

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hemodialysis is one of the most important and classic treatments for chronic renal failure. There should be at least 200 mL blood in circulation between the patient and hemodialysis machine for eliminating waste, and hence it is important to secure access to a large vessel for hemodialysis [1,2]. An external shunt had been used for securing access to a large vessel in the past, but it had many problems, such as thrombosis, infection, etc. [3,4]. Therefore, Brescia et al. [4] introduced a new method for vascular access, arteriovenous fistula (AVF), and decreased the complications of hemodialysis. AVF is considered as the gold standard for safe and effective vascular access during hemodialysis treatment [2,5].
However, there are still some problems with AVF surgery. The common complications of AVF surgery are as follows: AVF dysfunction, venous thrombosis, edema or ischemia in the fistula-created limb, atherosclerosis, and neuropathy after surgery. Technical difficulty of anastomosis, inappropriate position of the artery or vein, sclerosis of the proximal vein, calcification in the artery and anastomotic failure, and hypotension due to a hypovolemic state could also occur following AVF surgery [6,7].
For avoiding these complications, appropriate vascular maturation time is needed after surgery. In previous studies, different maturation times ranging from 4 to 8 weeks were suggested. However, in a clinical setting, we usually wait for 4 weeks [8]. The patients are asked to perform hand exercises during this period to encourage fistula maturation. Usually, hand-squeezing exercise with a soft ball or a rubber ring is performed [5], and the exercise protocol is according to the Kidney Disease Outcomes Quality Initiative guidelines. It suggests that the patients should perform hand squeezing exercise 2 days after the AVF surgery when edema of the limb has decreased. If there are any unusual findings at the surgical site, such as sustained edema, redness, tenderness, discharge or abscess formation, the patient must stop the exercise and the surgical site should be checked by the surgeon [9,10].
There have been many studies demonstrating the beneficial effects of hand exercise on maturation of the blood vessels and reduction in the complications after AVF surgery. Hand exercise was proved to be effective in increasing the diameter of the artery and vein around the AVF, and it improved the capacity for vasodilatation and maturation of the fistula [5,11,12]. The hand exercise could consequently decrease the mortality rate after AVF surgery [13]. However, no research has been performed for determining which type of hand exercise is more effective for facilitating the maturation of the vessels and for improving the functioning of the fistula.
Although hand exercises increase the blood flow in the fistula and decrease the complications of surgery [5,11,12,13], it does not indicate a direct improvement of hand strength (e.g., grip strength, pinch strength, or forearm muscle strength). It is important to assess the muscle power because it could represent the general body strength in patients, and it can also be used as a parameter for predicting the success of rehabilitation exercise [14,15]. To the best of the authors' knowledge, no study has assessed which type of hand exercise is more beneficial for improving the hand strength after AVF surgery.
Therefore, the aims of this study are to assess the following. 1) Can the 2 types of hand-squeezing exercises significantly improve cephalic vein maturation after AVF surgery? 2) Can the 2 types of hand-squeezing exercises significantly increase the grip strength, pinch strength, and forearm circumference (representing the forearm muscle strength)? 3) Is there any significant difference between the two exercises in improving the muscle strength and vascular maturation?
Go to : 
MATERIALS AND METHODS
Subjects
Eighteen subjects who were diagnosed with chronic kidney disease (CKD) and had undergone AVF surgery for hemodialysis at Hanyang University Guri Hospital were recruited into this study. The purpose of the study was explained to the subjects, and the volunteers understood that the study would be performed in accordance to the Declaration of Helsinki. They signed the informed consent form approved by the Institutional Review Board of the Hanyang University Hospital for the Protection of Human Subjects.
If patients had injury, history of surgery, or limitation of motion (LOM) in the fistula-created limb, they were excluded from the study. We performed electromyography or magnetic resonance imaging of the operated limb if the patient complained of pain around the arm, and patients with peripheral neuropathy or radiculopathy were also excluded. The inclusion of patients with rheumatic disorders, myopathy, and any type of arthritis that could affect the study results was also limited.
