

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cerebral palsy (CP) describes a group of disorders in movement and posture that limits activity and is attributed to disturbances in the developing fetal or infant brain [1]. Treadmill walking exercise may improve walking activity in children with CP, as it provides an opportunity to repetitively train the entire gait cycle and facilitate an improved gait pattern [2]. Treadmill walking exercise has been associated with increases in strength and decreases in energy expenditure [3]. Moreover, partial body-weight supported treadmill walking exercise to reinforce the pattern of walking achieved on the treadmill has been used to force an increase in walking speed and distance [4]. Several preliminary studies suggest partial body-weight supported treadmill walking exercise as effective in improving walking among ambulatory children with CP [2,3,4,5] and post-stroke locomotion recovery [6,7]; however, there are few studies on ambulatory adults with CP without a body-weight support. Therefore, more research is needed to determine whether treadmill walking exercise is effective for adult CP patients who usually show decline in walking activity and aerobic capacity [2,3,5].
Oxygen consumption (VO2) is considered as the gold standard for assessing energy expenditure during an activity [8]. Walking energy consumption is a valid evaluation of walking performance in individuals. Gait disabilities, such as CP and stroke, increase the energy expenditure of walking and the intensity of physical effort with altered walking speeds [9]. Our study was designed to evaluate the effect of a treadmill walking exercise as a mean of improving the energy expenditure of walking and gait efficiency in adults with CP. We also determined improvement in parameters such as gait speed, distance and energy consumption during overground walking or treadmill walking in response to such exercise in ambulatory CP patients.
MATERIALS AND METHODS
Participants
Fourteen ambulatory adults with CP (7 male and 7 female; mean age of 28 years) were recruited to the treadmill walking exercise experimental group. A control group of 7 adults with CP, who attended conventional physical therapy alone, were also recruited. This study was approved by the Institutional Review Board (IRB No. 4-2008-0624). Total 21 CP participants were randomly allocated to either the experimental or control group at a 2:1 ratio, using a central telephone randomization service [10]. Inclusion criteria were as follows: the ability to ambulate independently indoors without a gait aid and the ability to follow verbal directions for standardized testing. The following were used as exclusion criteria: orthopedic surgery such as musculotendinous lengthening and femoral derotation osteotomy, neurosurgery such as selective dorsal rhizotomy and intrathecal baclofen pump implantation, or botulinum toxin injection into gastrocnemius, medial hamstring and hip adductors in the past 12 months, and clinically evident unstable cardiac status, or any premorbid conditions. All participants in the experimental group performed a treadmill walking exercise for 30 minutes and conventional physical therapy. The treadmill walking exercise protocol for the current study consisted of 3-5 training sessions per week for 1-2 months (total 20 sessions). Participants in the control group received conventional physical therapy in the same sessions.
Six-minute walking test
The 6-minute walk is a reliable and valid measure of walking endurance. The instructions for the test are standardized according to Lipkin et al. [11]. For the 6-minute walking test during overground walking, the patients were encouraged to walk as fast as possible while not running, and the total walking distance was recorded. If the patients could not maintain overground walking for 6 minutes, they finished the walking endurance test, and the distance walked until the time was measured.
Measurement of energy expenditure
Energy expenditure was examined during treadmill walking at a self-selected comfortable speed and overground walking on the first and the last day of treadmill walking exercise. The energy expenditure was measured using KB1-C oximeter (AeroSport Inc., Ann Arbor, MI, USA). Oxygen consumption of walking is the volume of oxygen consumed per kg of body weight for a given time. Oxygen rate of the experimental subjects using a breathing mask were analyzed with oxygen gas analyzer built into the computer. Oxygen uptake per minute (VO2, mL/min), carbon dioxide production amount per minute (VCO2, mL/min), respiratory volume per minute (VE, L/min), oxygen consumption rate (O2 rate, mL/kg·min), and oxygen consumption cost (O2 cost, mL/kg·m) were measured. The O2 cost was determined by dividing O2 consumption by the velocity of walking, as an indicator of the gait efficiency [9].
Statistical analysis
Wilcoxon signed-rank test for paired samples before and after treadmill walking exercise was used to compare the parameters of energy consumption test during treadmill walking or overground walking. Additionally, Mann-Whitney U test was used to compare the parameters of Δdistance, Δvelocity, ΔO2 rate, and ΔO2 cost calculated by the subtraction from post-treatment to pre-treatment values between experimental and control groups. All statistical analyses were performed using SPSS ver. 20.0 (IBM SPSS Inc., Armonk, NY, USA). A value of p<0.05 was considered statistically significant.
