

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Holmes' tremor was first described in 1904 [1]; it is characterized as both a rest and intentional tremor that is often non-rhythmical [2]. The tremor is of low-frequency flexion-extension oscillation at rest, mostly below 4.5 Hz, exacerbated by posture and action, and generally unilateral [1,2,3]. There is variable delay (approximately 4 weeks to 2 years) between the lesion and the first occurrence of tremor [1,2,3]. Treatment includes oral drugs, such as levodopa, dopamine agonists, propranolol, clonazepam, and levetiracetam; thalamic surgery; and deep brain stimulation. However, such treatments have been described only by isolated case reports, thus treatment remains challenging.
We report a patient with Holmes' tremor secondary to pontine hemorrhage previously diagnosed with schizophrenia and failed usual medical treatment. The patient responded markedly well to ultrasonography-guided botulinum toxin type A (BoNT-A) injection.
Go to : 
CASE REPORT
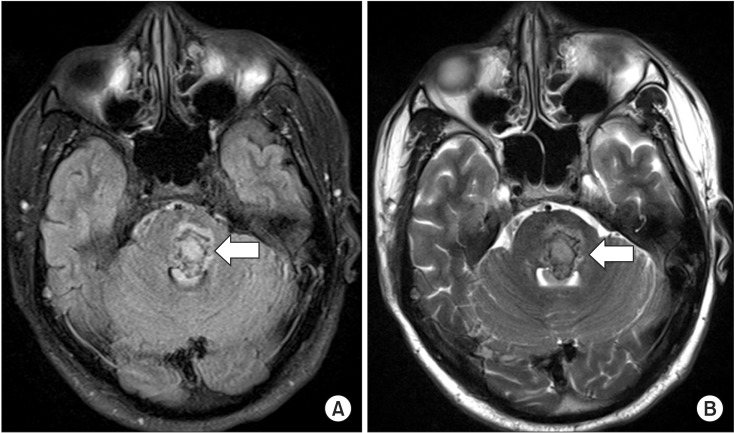
A 29-year-old Asian male patient with a 4-month history of 1.6-Hz postural and rest tremor of the right hand, consistent with Holmes' tremor, visited our department. He had been quadriplegic secondary to left pontine hemorrhage for 6 months (Fig. 1). His medical history was notable for a 6-year history of paranoid-type schizophrenia and psychiatric treatment with several typical and atypical antipsychotic agents. Four months ago, a 1.4- to 2-Hz tremor developed in his right hand and gradually spread to the wrist and elbow, characterized by irregular flexion-extension oscillation, distal prominence, presence at rest, and increase with posture. It worsened his right upper extremity function and his gait, leading to limitation of activities of daily living. In family history, his mother had schizophrenia but there was no history of movement disorders, including tremors and other neurologic illnesses.
Current medications were olanzapine (10 mg daily), amisulpride (100 mg daily), and lorazepam (0.5 mg daily) as antipsychotic agents for the past 6 years, and levetiracetam (1,000 mg daily) as seizure prophylaxis for the past 6 months. For tremor relief, he received clonazepam (4 mg daily) for 3 months and levodopa (500 mg daily) for 2 months. Although these medications mildly improved the tremor, visual hallucinations became more vivid and frequent.
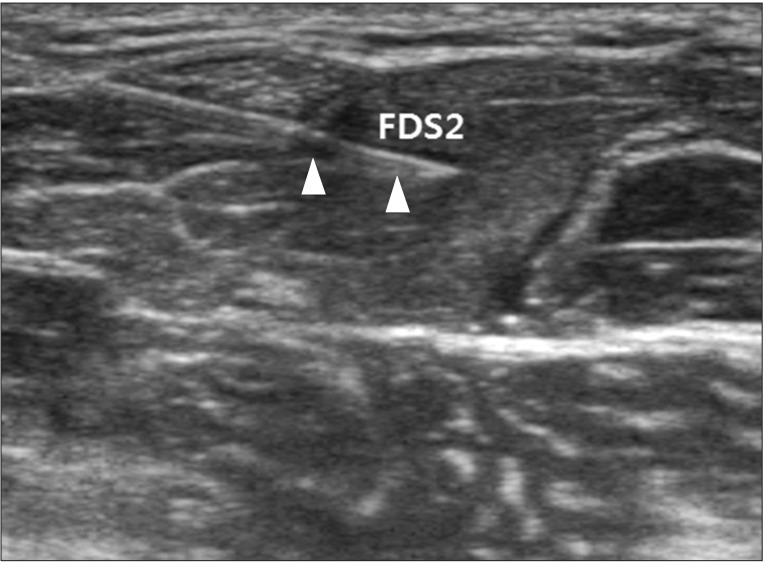
Therefore, we administered 100 units (U) of BoNT-A (Botox; Allergan, Irvine, CA, USA) while decreasing the dosages of the medications for tremor. Injection was performed by an expert physiatrist using ultrasonography (ACCUVIX XG; Medison, Seoul, Korea) interfaced with a 5-13 MHz linear array transducer and electrical stimulation (Stimuplex; B. Braun Melsungen AG, Melsungen, Germany) guidance in the right side of the flexor digitorum superficialis of the second, third, and fourth digits (20 U each), and in the extensor pollicis longus (40 U) muscles (Fig. 2). Those muscles were selected because they showed the most vivid contraction on real-time ultrasonography during rest and during provoked state by clenching his left fist and elevating his lower extremities. During the first few days after infiltration, improvement of symptoms, mainly tremor on extension of the first, second, and third fingers, was observed. Rest tremors showed marked improvement, and postural and intentional tremors also improved, although to a lesser extent.
