

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The physical growth of children draws a steep curve during the infancy. Likewise, their language abilities remarkably develop during this period. Ordinarily, children utter their first word when they are 12 months old and when they are 24 months old, they are able to pronounce more than 100 words [1]. However, some children may be behind others in language development.
Children, who are at least one year behind others, are diagnosed as language developmental delay. It has been reported that language developmental delay occurs in 5% to 8% of the child population [2,3,4]. Language developmental delay is diagnosed by standardized assessment tools, such as the Sequenced Language Scale for Infants (SELSI) or the Preschool Receptive-Expressive Language Scale (PRES). Such assessments are conducted only by professionally-trained speech therapists and they are expensive and time consuming. Actually, it takes more than 30 or 40 minutes [5,6]. Such problems led to a need for a simple screening test that can be conducted prior to SELSI or PRES. The MacArther-Bates Communicative Development Inventories (M-B CDI) was developed and has been proved to be reliable and valid. Currently, it is used throughout the world, being translated into English, Danish, and Swedish [7,8,9]. Recently, a Korean version named M-B CDI-K was provided and its usefulness has been proved in a study [10]. However, the M-B CDI-K is still expensive and time consuming because it was composed of many subsections. Besides, some questions are too professional for any respondents. Therefore, a M-B CDI-K short form version was developed in 2008 [1,11]. This test is divided into two types: one is for children aged between 9 and 17 months and the other one is for children aged between 18 and 35 months. The first type is composed of understanding score, expressing score, and playing with things score, and the second type is composed of understanding score, expressing score, and grammar score. It has the merit of being simple and easy enough to fill up brief questionnaires in a short time [1]. For these reasons, this study was carried out to investigate the effectiveness of M-B CDI-K short form as a screening test compared with SELSI or PRES.
Go to : 
MATERIALS AND METHODS
This study was conducted on 87 children whose chief complaints were speech and language delays and who visited the Department of Rehabilitation Medicine or the Developmental Delay Clinic of Ilsan Hospital between April 2010 and May 2012. The study protocol was approved by the ethics committee of the National Health Insurance Service Ilsan Hospital, Ilsan, Korea.
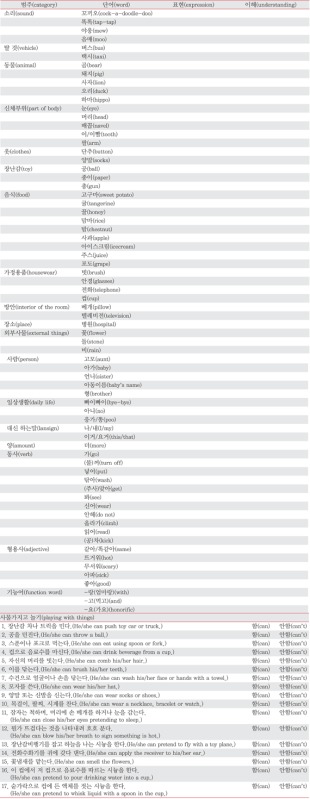
All children underwent physical and neurologic examinations by medical staff. Their parents or guardians filled up the M-B CDI-K short form, a screening test, after being given a speech therapist's explanation. In addition, the children took diagnostic language assessments according to their developmental age. Their cognitive functions were tested with Korean Bayley Scales of Infant Development- II (K-BSID-II) or Korean Wechsler Preschool and Primary Scale of Intelligence (K-WPPSI). Their language abilities were assessed with SELSI or PRES: the former was for children under the age of 3 years and the latter for preschoolers above the age of 3 years. But, SELSI was conducted in some children whose language levels were inadequate for PRES. Language developmental delay was defined as language age below 2 years as standard deviation of SELSI or language age was at least 1 year behind normal on the PRES [5,6]. In the M-B CDI-K short form, parents or guardians checked on words that children could understand or express, on their gestures or behaviors, and on the levels of their abilities to verbalize expression of sentence and grammatical sentence (Appendix 1). Based on the results, the children were classified into a high risk group and the non-high risk group. And then we compared the M-B CDI-K short form with SELSI or PRES [1].
