

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of feeding problems has been estimated to be from 33% to 80% in children with developmental disorders [1,2]. Feeding and swallowing disorders during childhood are increasing. They typically occur in conjunction with multiple and complex medical and developmental conditions [3,4]. Approximately 37% to 40% of children assessed for feeding and swallowing disorders were born prematurely at less than 37 weeks of gestation [5,6]. Increased survival rates of children with histories of prematurity, low birth weights, and complex medical conditions might explain the recent increase of pediatric dysphagia [7].
Swallowing is a dynamic process. Videofluoroscopic swallowing study (VFSS) is generally considered as a reliable and safe method to evaluate dysphagia in pediatric population [8]. Nonetheless, the procedure exposes children to radiation. In addition, it provides only a brief sample of swallowing performance which can be an unpleasant and frightening experience for some children. Increased use of VFSS in the pediatric population has led to queries regarding the overuse of VFSS in evaluating swallowing difficulties [9]. The benefits from the use of the test should be weighed against its risks, particularly if its use involves infants. Therefore, before considering a VFSS referral, a review of medical, developmental, and feeding history should be conducted to comprehensively evaluate children with dysphagia.
At present, standard clinical assessment tool for pediatric dysphagia has yet to be validated. Indicators have not been established to determine when a VFSS is necessary. Consequently, evaluating the severity of dysphagia is more challenging in children than in adults. Moreover, there is little understanding on the characteristics of children with severe dysphagia, especially those with etiologies other than neurologic disorders. The purpose of this study was to evaluate demographic data of children with suspected dysphagia referred for VFSS, including age, prematurity, underlying medical conditions, reason for referral, and diet status at the time of the study to identify clinical factors related to penetration or aspiration confirmed by VFSS.
Go to : 
MATERIALS AND METHODS
Subjects
The study included 352 children under 19 years of age who were referred for VFSS from January 2006 to December 2011. Their developmental and medical histories in medical charts were reviewed in details. Subjects included 197 boys and 155 girls with a mean age of 49.3 months (standard deviation, 56.8 months). For subjects who underwent more than one VFSS, data from the first VFSS were used. Subjects were divided into five groups based on normal developmental feeding behavior. Generally, infants under 6 months are breastfed or bottlefed. Progression to a transitional diet (weaning food) is completed between 7 months and 2 years. At the age of 6 years, coordination of mastication matures [10]. Children begin elementary school when they are 7 years old, and those between 13 and 18 years of age are classified as adolescents.
We used adjusted age during the first 24 months of life in preterm infants with less than 37 weeks' gestational age [11]. For example, a child born at 33 weeks' gestational age whose chronological age was 12 months was assigned an adjusted age of 11 months. For children older than 25 months, age was described in years. Assumption for feeding behavior and swallowing safety was estimated based on age and overall developmental status of the subject.
Videofluoroscopic swallowing study
VFSS was performed using a Hitachi Medix 3000 table unit fluoroscope (Hitachi Medical Corp., Tokyo, Japan). Frame-by-frame images were acquired as digital imaging files using a computer-based image processing system equipped with a digital frame grabber board (Pegasus HD/SD Board; Grass Valley Inc., Honorine, France). A clinician experienced in feeding and swallowing disorders conducted each study. Subjects were placed in upright sitting position during the studies. For those who were unable to maintain a sitting posture, a reclining position was adopted.
VFFS was performed using protocol initially described by Logemann [12] with modifications. Parents prepared bottles or weaning food, if indicated. All bottled milk or weaning diet was mixed with liquid barium immediately prior to VFSS. For infants, bottled milk mixed with liquid barium was presented initially. For infants older than 6 months, curd-type yogurt or prepared weaning food was presented subsequently. For children older than 1 year, 2 and 5 mL of diluted barium (35% wt/vol), pudding, curdtype yogurt, rice porridge, and steamed rice in a spoon were used. Food was given to the children by a physiatrist or family caregiver. Images were analyzed by a clinician under the supervision of a senior clinician who had at least 2 years' experience with VFSS. Common VFSS findings in pediatric patients included delayed pharyngeal swallow and the presence of supraglottic penetration, nasopharyngeal reflux, and aspiration [13]. Penetration and aspiration, a major finding equally applied in variable pediatric age groups, was chosen as the primary outcome among those with pharyngeal phase abnormalities. Penetration was defined as the passage of contrast materials into the larynx but not through vocal cords. Aspiration was defined as the passage of contrast materials below true vocal cords [14].