The total number of subjects was 18 (6 males and 12 females), and they were diagnosed with CKD by a nephrologist at the Hanyang University Guri Hospital. Each patient had undergone an AVF surgery in the upper limb for hemodialysis, which was performed by one experienced thoracic surgeon in the same hospital. The patients were randomly allocated into two groups, and the first group (10 subjects) used handgrip for the hand-squeezing exercise, and the second group (8 subjects) used soft ball.
The mean ages of patients in the groups using handgrip and soft ball were 64.3±3.1 years and 63.5±2.8 years, respectively. The mean body weights were 60.5±4.1 kg and 61.3±3.4 kg, respectively; and the mean heights were 163.7±5.4 cm and 162.8±4.7 cm, respectively. There was no significant difference with respect to the age, weight, and height between the two groups (Table 1).
One out of these 18 subjects had CKD as a complication of contrast medium, 3 subjects had CKD due to hypertension, 5 subjects had CKD due to unknown reasons, and 9 subjects had CKD due to diabetes mellitus.
Exercise protocol
The subjects who trained with handgrip used GD Grip (GD Co., Incheon, Korea) (Fig. 1) and the other subjects used Soft Ball (MCS Co., Xiamen, China) (Fig. 2).

The subjects who used GD Grip set their handgrip resistance at 10 repetition maximum (RM), and performed 10 squeezes for 1 set. They performed 3 sets of 10 squeezes each at a 1-minute interval. Three sets of exercises were performed 2 times in the morning and 2 times in the afternoon. Resistance of GD Grip was reset to 10 RM every week when the subjects visited our out-patient department.
The subjects who used Soft Ball squeezed the ball 10 times for 1 set, and performed 3 sets of 10 squeezes each at an 1-minute rest interval. Three sets of exercises were performed twice in the morning and twice in the afternoon.
All of the subjects were monitored for any signs of infection, abscess formation, inflammation, dehiscence, pain or tenderness causing LOM in the operated limb during 24 hours after the AVF surgery. If these abnormal signs were not detected during 24 hours, they immediately started the hand-squeezing exercise. Patients in both groups performed the exercise for 4 weeks.
The subjects were instructed not to undergo any other physical therapy or perform a different hand exercise during these 4 weeks. They were instructed to perform only the activities of daily living, and not to perform any strenuous activities.
Measurement of hand strength and forearm circumference
We used Jamar hand dynamometer, and Jamar hydraulic pinch gauge (Sammons Preston Rolyan, IL, USA) for measuring the hand grip strength and pinch strength (Figs. 3, 4) [16].
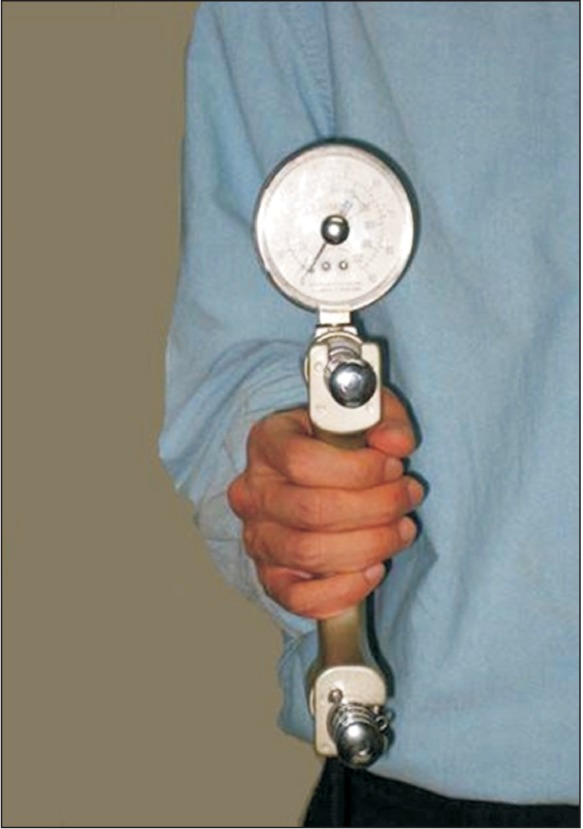
For measuring the grip strength, the subjects were asked to sit on a chair with their hip joint flexed at 90°, and shoulder joint in a neutral position. The elbow was fixed at 90° flexion, forearm in a neutral position, and wrist at 0° to 15° radial deviation (Fig. 3). The test was performed twice, and the higher value between the two measurements was selected. The subjects were allowed a rest time of more than 5 minutes after the first measurement to avoid examiner bias and to decrease physical stress.
