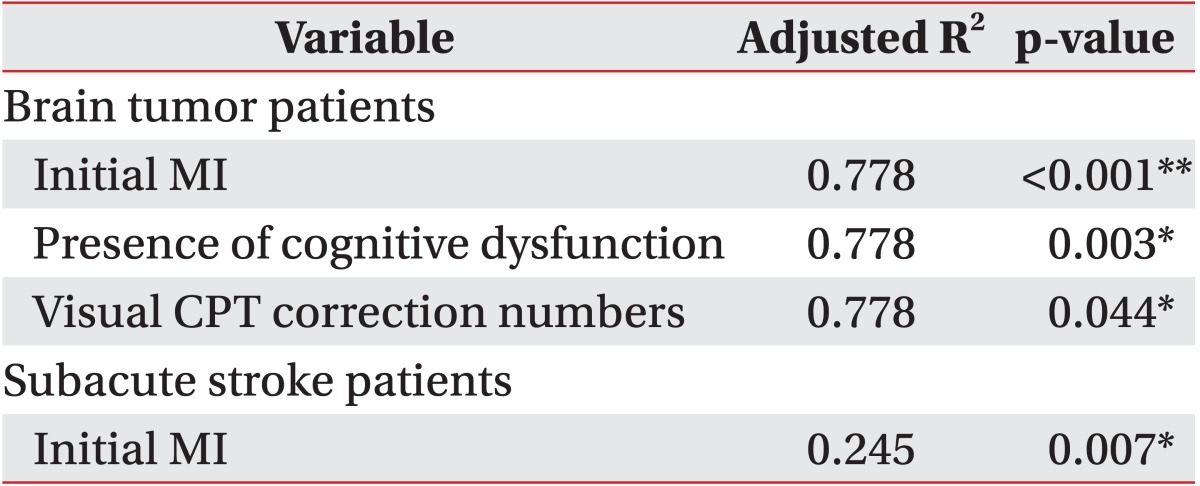
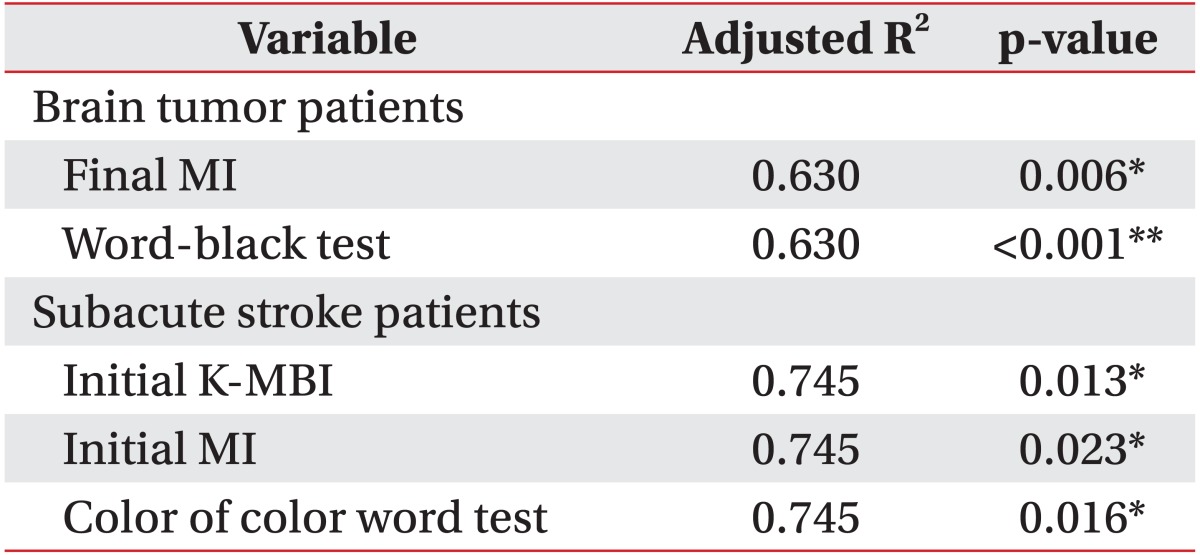
The initial K-MMSE scores of all patients correlated significantly with the subcategorized computerized neuropsychological test, except for the word of color word test, color of color word test, and trail making test type B. In patients with brain tumors, initial K-MBI scores correlated significantly with initial MI, cognitive dysfunction, visual CPT (correction numbers), word-black test, forward visual span test, and trail making test type A. Final K-MBI scores correlated significantly with initial K-MBI, final MI, word-black test, backward digit span test, and trail making test type A.
In patients with subacute stroke, initial K-MBI scores correlated significantly with initial MI. Final K-MBI scores correlated significantly with the initial K-MBI, initial and final MI, first visual learning test, color of color word test, and trail making test type A.