Statistical analysis
Frequency analysis and descriptive statistics were used to summarize demographic data. Chi-square test and univariate analysis were used to identify the relationship between demographic factors and penetration or aspiration. Multivariate logistic regression analysis was used to identify independent factors related to penetration or aspiration. All statistical analyses were performed using SPSS ver. 20.0 (IBM SPSS Inc., Armonk, NY, USA). A p-value of less than 0.05 was considered statistically significant.
Go to :
RESULTS
Demographic characteristics
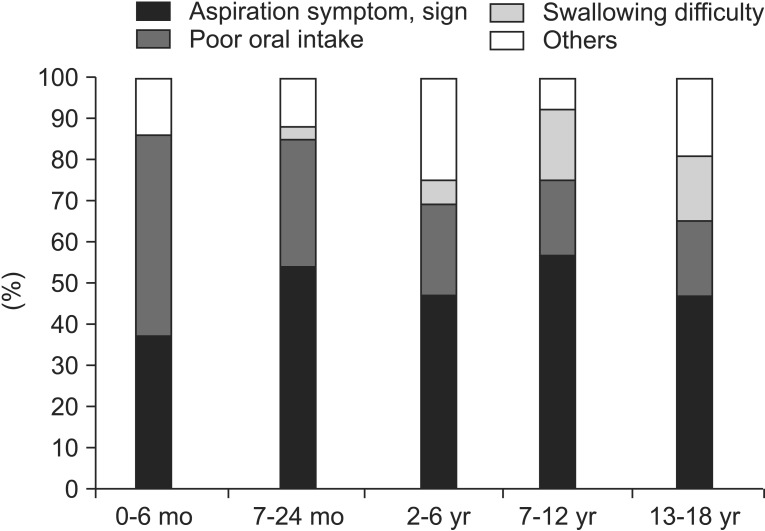
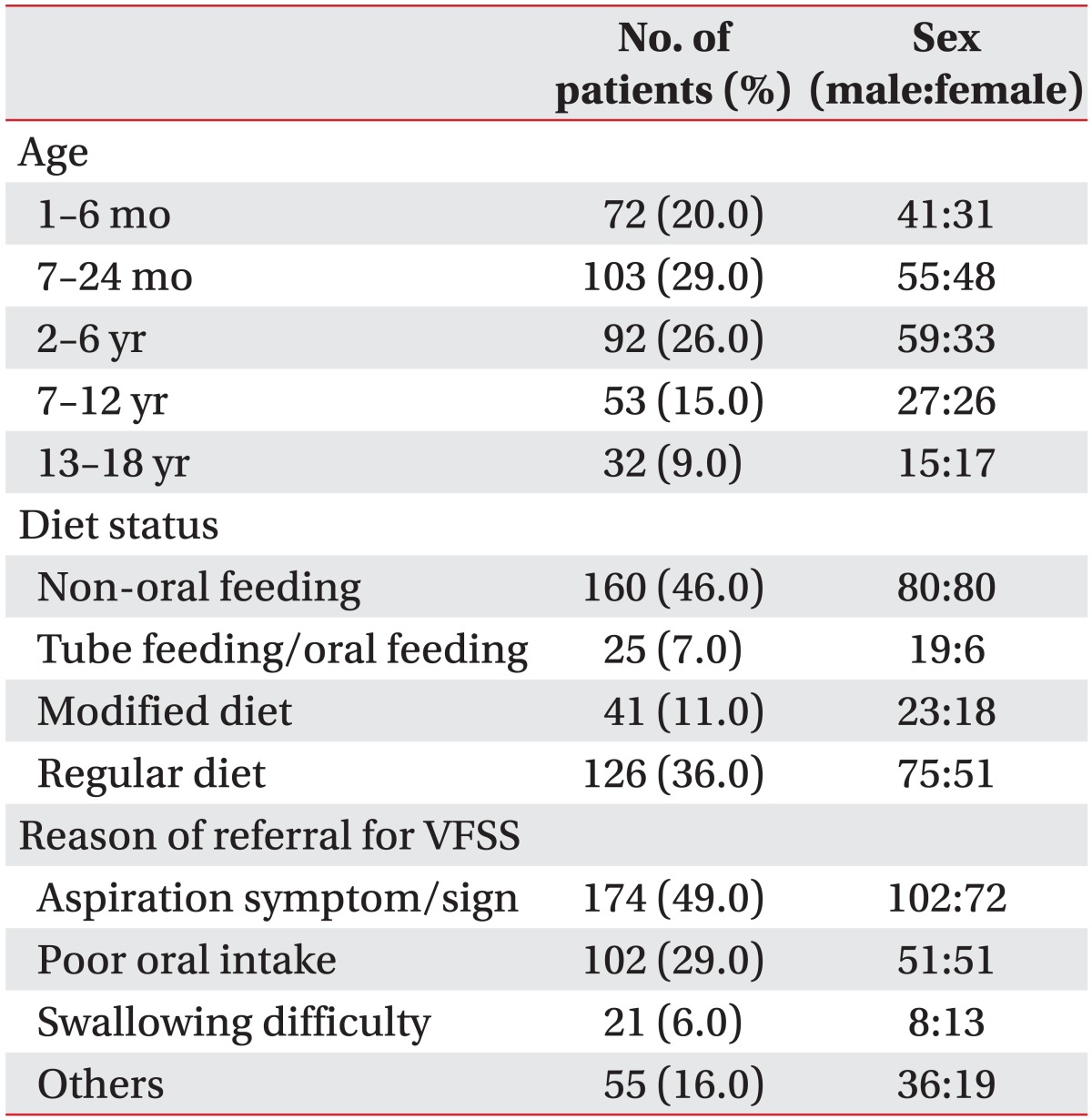
About half of the subjects (n=175, 49%) who underwent VFSS were younger than 24 months. Aspiration symptoms or signs (174/352, 49.4%) were the major cause of referral for VFSS in most age groups except for those younger than 6 months. Almost half of the subjects (35/72, 