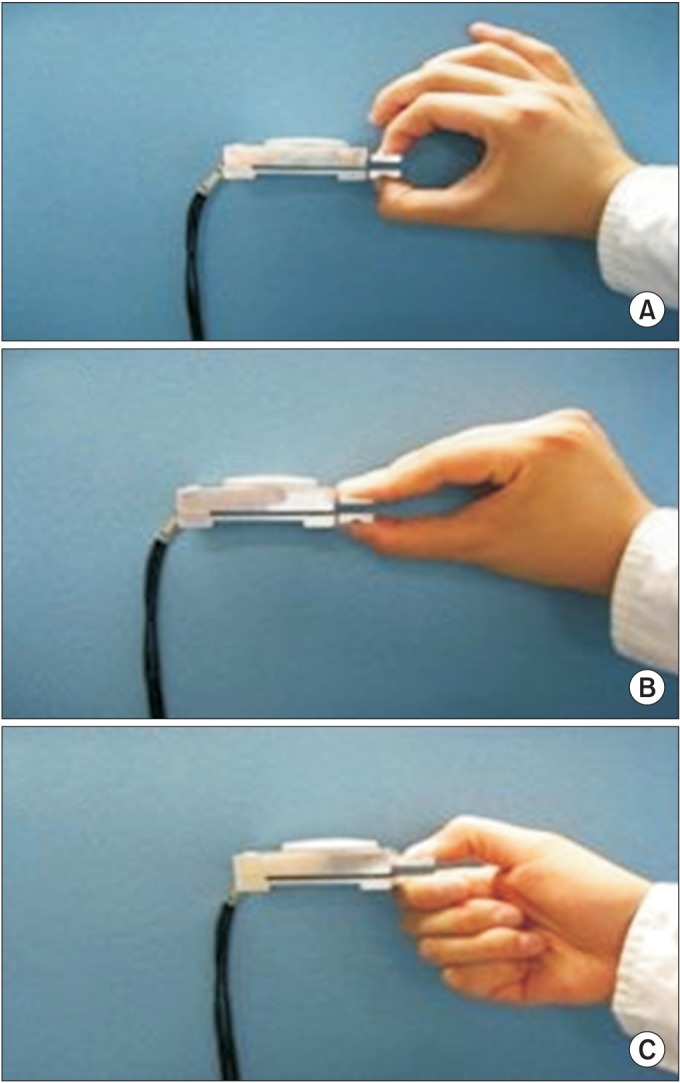
Pinch strength was measured during 3 types of pinchtip pinch, palmar pinch, and lateral pinch (Fig. 4) [17,18,19,20,21,22]. In tip pinch, the tip of the index finger and thumb hold the objects (Fig. 4A). It can be used as a parameter for indicating direct strength of the two fingers. In palmar pinch, the thumb, index finger, and middle finger hold the objects (Fig. 4B). In lateral pinch, the thumb and the lateral side of index finger come into contact (Fig. 4C). The levers of dynamometer and pinch gauge were held at the same width during each test, and therefore, the subject could start griping or pinching with the same force by using the same muscles [23].
The examiner helped the subjects to maintain their forearm and hand steady and parallel to the ground by holding the bottom of the dynamometer and pinch gauge. The measurement unit was kilogram (kg).
For measuring the circumference of the forearm, the subjects were seated on a chair with their forearm supinated, and the elbow flexed at 90°. Circumference of the forearm was measured 2 cm distal to the cubital fossa.
