

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stroke is one of the most common causes of disability in adults and post-stroke disabilities are usually not cured completely, leaving 50% of stroke patients with sequelae [1]. Available treatments promoting motor function recovery after stroke are functional electrical stimulation (FES), constraint induced movement therapy, traditional physical therapy and occupational therapy, and drug therapy [2,3]. Although traditional physical therapy, occupational therapy, and FES are beneficial for recovery after stroke, complete rehabilitation requires lengthy treatment and effort. In addition, there are limitations to FES because it is based on improving brain capacity through peripheral modulation and drug therapy which may entail side effects [4].
Recently been much research on a non-invasive method to stimulate the brain. The technique of repetitive transcranial magnetic stimulation (rTMS) is beneficial motor functional recovery in hemiplegic patients after stroke by controlling the activation of cerebral cortex [5,6,7,8]. Frequency of rTMS is the most well-known factor that can affect control of cerebral cortex activation. At low frequency (1 Hz), stimulation inhibits the cortex [6,9] and at high frequency (>5 Hz), it excites the cortex [10]. The two ways to improve motor function through rTMS are up-regulating the excitability by giving high frequency stimulation to primary motor cortex of ipsilesional hemisphere according to interhemispheric competition model, and down-regulating the excitability by giving low frequency stimulation to primary motor cortex of contralesional cerebral hemisphere [11]. Previous studies showed that both methods significantly improved the upper limb motor function of chronic stroke patients [12,13]. However, there has not been much research on the effects of high and low frequency stimulation, so it is still unclear which type of stimulation is more effective in upper limb motor function. In addition, there has not been much research on rTMS on acute or subacute stroke patients despite the fact that acute and subacute periods after stroke show the fastest natural recovery in the widest range and are thus very important in rehabilitation therapy [14,15,16].
Therefore, in this research, we compared the effects and safety of low frequency (1 Hz) and high frequency (20 Hz) rTMS in subacute stroke patients.
MATERIALS AND METHODS
Subjects
The subjects were selected from patients who were hospitalized at our rehabilitation department for stroke hemiplegia from 2011 to 2013. The criteria were <4 weeks after first subacute ischemic stroke, declined upper limb motor function on the opposite side of the lesion, ability to undergo continuous rehabilitation therapy, and ability to understand and carry on the treatment and evaluation by the medical faculty.
Those who had complications that required intensive medical managements, such as pneumonia, heart failure, urinary tract infection, or poor nutritional state, or common contraindications of rTMS (e.g., metallic substance in the brain like aneurysm clip, cardiac pacemaker, pregnancy, or past history of seizure) were excluded.
Strength and location of stimulation
To decide on the appropriate strength and location of stimulation, we found each patient's hot spot and chose the resting motor threshold (RMT). After attaching the recording electrode on each patient's contralateral abductor pollicis brevis muscle, we carried out rTMS at rest using a 97-mm wide butterfly-shaped coil (MCF-B70; MagVenture, Farum, Denmark) and MagPro R30 with MagOption stimulator (MagVenture). To have the electromagnetic current perpendicular to the central sulcus, the coil was set at 45° to the central line and stimulation was carried out on the scalp every 1 cm to find the hot spot. When we found the hot spot, single pulse TMS was performed at the location, with RMT defined as the minimum strength showing motor-evoked potential peak-to-peak amplitude >50 µV in more than five of 10 stimulations.
rTMS stimulation methods
Subjects were divided into a low frequency (1 Hz) rTMS group and high frequency (20 Hz) rTMS group. Each subject received 10 treatment sessions over 2 weeks. The low frequency group received 1 Hz frequency stimulation on the hot spot of the M1 region (the motor cortex area at the contralesional hemisphere) at 120% of RMT for 150 seconds and rested for 30 seconds. This was repeated 10 times, for a total of 1,500 pulses of stimulation. The high frequency group received 20 Hz frequency stimulation on the hot spot of the M1 region (the primary motor cortex of the ipsilesional cerebral hemisphere) at 90% of RMT for 5 seconds and rested for 50 seconds. This was repeated 20 times, for a total of 2,000 pulses of stimulation. The TMS protocol used in this research was performed according to the safety guidelines for rTMS [17]. All the patients received palliative rehabilitation treatment and drug therapy. Occupational therapy immediately followed. During the rest period of treatment, exercise training including active assistive range of motion exercise of the affected extremity and holding, moving, and releasing of cups and cubes were administered by the medical faculty. For safety, each patient was clinically monitored by medical and neurologic examination during rTMS sessions. Vital signs including blood pressure, heart rate, and level of consciousness were evaluated before and after rTMS sessions.