48.6%) younger than 6 months had poor oral intake. In groups with age over 7 years, swallowing difficulties, such as odynophagia and the sensation of food stuck in the throat, formed a certain percentage (17% and 13%, respectively) (Fig. 1). At the time of the study, 160 subjects (46%) were dependent solely on non-oral feeding methods, including nasogastric and oroesophageal tubes, gastrostomy and jejunostomy tubes, and total parenteral nutrition (Table 1). Among subjects who were on regular diets at the time of the study, aspiration symptoms (60%) were the most common cause of referral for VFSS.
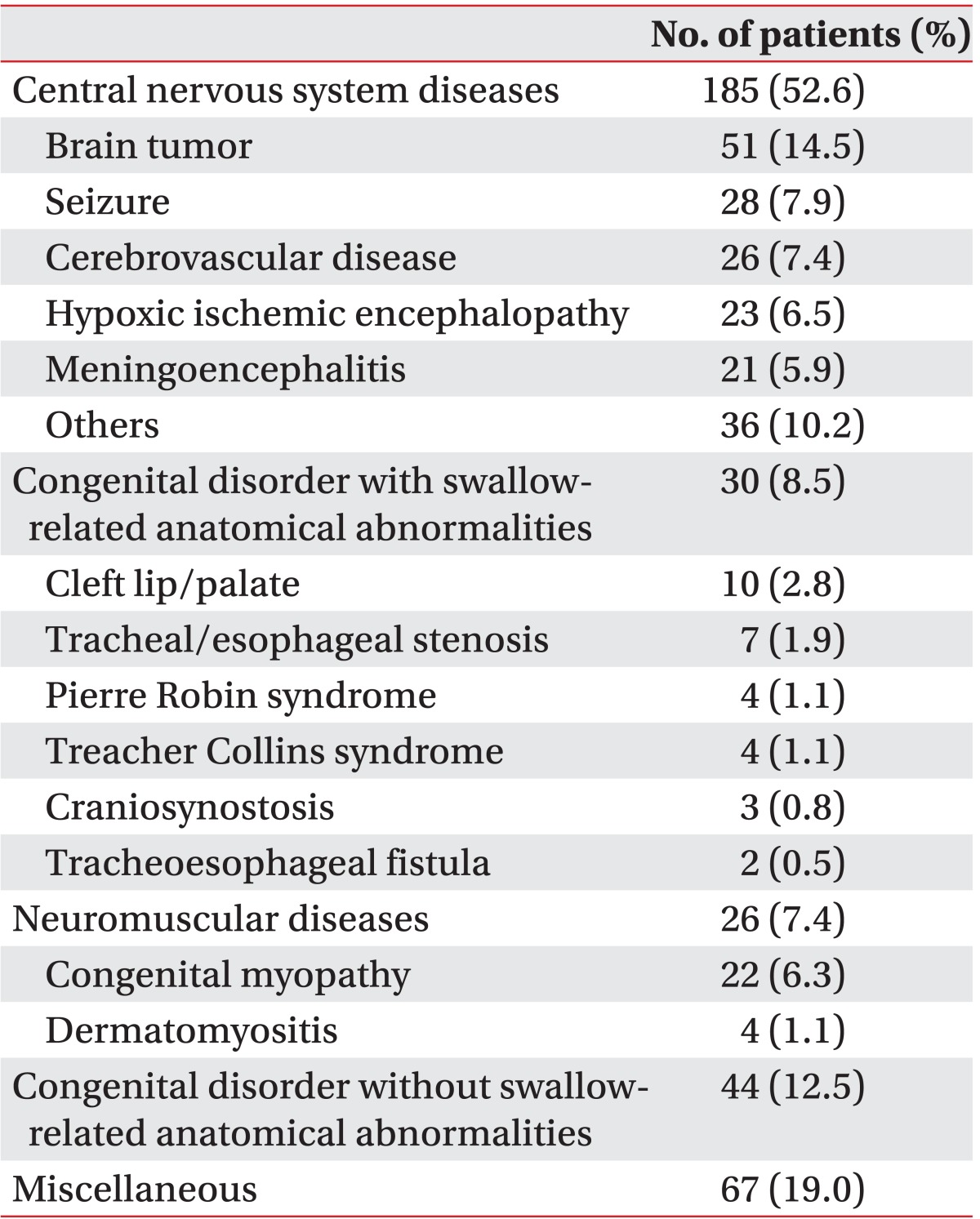
Sixty-two patients (18%) were born prematurely at less than 37 weeks' gestational age, including 33 patients (53%) who were born less than 34 weeks of gestation. The most prevalent underlying medical condition of dysphagia was central nervous system (CNS) disease (53%). The