The grip strength, pinch strength, and circumference of the forearm were measured by the same examiner before beginning the hand-squeezing exercise and 4 weeks after the exercise.
Examination of the cephalic vein
The cephalic vein in the operated arm was examined by an experienced technician with ultrasonography. A single technician performed ultrasonography during the whole study, and he was not aware of the exercise group to which the subjects were allocated. Ultrasonography of the cephalic vein was performed before beginning the exercise and after completing the 4-week training. The technician examined the vein from the AVF site to the proximal area till he could identify the vein on the image, and the last detectable area was usually the shoulder joint. The largest and shortest diameter, blood flow volume, and blood flow velocity were measured where the area of the vein was the smallest [5,11]. We calculated the size of the vein based on the mean value of the largest and shortest diameter.
Statistics
SPSS ver. 18.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The p-values less than 0.05 were considered statistically significant. Wilcoxon signed-rank test was used for comparing the grip strength, pinch strength, and ultrasound measurements between pre- and post-exercise in each group.
We used Mann-Whitney U test to compare between the GD Grip group and Soft Ball group. For statistical analysis between the groups, percentage increase was used. Percentage increase was calculated based on the difference between the pre- and post-exercise values, which was divided by pre-exercise values and multiplied by 100.

Go to :
RESULTS
Comparison of pre- and post-exercise changes in each group
GD Grip group: changes in the grip strength, pinch strength, forearm circumference, and vascular measurements
In the GD Grip group, before the exercise, pinch strength was 2.4±0.9 kg in the tip pinch, 3.0±1.2 kg in the palmar pinch, and 3.4±1.2 kg in the lateral pinch. The grip strength was 10.8±5.3 kg and forearm circumference was 22.0±0.8 cm. The size of the cephalic vein was 5.5±0.7 mm, blood flow velocity was 27.0±30.8 cm/sec, and blood flow volume was 299.3±330.9 mL/min.
After the 4-week exercise program, strength of the tip pinch was increased to 3.2±1.0 kg, that of the palmar pinch was increased to 3.8±1.1 kg, and that of the lateral pinch was increased to 4.5±1.1 kg. The grip strength was elevated to 16.7±6.1 kg and the forearm circumference was increased to 22.7±0.9 cm.
The pinch and grip strength and forearm circumference were significantly increased after the 4-week exercise (p<0.05) (Table 2).
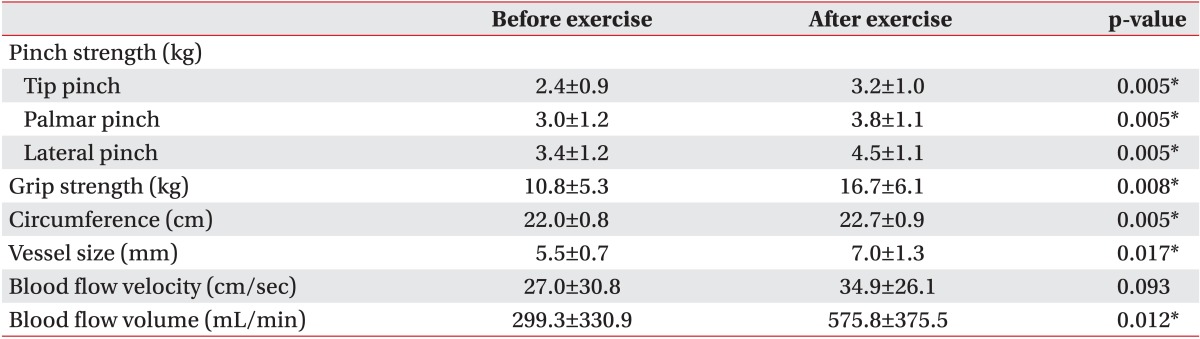
Two out of the 10 subjects refused to undergo ultrasound examination because of difficulty in visiting the hospital and busy work schedule. The size of the cephalic vein was increased to 7.0±1.3 mm, blood flow velocity was increased to 34.9±26.1 cm/sec, and blood flow volume was elevated to 575.8±375.5 mL/min. Only the cephalic vein size and blood flow volume showed a significant increase after the exercise (p<0.05) (Table 2).