During the research, all the patients received conventional rehabilitation that included range of motion training, muscle exercise, fitness training, gait training, and activities of daily living training for 60 minutes from an average of 3 days after the onset of disease. All of the patients also received conventional medical treatment, such as management of blood pressure and anticoagulant or antiplatelet therapy.
Evaluation of upper limb function and activities of daily living performance
To discern whether upper limb function and activities of daily living performance had improved, manual function test (MFT) [18], upper limb score in the Fugl-Meyer Assessment (range 0-66) [19], Modified Barthel Index (MBI, range 0-100) [20], Brunnstrom recovery stage [21], and grip strength [22] were performed to compare the results of the two groups before and after rTMS, and one month after the end of the last rTMS session.
Statistical analyses
Statistical analyses were done with the SPSS ver. 18 (SPSS Inc., Chicago, IL, USA). Data are presented as mean±standard deviation. The general characteristics of the two groups were analyzed with Mann-Whitney U test and Pearson chi-square test. Within each group, mean value comparison of Fugl-Meyer Assessment Scale, MFT, Brunnstrom stage, Modified Ashworth scale, MBI, and grip strength of before, after, and one month after the treatment was done with repeated measures ANOVA and post-hoc tests were done using Bonferroni correction. The difference between the two groups was measured by independent t-test, with statistical significance defined as p<0.05.
RESULTS
All the patients completed their rTMS sessions. No adverse side effects were reported during the course of the experiment using consecutive multi-session high or low frequency rTMS.