proportion of CNS disease increased from 29% to 81% as the age of subjects increased. In subjects younger than 6 months old, congenital disorder with swallow-related anatomical abnormalities and neuromuscular disease formed a certain percentage (15.3%) of underlying conditions. In the age group between 7 and 24 months, congenital disease without swallow-related anatomical abnormalities was the second leading cause of dysphagia (23%) (Fig. 2).
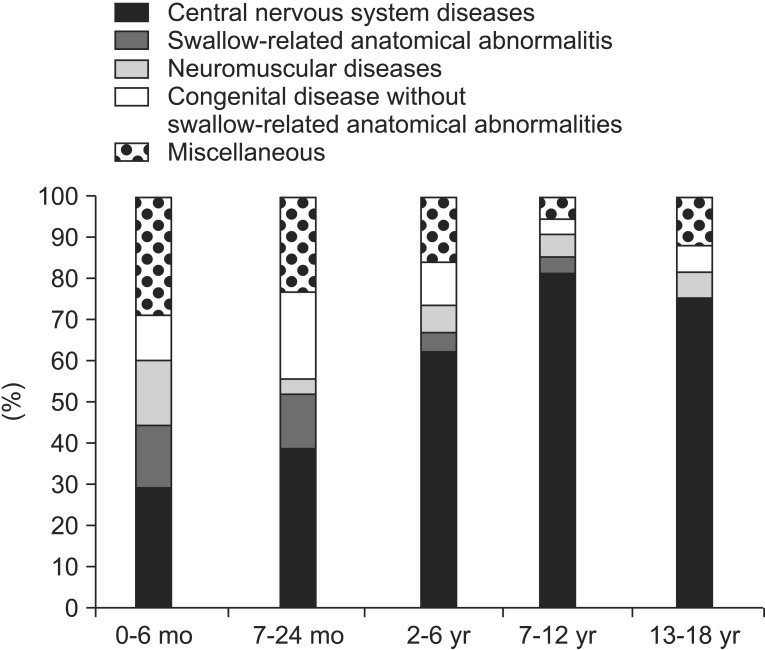 | Fig. 2Proportion of underlying medical conditions in specific age groups. Central nervous system disease was the most common cause of dysphagia in children with an increased tendency in groups of older children. Among children younger than 6 months of age, congenital disorder with swallow-related anatomical abnormalities (11/72, 15.3%) and neuromuscular disease (11/72, 15.3%) formed a considerable portion of the underlying conditions.