Soft Ball group: changes in the grip strength, pinch strength, forearm circumference, and vascular measurements
In the Soft Ball group, before the exercise, pinch strength was 2.4±0.6 kg in the tip pinch, 3.7±1.0 kg in the palmar pinch, 4.5±1.3 kg in the lateral pinch. The grip strength was 13.0±4.8 kg and forearm circumference was 23.2±1.9 cm. The size of the cephalic vein was 5.6±1.3 mm, blood flow velocity was 20.3±18.9 cm/sec, and blood flow volume was 241.7±224.6 mL/min.
After 4 weeks, strength of the tip pinch was increased to 2.6±0.6 kg, that of the palmar pinch was increased to 3.9±0.8 kg, and that of the lateral pinch was increased to 5.1±1.3 kg. Grip strength was increased to 16.6±5.3 kg and the forearm circumference was increased to 23.6±2.1 cm. Only the strength of tip and lateral pinch, and the forearm circumference were significantly increased after the exercise with Soft Ball (Table 3).
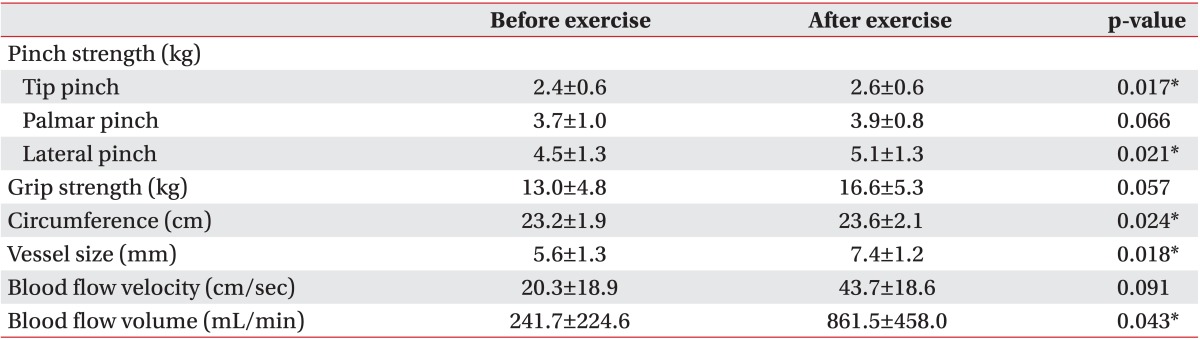
One out the 8 patients refused to undergo ultrasound imaging because of busy work schedule. A total of 7 subjects underwent ultrasound examination, and the mean size of the cephalic vein was increased to 7.4±1.2 mm. Blood flow velocity was increased to 43.7±18.6 cm/sec and blood flow volume was elevated to 861.5±458.0 mL/min. The cephalic vein size and blood flow volume demonstrated a significant increase (p<0.05) (Table 3).
Comparison between the two groups: percentage increase after the 4-week exercise program
We calculated the percentage increase in the pinch strength, grip strength, forearm circumference, and vascular measurements for comparing between the GD Grip group and Soft Ball group (Table 4).