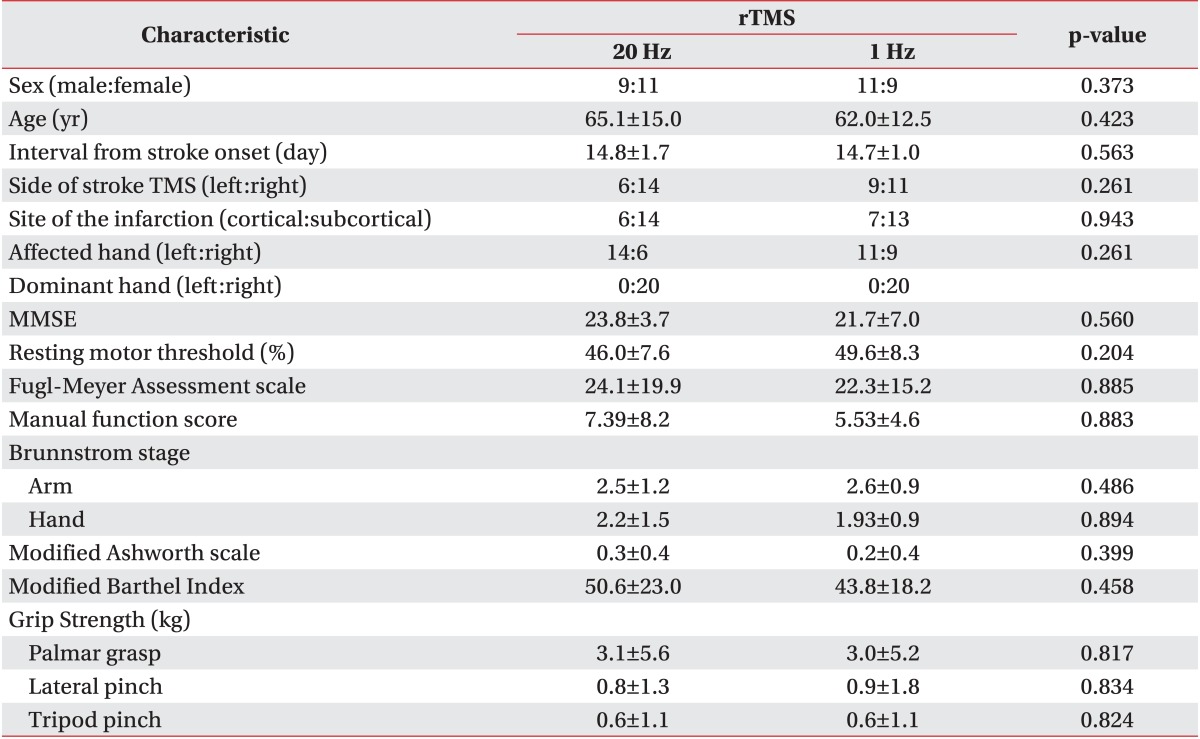
Twenty patients received low frequency (1 Hz) rTMS, and the other 20 received high frequency (20 Hz) rTMS. In the low frequency group, there were 11 males and 9 females and in the high frequency group, there were 9 males and 11 females, so there was no significant difference in the distribution of sex. The average age of the low frequency group was 65.1 years and that of high frequency group was 62 years. All the patients were right hand dominant. In the low frequency group, 9 patients had the lesion in their left hemisphere, and 11 in their right hemisphere. In the high frequency group, the numbers were 6 and 14, respectively. On average, the low frequency group received rTMS 14.7 days after disease occurrence, and high frequency group received rTMS 14.8 days after disease occurrence. No significant differences were evident in any of the variables (Table 1).
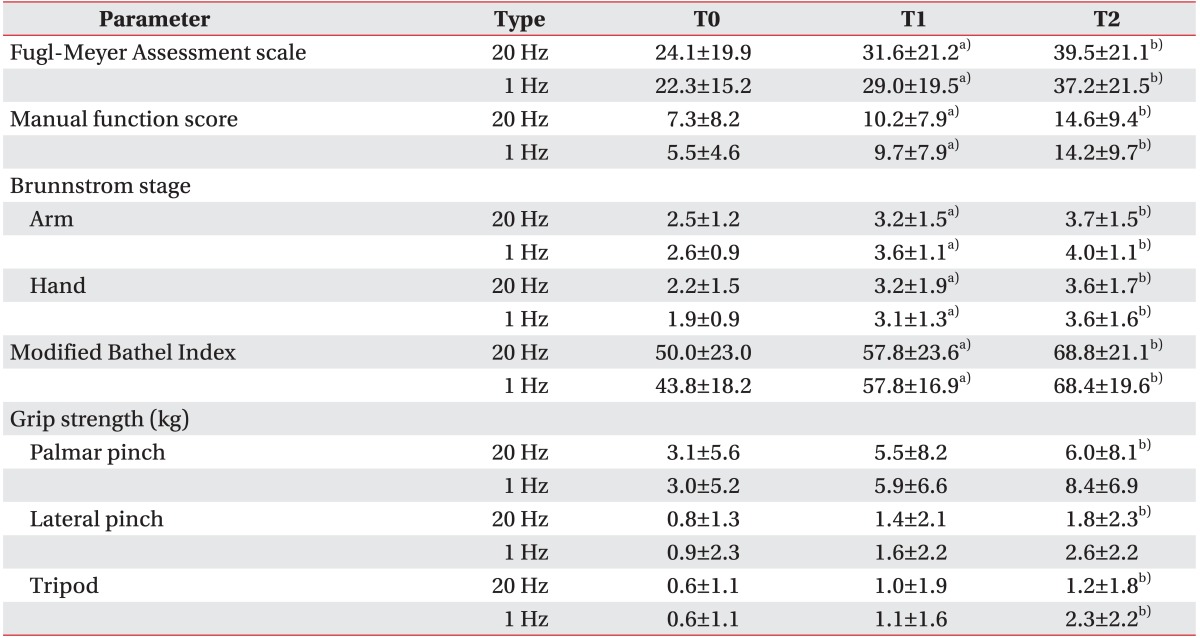
Both groups showed statistically significant improvement in Fugl-Meyer Scale, MFT, Brunnstrom, and MBI right after treatment and one month after treatment when compared to before treatment (p<0.05). Although the two groups showed a trend of improvement in palmar grasp, lateral pinch, and tripod pinch in grip strength, there was no statistically significant difference before and after treatment in the high frequency group, while there was a statistically significant difference before and one month after treatment. In the low frequency group, there was no statistically significant difference in grip strength before, after, and one month after treatment (p>0.05). Consequently, there was no statistical difference between two groups in the extent of improvement before and after rTMS treatment (Table 2).