DISCUSSION
In our present study, cognitive dysfunction, which was assessed using objective subcategorized computerized neuropsychological testing, and its effects on initial and final rehabilitation functional outcomes were compared between brain tumor and stroke patients. These results demonstrated that impaired attention (visual) and motor and cognitive dysfunction (K-MMSE<24) affected the ADL function of brain tumor patients, and that impaired motor function affected the ADL function of stroke patients at baseline. Given that initial motor function and the number of patients with cognitive dysfunction were not statistically different between the two groups, a tendency to show poor results in the visual attention test might significantly affect the low daily activity scores of brain tumor patients at baseline. In addition, we found that after a 4-week rehabilitation, impaired selective attention (word-black test) and ADL functions at baseline and the final motor function affected final ADL function of brain tumor patients, whereas impaired selective attention (color of color word test), initial motor, and initial ADL function affected final ADL function of stroke patients.
Brain tumor patients usually suffer from cognitive impairments caused by both the tumor itself and its treatment, such as resection, chemotherapy, or radiation therapy [2526272829]. Furthermore, sensorimotor weakness and cognitive problems are common impairments in stroke and brain tumor patients [15]. However, most trials reported that the commonly used MMSE showed a lack of sensitivity to cognitive dysfunction at higher scores [303132]. In other words, an MMSE score within the supposedly normal range does not always indicate that the individual is free of significant cognitive problems, and the MMSE score alone cannot determine which cognitive domains have problems [30].
Only a few trials have assessed the cognitive function of patients with brain tumors by using comprehensive neuropsychological tests that evaluate the various cognitive domains, such as verbal and visual memory, executive functioning, attention, working memory, visuomotor coordination, and higher cognitive function [293334]. Duval et al. [33] reported a case study in which a comprehensive program for the rehabilitation of working memory and its effects on neuropsychological test performance and subjective cognitive functioning were sustained until a 3-month follow-up. Hassler et al. [34] performed neuropsychological assessments before and after intervention and observed a significant improvement in verbal learning. Gehring et al. [35] reported that a multifaceted cognitive rehabilitation program had positive effects on continued improvement in attention and verbal memory at the 6-month assessment in adult patients with lowgrade and anaplastic gliomas.
The Seoul Computerized Neuropsychological Test is a validated and objective method for comprehensive cognitive assessment with high inter-rater reliability in patients with brain injuries [23]. To the best of our knowledge, this is the first comparative study of cognitive impairment in brain tumor and stroke patients that used a computerized neuropsychological test. Although we did not follow the improvement of cognitive impairment by CNT, the majority of our patients revealed many deficits in the broad domains of attention, visual and verbal memory, visuomotor coordination, and frontal executive function at baseline, consistent with the above findings and irrespective of pathological histology. Moreover, we confirmed that attention deficits disturbed daily activity function in brain tumor patients at baseline and followup after 4 weeks and in subacute stroke patients at follow-up after 4 weeks. Therefore, attention should be paid to the cognitive as well as functional status of patients with brain tumors and stroke. In addition, not only conventional rehabilitation therapy, but also cognitive training focusing on specific deficits should be prescribed.
This study had several limitations, of which the most serious is the small number of patients evaluated. Thus, monitoring the effects of each treatment, including tumor resection, chemotherapy and radiotherapy, that might cause cognitive impairment could not be performed [36]. However, because many of the brain tumor patients had received resection and radiotherapy or chemotherapy simultaneously, there limitations might be attributed to clinical situations. Another limitation is the heterogeneity of lesion sites and tumor histology. Although malignant tumors were compared with benign tumors, further studies with a larger number of patients and groups subcategorized by histological type should be conducted. Third, several factors, including age and K-MBI, that showed statistical differences could also have an effect on the functional outcome after rehabilitation therapy. Although these factors were not correlated with final daily activity in regression analysis, this result should be proven in a large-scaled prospective study. Fourth, only cognitive status was assessed by the K-MMSE at discharge in the absence of follow-up computerized neuropsychological testing at discharge. As mentioned previously, a stable MMSE score over time does not necessarily indicate a stable cognitive function lacking significant changes [30]. Fifth, the brain tumor patients of this study could not be compared with brain tumor patients who did not perform rehabilitation therapy since it was impossible to assign patients to control group due to ethical reasons. Finally, a therapeutic intervention period of 4 weeks might be too short to demonstrate full recovery of patients with severe disability after stroke or brain tumor treatment since functional recovery of a stroke or brain tumor could be considered to require 6 months after onset [3738].
Further investigations, with larger numbers of patients, follow-up computerized neuropsychological testing, and long-term follow-up are warranted to assess the effects of cognitive training on cognitive and functional outcomes in brain tumor patients in terms of the brain lesion and tumor histology type.
In conclusion, patients with subacute stroke and patients with brain tumors reveal deficits in the broad domains of attention, visual and verbal memory, visuomotor coordination, and frontal executive function. In particular, attention deficits of patients with brain tumors affect functional outcomes both at baseline and after a 4-week intervention. Therefore, an objective cognitive evaluation should be performed in brain tumor patients for improving their daily activity function and quality of life.



 XML Download
XML Download