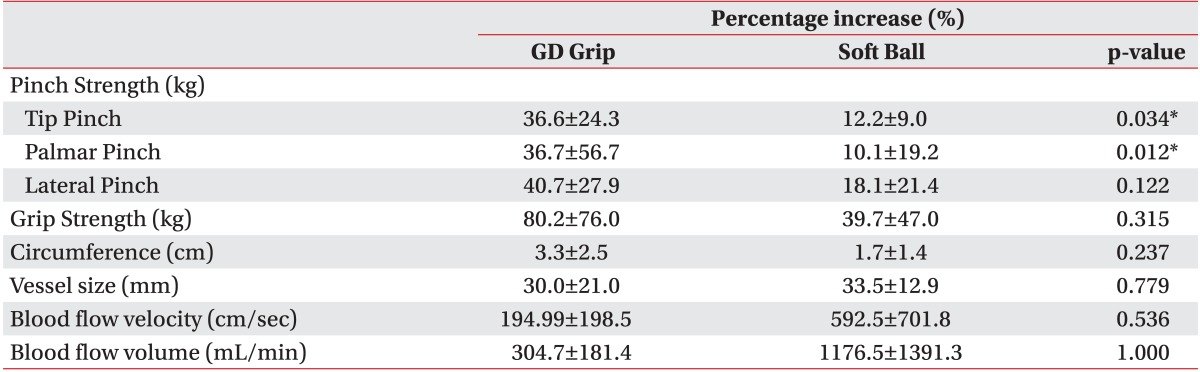
GD Grip group showed a percentage increase of 36.6% in the tip pinch strength, 36.7% in the palmar pinch strength, and 40.7% in the lateral pinch strength. The percentage increase in grip strength was 80.2%, and that in the forearm circumference was 3.3% after the 4-week exercise program. The percentage increase in the size of the cephalic vein was 30.0%, that in the blood flow velocity was 194.9%, and that in the blood flow volume was 304.7%.
Soft Ball group demonstrated a percentage increase of 12.2% in the tip pinch strength, 10.1% in the palmar pinch strength, and 18.1% in the lateral pinch strength. The percentage increase in grip strength was 39.7%, and that in the forearm circumference was 1.7%. The percentage increase in the size of the cephalic vein was 33.5%, that in the blood flow velocity was 592.5%, and that in the blood flow volume was 1,176.5%.
Comparison of percentage increase between the two groups did not show any significant difference in the vascular measurements, grip strength, and lateral pinch strength, but it showed a significant difference only in the tip pinch and palmar pinch strength (p<0.05). Therefore, it was proved that exercise with GD Grip significantly improved the strength of the tip and palmar pinch compared to exercise with Soft Ball (Table 4).
Go to :
DISCUSSION
Exercise with Soft Ball
Exercise with Soft Ball significantly increased the strength of the tip pinch and lateral pinch. We could assume that hand-squeezing exercise with Soft Ball improved the power of fingers, especially the thumb and the index finger. However, it failed to increase the strength of palmar pinch and hand grip.
The tip pinch and palmar pinch strength demonstrated different results after the 4-week exercise program. We hypothesized that this significant difference was probably due to activation of different muscles during each pinching method. In the tip pinch, the index finger and the thumb are flexed for picking up the objects. The muscles used during the tip pinch are usually the flexor pollicis longus muscle (FPL), flexor pollicis brevis muscle (FPB), opponens (OP), adductor pollicis muscle (AP), flexor digitorum superficialis muscle (FDS), flexor digitorum profundus muscle (FDP), and lumbrical muscle (LUM) [24,25,26]. However, in the palmar pinch, the objects are picked up with the fingers straight but flexed at the metacarpophalangeal joint (Fig. 4), and the FPB and LUM are usually used. Exercise with Soft Ball significantly improved the strength of tip pinch and lateral pinch, but it failed to improve the strength of palmar pinch. Therefore, we assumed that hand-squeezing exercise with Soft Ball could be more beneficial for exercising the finger muscles, such as FPL, FDS, and FDP, rather than the intrinsic hand muscles, i.e., FPB or LUM.
Although exercise with Soft Ball improved the strength of the index finger and thumb flexors, it could not increase the hand grip strength. We hypothesized that the hand-squeezing exercise with Soft Ball did not cause a statistically significant increase in the grip strength, but it could cause a clinical improvement in the grip strength (p=0.057).
The hand-squeezing exercise with Soft Ball also increased the strength of lateral pinch. This pinching method usually uses adductor pollicis muscle and dorsal interosseous muscle [27]. It would be reasonable to assume that exercise with Soft Ball would also be helpful for exercising these muscles.