DISCUSSION
In this research, we found out that low (1 Hz) and high (20 Hz) frequency rTMS can be safely administered to subacute stroke patients without side effects, and that both groups showed improvement in upper limb motor function.
Recently, many post-stroke treatment options including non-invasive TMS have been suggested as new strategies in the neurorehabilitative setting [23]. rTMS can improve motor function after stroke and, according to the interhemispheric competition model, high frequency stimulation can be administered to the primary motor cortex of the ipsilesional cerebral hemisphere to up-regulate excitability or low frequency stimulation can be administered to the primary motor cortex of the contralesional cerebral hemisphere to down-regulate excitability [11]. Low frequency stimulation to the intact cerebral hemisphere can significantly improve upper motor limb function in chronic stroke patients [13]. Due to both seizure risk and unproven efficacy, some researchers argue that rTMS on the primary motor cortex of the ipsilesional cerebral hemisphere should be better understood and researched before implementation [24]. However, recent research shows that high frequency rTMS is safe for adults, adult stroke patients, and even children [12,25,26]. In this research, daily TMS sessions were well tolerated and side effects, such as seizure, were not observed in the high frequency group.
Consecutive multi-sessions of rTMS at a frequency of 10 Hz can produce significant motor function improvement in subacute stroke patients [27]. Our research went further and used a frequency of 20 Hz to show that high frequency consecutive multi-sessions of rTMS can be administered safely without side effects, and confers a significant improvement in upper limb motor function. It should be noted that the improvement lasted until one month after treatment.
The long-term effects (i.e., until one month after treatment) could reflect the capacity of rTMS training combined with upper limb motor practice in the subacute stage of stroke to promote engagement in better quality upper limb practice from an earlier stage of stroke [12,27]. Secondly, multi-session cumulative rTMS treatment might provide a long-lasting effect [28]. Although changes in cortical excitability were not assessed after each rTMS session in this study, previous research has shown that multi-session rTMS produces a greater effect on cortical excitability [29]. Further study is needed to confirm the possible mechanisms of long-term effect of rTMS in stroke patients.
Previous studies showed that both frequency methods significantly improved the upper limb motor function of stroke patients compared to the sham group [12,13,27]. However, comparison of the effect of high and low frequency stimulation has not been done, so it is still unclear which type of stimulation is more effective in upper limb motor function.
In a prior study, one daily session for 5 consecutive days was administered to nine patients in the high frequency (10 Hz) group and 11 patients in the low frequency (1 Hz) group, and the high frequency group showed significantly greater improvement compared to the low frequency group [30]. However, in the present study, each group with 20 subacute stroke patients received one session for 10 consecutive days, and there was no statistically significant difference between the two groups after treatment, and one month after the treatment. Therefore, we cannot conclude whether high or low frequency stimulation is more effective for upper limb motor function improvement.
The limitations of this study are the relatively few numbers of subjects, absence of sham group to estimate the natural recovery post stroke, and the fact that we could not make the use of functional neuroimaging studies, such as functional magnetic resonance imaging and positron emission tomography. Future studies should include more patients and utilize more functional neuroimaging studies.
In this research, we confirmed that in subacute stroke patients, low (1 Hz) and high (20 Hz) frequency rTMS can be safely administered, and that both groups showed improvement in upper motor function, which lasted up to one month after treatment. However, we cannot conclude whether high or low frequency stimulation is more effective for upper limb motor function improvement. With more patients included in the future studies, this research results can be used as a clinical data in upper motor function recovery in subacute stroke patients.
 XML Download
XML Download