RESULTS
General characteristics of subjects
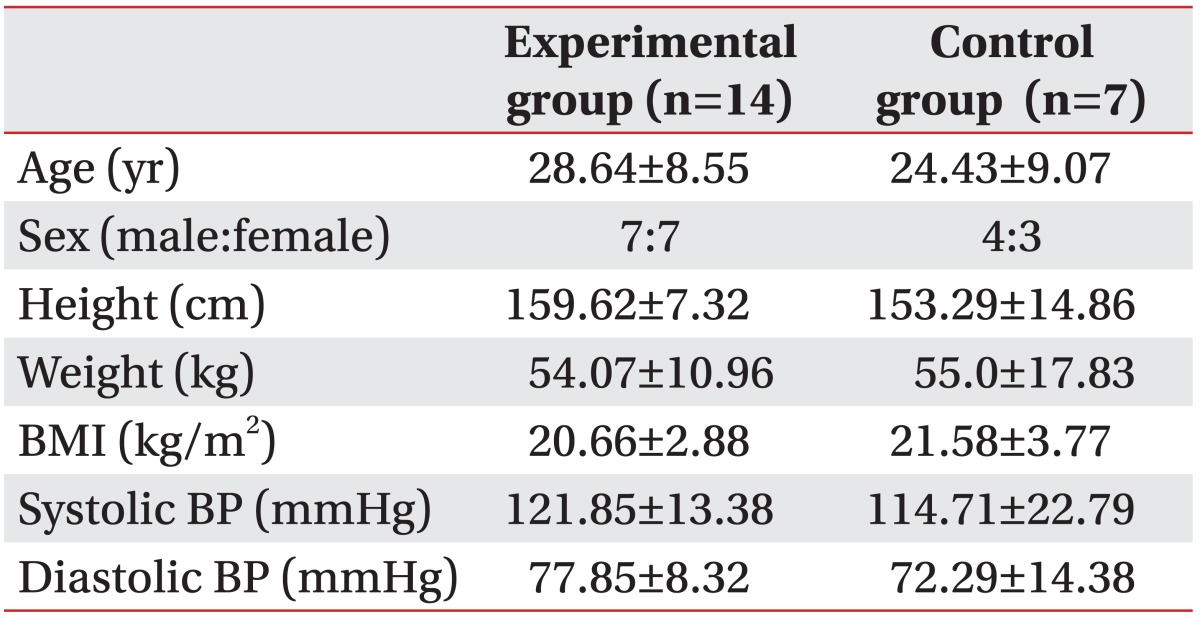
General physical characteristics of the experimental and control groups were described in Table 1. Total 21 adults with CP (11 men and 10 women) consisted of 14 in the experimental group (7 men and 7 women) and 7 in the control group (4 men and 3 women). There were no significant differences in age, sex, height, weight, body mass index, systolic blood pressure, and diastolic blood pressure between the two groups of CP patients (Table 1).
Changes in the parameters of energy consumption test during treadmill walking
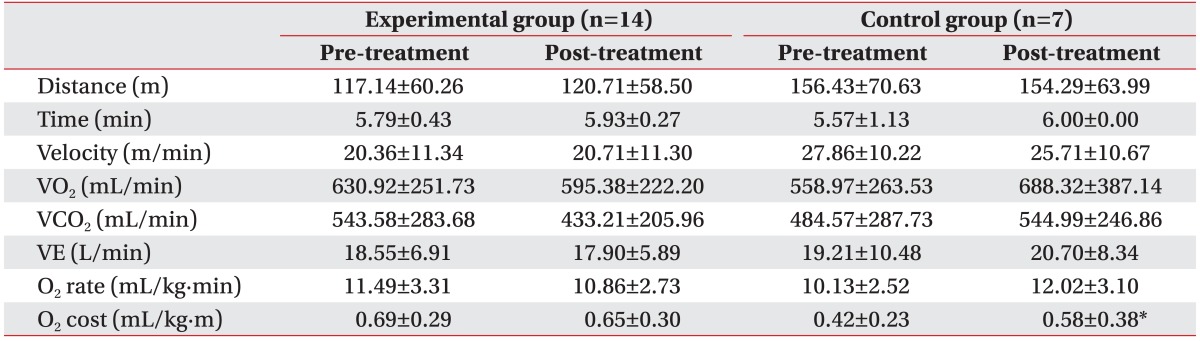
The results collected on a treadmill after treadmill walking exercise or conventional physical therapy was shown in Table 2. There were no significant changes in all the parameters, such as walking distance, time, velocity, VO2, VCO2, VE, and O2 rate between the pre-treatment and post-treatment states (Table 2). However, energy expenditure per meter, O2 cost was significantly increased from 0.42±0.23 to 0.58±0.38 mL/kg·m after conventional physical therapy in the control group (p=0.046), suggestive of an increase in energy expenditure with no improved gait efficiency during treadmill walking (Table 2).