Go to :
RESULTS
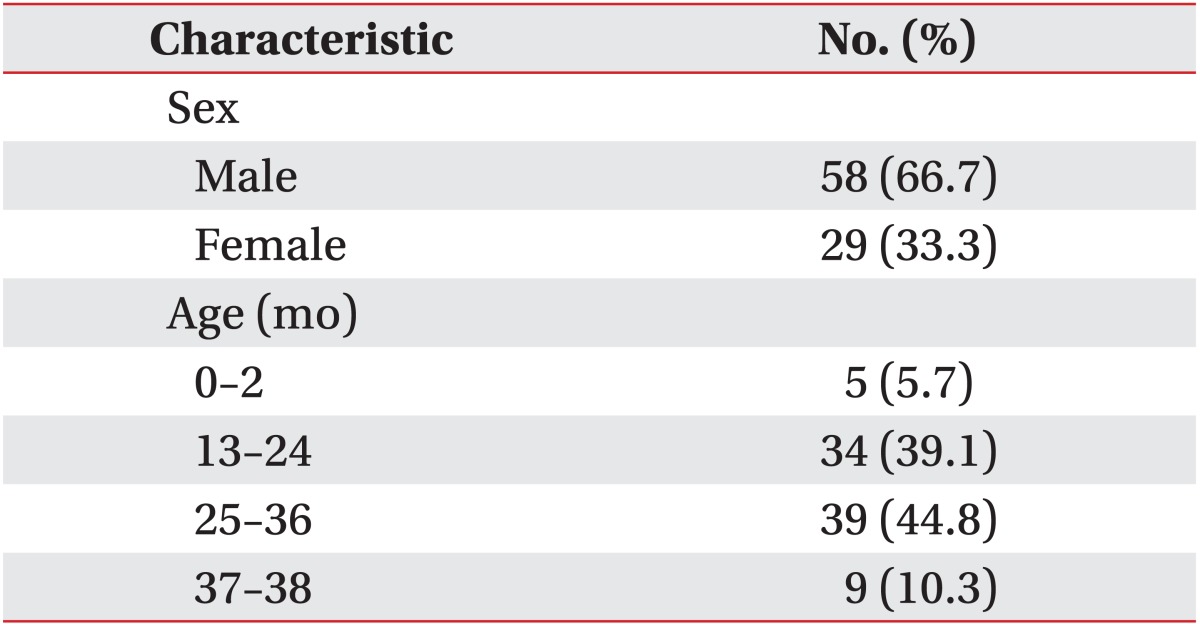
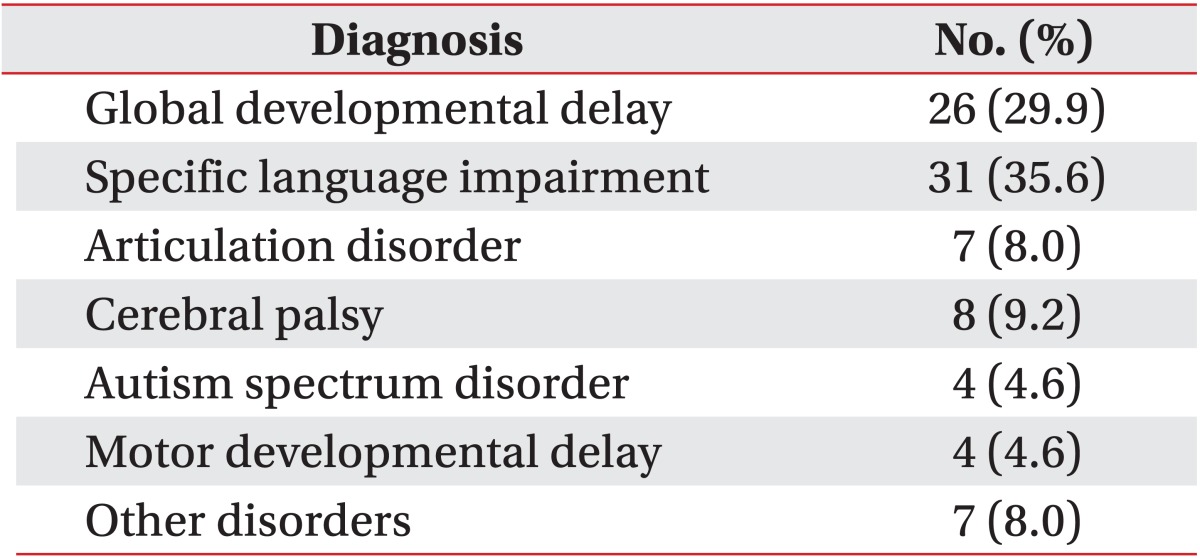
This study included 87 children, 58 boys and 29 girls. Their average age was 25.9 months. Eighty-five out of 87 were tested with SELSI and the other 2 were tested with PRES (Table 1). We included 9 children aged between 37 to 38 months old because their language development stage was considered below 36 months. And 7 out of 9 children completed SELSI because they could not perform PRES. Twenty-six children were diagnosed with global developmental delay, 31 with selective language impairment, 7 with functional articulation disorder, 8 with cerebral palsy, 4 with autism spectrum disorder, 4 with motor developmental delay, and the other 7 with reactive attachment disorder or quadriplegia caused by cerebral hemorrhage and so forth (Table 2).
The results of language assessments are as following: Twenty-six children were diagnosed with global developmental delay, 25 showed language developmental delay on SELSI or PRES and were tested positive for high risk on the M-B CDI-K short form. Another child showed a language developmental delay on SELSI or PRES but was negative tested for high risk on the M-B CDI-K short form. Of 31 children diagnosed with selective language impairment, 29 showed language developmental delay on SELSI or PRES and were positive tested on the M-B CDI-K short form. One child did not show language developmental delay on SELSI or PRES but was positive tested on the M-B CDI-K short form, another child did not show language developmental delay on SELSI or PRES and was negative tested on the short form M-B CDI-K. The seven children diagnosed with functional articulation disorder did not show language developmental delay on SELSI or PRES and were negative tested on the short form M-B CDI-K. Of eight children diagnosed with cerebral palsy showed five a language developmental delay on SELSI or PRES and were positive tested on the M-B CDI-K short form, two did not show language developmental delay on SELSI or PRES but were positive tested on the M-B CDI-K short form. Another child showed language developmental delay on SELSI or PRES but was negative tested on the M-B CDI-K short form. Four children diagnosed with autism spectrum disorder showed language developmental delay on SELSI or PRES and were positive tested on the M-B CDI-K short form. Four children diagnosed with motor developmental delay showed language developmental delay on SELSI or PRES and were negative tested on the M-B CDI-K short form (Table 3).