The forearm circumference was significantly increased after exercise with Soft Ball. It was a parameter for examining the general strength of the forearm muscles. We could presume that the significant increase in the forearm circumference resulted from the changes caused by the hand-squeezing exercise in the FPL, FDS, and FDP. In a previous study, finger flexing exercise was proved to be beneficial for increasing the muscle volume, and the increase in muscle volume was due to the FDS and FDP [24]. Furthermore, the changes in muscle volume were found at all ages. In not only the young subjects but also in the elderly subjects, an increase in the muscle volume, especially that of the first dorsal interosseous muscle, was observed [28].
The exercise with Soft Ball caused a significant improvement in the size of the cephalic vein and blood flow volume. Our results support the previous findings that resistance hand exercise could significantly increase the vessel diameter and vasodilatation compared to that in the non-exercise group after AVF surgery [5,13]. We considered one more parameter, the blood flow volume, and demonstrated that the blood flow volume was also improved considerably after the exercise.
Exercise with GD Grip
Exercise with GD Grip significantly improved all the 3 types of pinch and grip strength. It was already proved that performing exercise with increased resistance caused more protein synthesis in the muscles and increased the total volume of muscles than training with same resistance [24,28,29] Therefore, applying more resistance during exercise with GD Grip to fit into 10 RM would be more helpful for increasing the strength. The exercise with GD Grip also increased the size of the cephalic vein and blood flow volume.
Comparison between the two exercises
Comparison between the two exercises demonstrated a significant difference only in the tip pinch and palmar pinch strength.
Although both the exercises increased the strength of tip pinch, the exercise with GD Grip was more effective in increasing the tip pinch strength. In other words, both the exercises were beneficial for exercising the FPL, FDS, and FDP, and the beneficial effect was greater after exercise with GD Grip. However, the effect of the two exercises on the lateral pinch strength, hand grip strength, forearm circumference, vessel size, blood flow volume and velocity was not significantly different between the two exercises (Table 4).
Both the exercises could significantly improve the vessel size and blood flow volume. It means that the 2 types of exercises, same resistance-repeat and increased resistance-repeat exercises, had the same effect on vascular maturation. Unless exceptional hand strength is required, for example, training the athletes or sports players during the acute period after surgery, it is not important which type of exercise he or she performs. In contrast, elderly patients or patients with poor compliance have a high possibility of dropping out of the exercise program because of high loading while performing the increased resistance exercise. Therefore, we suggest that the patients should perform steady-state exercise for vascular maturation rather than high loading exercise, and doctors should be aware of the fact that the key to successful AVF formation is not the high loading exercise but steady-state exercise program and patient participation.
Although no significant difference was reported in the lateral pinch strength, hand grip strength, and forearm circumference between the two groups, the mean values of percentage increase were much higher in the GD Grip group than in the Soft Ball group, and the vessel size, blood flow velocity and volume were higher in the Soft Ball group (Table 4). The reason why the results did not reach statistical significance in spite of a big difference in the mean values was presumably a large standard deviation [30]. We could demonstrate that the percentage increase showed fluctuation in each subject. If a subject had shown exceptionally high or low values, he or she should have been excluded from the statistical analysis. However, we could not exclude such subjects from the study population because of the limited number of participants. It is well known that even a nonparametric analysis can produce a statistical error when the sample size is too small [31].
Another possible explanation for why the results failed to reach statistical significance is the short exercise period. In a previous study, the hand strength analyzed with surface electromyography showed maximal increase after at least 8-week training [5,28]. We performed the study with only a 4-week exercise program, and this time period would not be enough for improving the hand strength or vein parameters.
In conclusion, exercise with GD Grip significantly increased the strength of tip pinch and palmar pinch compared with exercise with Soft Ball. However, there was no difference in the vein parameters between the two exercises. Both the exercises could improve the size of the cephalic vein and blood flow volume. It means that resistance exercise can help in vascular maturation regardless of what type of exercise is performed.
Study limitations
There were several limitations to this study. First, a small number of subjects and a short exercise period were the most important limitations. This is probably why the results showed a large standard deviation and caused a possible statistical error. Further evaluation regarding how the activities of daily living would be affected by the improved pinch and grip strength, and vascular maturation is needed.
Go to :
 XML Download
XML Download