|
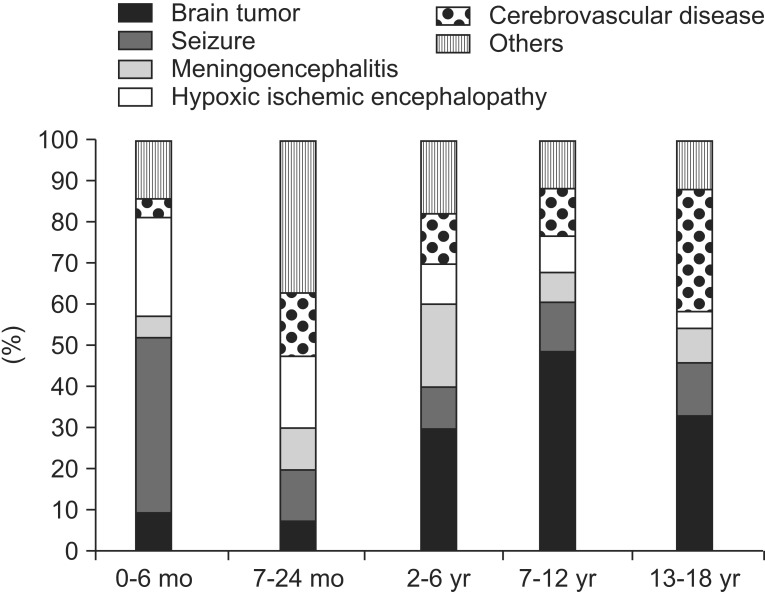
Brain tumor was found in 51 of 185 subjects (28%) with CNS disorder. The percentage showed a tendency of increase from 10% to 49% as the subjects reached school age. Distinctively, seizures (43%) were the first major cause of dysphagia in subjects younger than 6 months (Fig. 3). The subsets of underlying medical conditions predisposing to dysphagia are summarized in Table 2.
Clinical characteristics related to penetration or aspiration
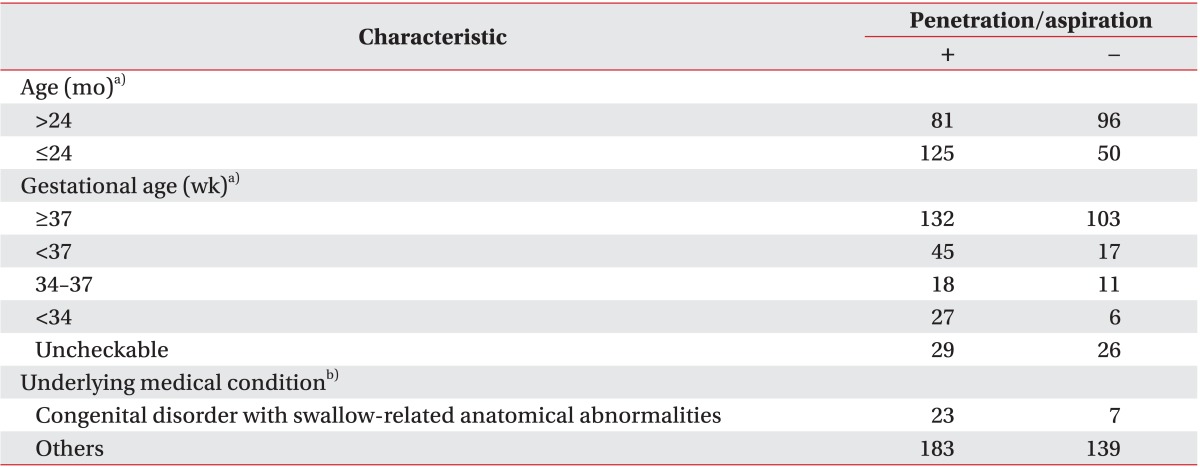
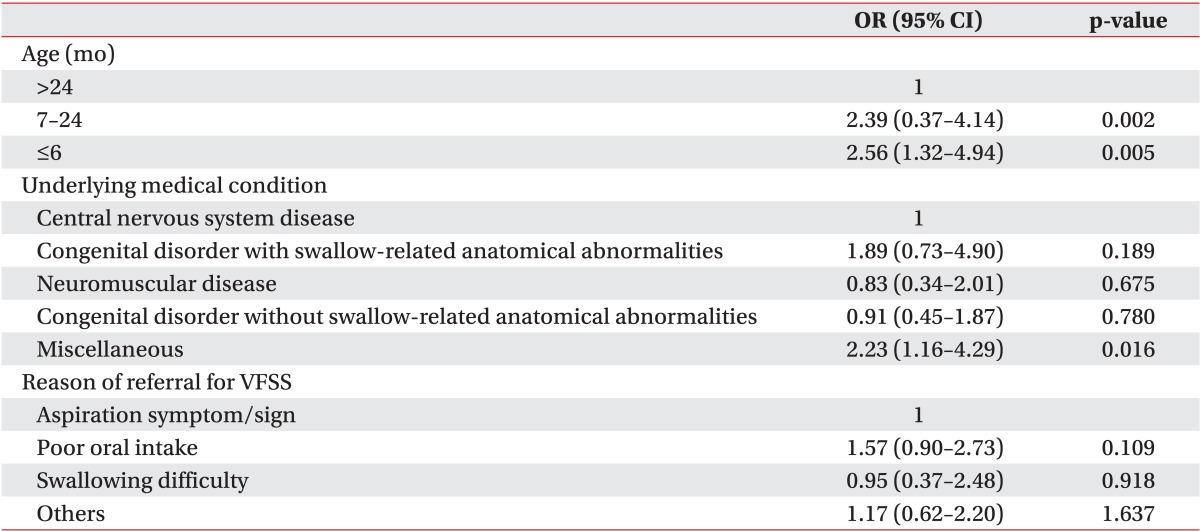
A total of 206 of 352 patients (58.5%) experienced penetration or aspiration during VFSS (Table 3). Three factors were significantly (p<0.05) associated with penetration or aspiration in chi-square test. Age groups under 24 months of age were more likely to show penetration or aspiration (p<0.001). The groups of subjects born prematurely were more likely to show penetration or aspiration (p=0.019). Of subjects born prematurely, children less than 34 weeks of gestational age were significantly more likely to experience penetration or aspiration (p=0.026) through subgroup analysis. Throughout various underlying medical conditions, patients with congenital disorder and swallow-related anatomical abnormalities had a higher percentage of penetration or aspiration with marginal statistical significance (p=0.074) (Table 4). Multiple logistic regression analysis showed that age younger than 24 months and miscellaneous underlying medical conditions were independent factors associated with penetration or aspiration findings in VFSS (Table 5).

Go to :
DISCUSSION
The objective of the present study was to identify the demographic characteristics and clinical factors related to penetration or aspiration in children with dysphagia who underwent VFSS. About 50% of the children in this study were less than 24 months of age, which corresponded well with the results of an earlier study by Rommel et al. [6]. The reason for the percentage of children younger than 24 months of age might be the essentiality of feeding for survival in those age groups. In this study, penetration or aspiration was observed in more than 70% of subjects with dysphagia who were younger than 24 months of age, which was similar to the penetration or aspiration rate of 74.8% in infants with swallowing difficulty reported by Uhm et al. [15]. However, Lee et al. [16] and Mercado-Deane et al. [17] reported aspiration rates in infants at 17% and 52%, respectively, which were lower than the rate in the present study. The discrepancy could be due to the difference in study populations. This study included subjects from a tertiary hospital where there are a large number of critical patients with serious underlying medical conditions.