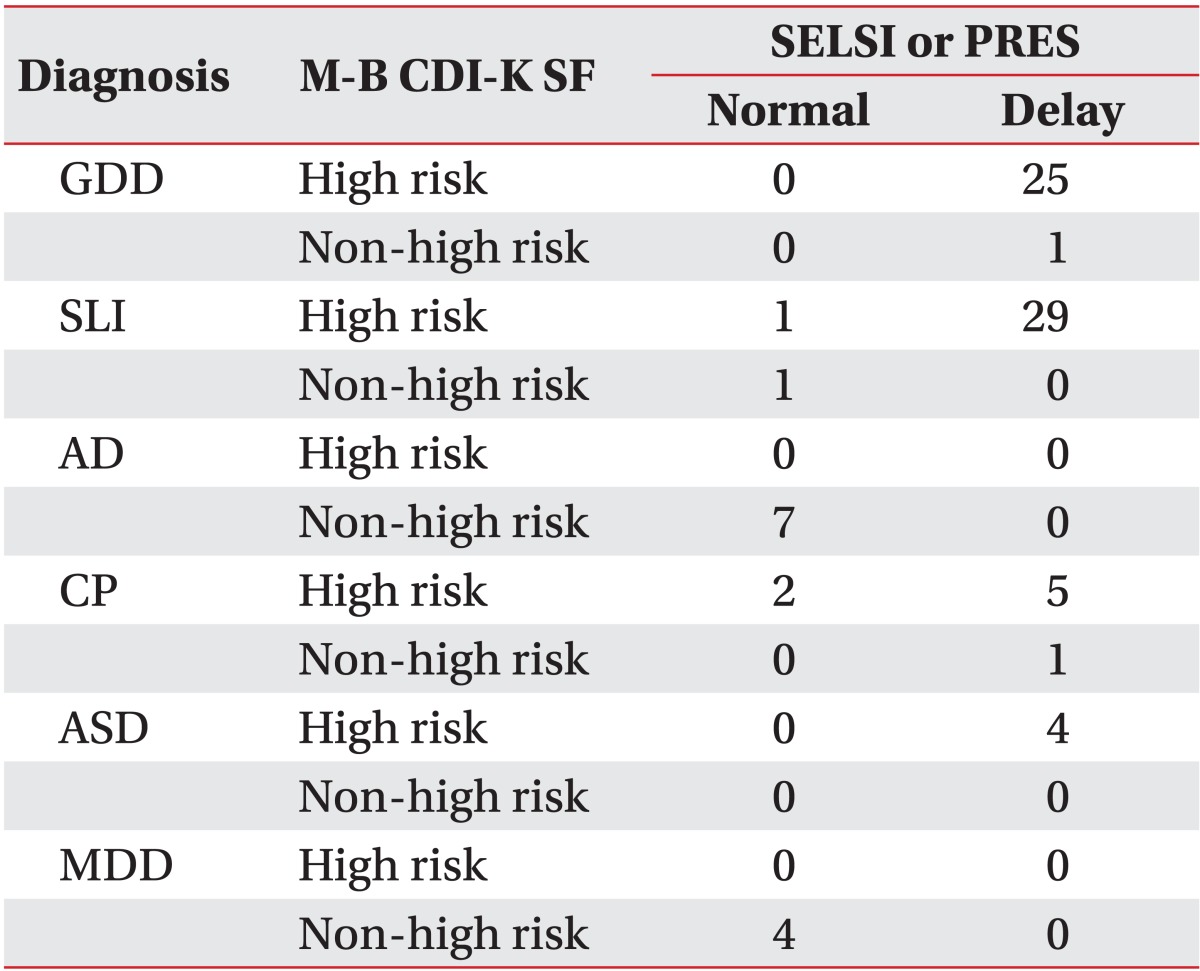
Table 3
Assessment results according to diagnosis
M-B CDI-K, MacArthur-Bates Communicative Development Inventories-Korean; SF, short form; SELSI, Sequenced Language Scale For Infants; PRES, Preschool Receptive-Expressive Language Scale; GDD, global developmental delay; SLI, specific language impairment; AD, articulation disorder; CP, cerebral palsy; ASD, autism spectrum disorder; MDD, motor developmental delay.