The frequency of tremor was measured retrospectively with video recording of ultrasonography; it decreased from 1.4-2 Hz to 0-0.5 Hz. In terms of activities of daily living, improvements in eating and dressing were observed. After 1 month of injections, he could perform small object manipulation, which was not possible at admission. The maximum benefit became evident approximately 2 weeks later and lasted for 2 months. Then, rest tremor reoccurred progressively. After 3 months of BoNT-A injections, the frequency of tremor decreased from 1.4-2 Hz to 1-1.4 Hz, and the duration at provoked state shortened from 3-5 to 2-3 minutes. Injection of 100 U of BoNT-A was repeated in the same muscles using ultrasonography guidance.
Go to :
DISCUSSION
Holmes' tremor is a rare late effect of lesions that occur in the brainstem, cerebellum, or thalamus owing to various nigrostriatal and cerebellothalamic pathway-damaging insults, including cerebral ischemia, hemorrhage, trauma, or neoplasm [2,4]. In most cases, medical therapy shows poor response, although levetiracetam, levodopa, clonazepam, ventralis intermedius nucleus thalamotomy, and deep brain stimulation have been reported to be effective in several case reports [3,5,6]. Alternative medical or surgical approaches for Holmes' tremor are not yet well established because of the absence of controlled studies. Unlike drug-induced tremor, the tremor in this case was nonrhythmical, with low-frequency (mostly 1.4-2 Hz) flexion-extension oscillation at rest [7]. Despite using the same antipsychotics for 6 years, no movement complaints, such as tremor, were ever reported. Tremor only occurred 2 months after pontine hemorrhage.
Recently, BoNT-A was recommended by 2 class II studies as a treatment option for essential hand tremor that has failed with other pharmacologic treatments [8]. In this case, BoNT-A injections improved the rest tremor considerably and the postural and intentional tremors mildly in a patient in whom long-term multiple pharmacological treatments had been unsuccessful. In this patient, especially because of his schizophrenia, we could not adequately increase the dose of medication and had to use a dopamine antagonist at the same time. Therefore, BoNT-A could have been more beneficial, considering the localized effect.
Ultrasonography has proved its validity and reliability as a diagnostic imaging tool for muscles and nerves [9]. We performed ultrasonography-guided BoNT injection in the upper limb muscles, which permitted accurate muscle selection. This procedure has been suggested as a standard technique for deep-seated and small muscles [10]. In addition, ultrasonography allowed us to compare tremor using frequency of muscle contraction as an objective indicator before and after treatment to evaluate progression. Frequency was obtained by counting each muscle contraction with the use of retrospective video recording analysis. To our knowledge, this is the first case of tremor evaluated using ultrasonography. Clinical numeric rating scales or ataxia scales also can be used for tremor evaluation, but they tend to be underestimated in subjects who have paralysis, spasticity, or decreased motor power. Although ultrasonography does not evaluate neurophysiological properties, only anatomic aspects, it has the advantages of noninvasiveness and easy accessibility. It also enables real-time inspection during injection and video recording.
Despite the transient effect of BoNT-A, it was the treatment of choice in this case due to the prescription limitations for the patient because of his schizophrenia. He also did not want an invasive treatment, such as surgery. The results in our case support the potential of BoNT-A injection in patients with Holmes' tremor before applying more invasive therapies. In addition, ultrasonography can be a useful instrument for the objective evaluation and treatment of tremor.
Go to :
 XML Download
XML Download