In addition, premature groups were more likely to show penetration or aspiration in univariate analysis, especially those born earlier than 34 weeks' gestational age. This fits well with the fact that coordination of sucking, swallowing, and breathing is established at 34 weeks of gestation [18]. However, prematurity was not significantly associated with aspiration in multivariate analysis. Of the 62 patients with prematurity history, 44 (71%) were younger than 2 years, 25 (40%) had CNS disease, 22 (35%) had miscellaneous disease, 12 (19%) had congenital disease, 3 (5%) had neuromuscular diseases. Ninety-two percent of premature patients performed VFSS at the corrected age of 4 months and older, indicating that most patients had dysphagia for a perceptible time. There is a high probability that aspiration of prematurity was influenced by other factors, including underlying medical conditions and age.
The results of this study demonstrate that CNS disease, especially brain tumor, is the most common underlying medical condition in children with dysphagia. Lefton-Greif [13] and Love et al. [19] reported that cerebral palsy was the most frequent neurologic condition associated with dysphagia in children. Rommel et al. [6] reported gastrointestinal problem was the most frequent medical diagnosis of children presenting feeding problem in a tertiary care center. The difference between our result and results by others could be explained by high ratio of critical patients in our hospital.
In multiple logistic regression analysis, patients with miscellaneous underlying medical conditions were more likely to show penetration or aspiration in VFSS. Miscellaneous conditions included various heart diseases (n=9, 3%), gastroesophageal reflux disease (GERD) (n=16, 5%), post-intensive care condition (n=3, 1%), and unknown causes. Infants with congenital heart disease are at risk of potential dysphagia, secondary to postoperative vocal cord dysfunction [20]. Patients with GERD often show aspiration pneumonia, masquerading oropharyngeal dysphagia. GERD can also occur in conjunction with laryngeal dysfunction or swallowing incoordination [17]. Patients with prolonged intubation are at increased risk of dysphagia mostly reported in adults [21]. Endotracheal tube can cause remodeling of palate due to pressure of the tube on the hard and soft palate [22]. Despite several tests, 16 subjects failed to reveal the exact cause of dysphagia. This group needed continuous consultation and periodic follow-up of changes in dysphagia. Patients with dysphagia of unknown cause need further research.
For all age groups except for infants younger than 6 months, aspiration symptoms or signs were the major causes of referral for VFSS. In patients younger than 6 months, poor oral intake was the primary cause of referral for VFSS. This finding correlated well with the results of Newman et al. [5] who reported that infants were less likely to show aspiration symptoms such as cough due to anatomical structures. However, our study showed higher penetration or aspiration rates during VFSS in younger age groups. This suggests that younger children without aspiration symptoms or signs can have silent penetration or aspiration which can be revealed by VFSS. The existence of silent penetration or aspiration displays the usefulness of VFSS in children with underlying medical conditions with ambiguous symptoms of dysphagia [8]. However, VFSS findings should be interpreted and integrated with other information, including feeding history, underlying medical conditions, and nutritional status. A physical examination including posture and position of feeding, respiratory pattern, alertness, response to sensory stimulation, self-regulation ability, oral structure, and growth should also be conducted. In addition, symptoms, such as vomiting, coughing, choking, drooling, wet voice, and feeding observation, must be included. Children are very sensitive to taste, texture, and temperature of food [23]. Therefore, using subject's usual meal for VFSS can change the result of the study, especially in those with poor oral intake.
There were several limitations to this study. First, this was a retrospective study. Second, the study was a single-center study. Therefore, referral bias might be an inherent consequence. In addition, a high ratio of preterm infants with variable underlying medical conditions was used in this study.
In conclusion, the results of this study showed that penetration or aspiration was more often observed (approximately 70%) in children younger than 24 months of age. The penetration or aspiration rate was higher in those born prematurely at less than 34 weeks of gestation. Underlying medical conditions causing dysphagia differed by age group. This study revealed that younger children born prematurely are at higher risk to develop feeding disorders. Therefore, performing VFSS is beneficial for these children. The findings from this study will improve our understanding on the usefulness of VFSS in children with dysphagia of unknown etiology, particularly for those younger than 24 months with a history of preterm birth.
Go to :
 XML Download
XML Download