![]()
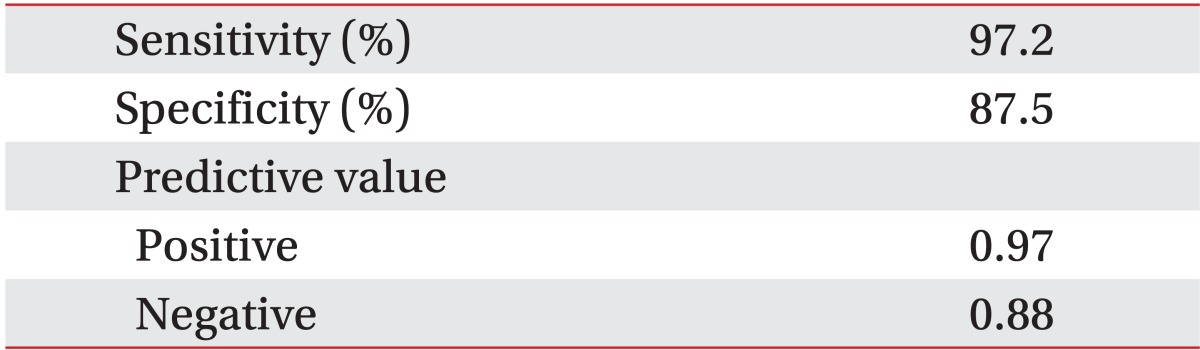
In our final analysis, 71 children showed language developmental delay on SELSI or PRES and 69 of them were positive tested for a high risk on the M-B CDI-K short form. Of 16 children without language developmental delay on SELSI or PRES were 14 negative tested for high risk on the M-B CDI-K short form. As for the M-B CDI-K short form, the sensitivity and specificity reached 97.2% and 87.5%, respectively and the positive predictive value and negative predictive value were worked out at 0.97 and 0.88, respectively (Table 4).
Go to :
DISCUSSION
Language developmental delay was easily observed in children with delayed development. In previous studies was language developmental delay reported as chief complaint in 41% of children who visited the children development clinic [12]. Since language developmental delay may improve with advancing years, there were a lot of controversies over treatment timing, therapeutic effects and necessity. However, it may negatively influence children's abilities to communicate, learn, and socialize if it is not diagnosed and treated early [2,13]. Thus, an early screening test is crucial for early diagnosis and treatment.
The M-B CDI-K short form has various advantages to evaluate the language developmental delay in infants and children [1]. It can be conducted even by nonprofessionals and sets fewer questions than other existing assessment tools and thus, it saves time and is economical. Actually, it can be finished within 5 minutes. Vocabularies used in the M-B CDI-K short form covered vocabularies of the original version and had a high relevance to the original. So, the M-B CDI-K short form provided high reliability [1]. However, we must not confirm the diagnosis of language developmental delay when children were positive tested for a high risk on the M-B CDI-K short form because it was just a screening test. Therefore, more detailed assessments should be given to children judged to be in the high risk group. Also it should be considered that the test may be subjective because the questionnaires were filled up by parents or guardians.
The Denver Developmental Screening Test (DDST) or the Ages and Stages Questionnaire (ASQ) has been used to assess the developmental status, but they have been found to be inferior to the M-B CDI-K short form regarding their sensitivity and specificity [14,15,16,17]. Further, there was a report that DDST is valueless as a screening test for speech and language development [18]. Therefore, DDST had a low value as a speech and language screening test.
In this study, there were about two times more boys than girls. It showed a similar ratio to previous studies where boys and girls with language developmental disorder as chief complaint were at a ratio of 2:1 to 3:1 [2,19].
The M-B CDI-K short form has been found to be cost-saving, time-saving, reliable, and valid, and thus can be an effective screening test for speech and language development. Commonly, screening tests are regarded as effective when their sensitivities and specificities reach at least 70% to 80%. The M-B CDI-K short form satisfied such conditions as its sensitivity and specificity reach 97.2% and 87.5%, respectively [20,21].
This study was conducted with 87 children whose chief complaints were speech and language delay and who visited the Department of Rehabilitation Medicine or the Developmental Delay Clinic at our hospital between April 2010 and May 2012. The study was carried out to investigate the effectiveness of the M-B CDI-K short form as a screening test, comparing it with SELSI or PRES. As a result, the M-B CDI-K short form showed a high sensitivity (97.2%), specificity (87.5%), positive predictive value (0.97), and negative predictive value (0.88). The results suggest that the M-B CDI-K short form may be effective to screen children suspected to have language developmental delay. Further study is needed about the M-B CDI-K short form including more children with normal and various diseases.
Go to :
 XML Download
XML Download