Changes in the parameters of energy consumption test during overground walking
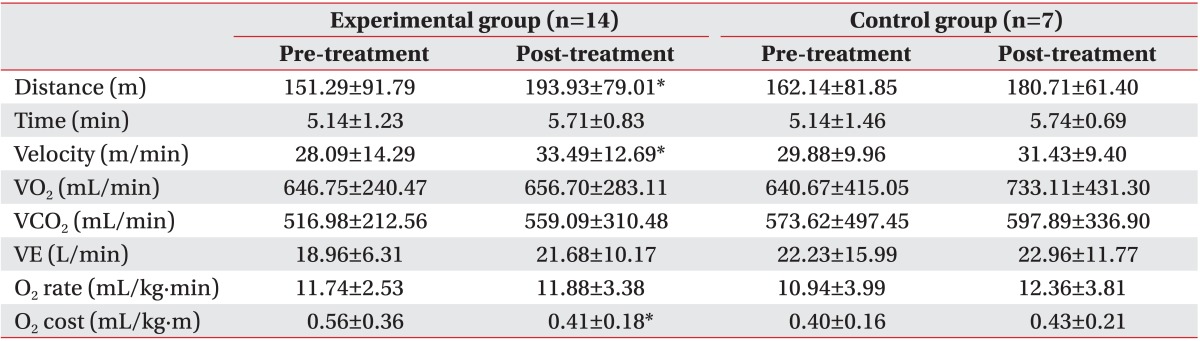
The results obtained during overground walking up to 6 minutes after the treadmill walking exercise or conventional physical therapy was described in Table 3. After the treadmill walking exercise, the experimental group showed that gait distance significantly increased from 151.29±91.79 to 193.93±79.01 m, and gait velocity increased from 28.09±14.29 to 33.49±12.69 m/min (p=0.048 each) (Table 3). Moreover, O2 cost was significantly decreased from 0.56±0.36 to 0.41±0.18 mL/kg·m in the experimental group (p=0.03), suggestive of an improved gait efficiency post-treadmill walking exercise (Table 3). In contrast, there were no significant changes in the control group.
Comparison of energy expenditure parameters between experimental and control groups
The parameters of energy consumption test, such as the difference between post-treatment and pre-treatment states (Δ) in the O2 rate and the O2 cost, were then compared between experimental and control groups. As a result, there were no significant differences in the ΔO2 rate during both treadmill walking and overground walking between the two groups (Fig. 1A, B). However, the experimental group showed significantly lower ΔO2 cost (-0.15±0.18 mL/kg·m), as compared with the control group (0.04±0.05 mL/kg·m) during overground walking (p=0.04) (Fig. 2B), although the ΔO2 cost was not significantly different between the two groups during treadmill walking (Fig. 2A).
DISCUSSION
A previous study suggested that individuals with CP are less active and more sedentary than their able-bodied peers [12]. Children and adolescents with CP tend to participate in less structured and lower intensity physical activities. A vicious cycle of exposure to lower physical activities in persons with chronic illness or disability leads to further deconditioning and physical deterioration [13]. Children with CP at the age of 7 have already lowered VO2 peak values compared to typical developing peers. Therefore, early intervention for an active lifestyle might be beneficial for promoting physical fitness in CP patients [14].
Schindl et al. [15] reported the effects of body-weight supported treadmill walking exercise as a treatment method to improve the physical fitness in children with CP who were mostly non-ambulatory; their data demonstrate relevant improvements in motor abilities. Activity patterns shift towards aerobic activity in adulthood, making aerobic capacity more important with increasing age [14]. Therefore, there was a need for studying adult subjects in treatments to improve aerobic capacity and physical fitness, such as treadmill walking exercise. We focused on adult patients with CP who have ambulatory function.
Oxygen uptake measures may be the best method to quantify gait efficiency during functional walking. Bowen et al. [16] reported O2 cost as a more reliable measurement of energy expenditure than VO2 alone. O2 cost is determined by dividing O2 consumption by the walking speed (mL/kg·m) as an indicator of gait efficiency. Duffy et al. [17] demonstrated that the O2 cost was significantly higher in children with spina bifida and CP compared to healthy children. In this study, ambulatory CP patients in the experimental group increased their walking distance and gait velocity, leading to a decrease in the O2 cost during overground walking after treadmill walking exercise. It suggested that treadmill walking exercise characteristically improved the gait efficiency during overground walking.
When the O2 cost of walking on a treadmill with those of overground walking is compared after treadmill walking exercise, it is possible to clarify the gait efficiency of both conditions. Little is known about the differences in the O2 cost on a treadmill versus overground walking; hence, a study must be conducted to determine the more efficient O2 cost in order to verify gait efficiency for treadmill training. As a result, the O2 cost measured during overground walking was significantly improved, as compared with the O2 cost during treadmill walking, suggestive of improved gait efficiency during overground walking in ambulatory patients.
The effects of treadmill training on overground walking speed have been reported [2]. On the other hand, preferred walking speed determined on a treadmill is slower compared to overground, leading to higher O2 cost on the treadmill, although the treadmill is often used to simulate overground walking [9]. Recent evidence indicates that when the direction of walking is the same for the 2 conditions, similar neural networks may be involved; however, when on the treadmill, subjects do not move through space as they do during overground walking. These contextual differences arise from the lack of visual and somatosensory information during treadmill walking. It is possible that these identifiable differences in task context are sufficient to transfer from the treadmill walking exercise to a more natural overground walking environment with more efficient gait [18].
In conclusion, treadmill walking exercise improved gait efficiency in adults with CP. It has been associated with decreased energy expenditure measured by O2 cost during overground walking. Therefore, treadmill walking exercise can be an important method for gait training in ambulatory CP patients who have higher energy expenditure and lower gait efficiency.


 XML Download
XML Download