

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The short- and long-term effects of initial percutaneous coronary intervention (PCI) on acute myocardial infarction (AMI) have been shown [1]. However, the reports on the likelihood of recurrence and restenosis have also followed [2]. To terminate the progression of coronary atherosclerosis after the procedure, risk factors need to be controlled with methods including low-fat/low-cholesterol diet, weight loss, smoking cessation [3] and drug treatment, such as antiplatelet and lipid lowering agents [4,5]. Regular exercise therapy is also essential for prevention of cardiovascular disease (CVD). When the exercise-based cardiac rehabilitation (CR) was carried out, total mortality, cardiovascular mortality and fatal refraction decreased significantly [6,7], and cardiorespiratory fitness and psychological profiles improved [8]. Thus, the total cholesterol, triglyceride and systolic blood pressure (BP) decreased [6]. When a drug-eluting stent (DES) was inserted in place of the metallic stent, the in-stent restenosis significantly decreased, but the safety concern of blood clots inside stent still remained a problem [9,10,11].
In the preceding study, the authors confirmed that CR could significantly delay the in-stent restenosis, regardless of the type of advancing DES [12]. However, stent insertion at the atherosclerotic lesion, progression of coronary atherosclerosis still remained problem. Ornish et al. [13] reported that the group of patients who received usual care without PCI showed progression of coronary atherosclerosis, which occurred after one to five years. However, there is no experimental study that further observes the degree of stenosis progression in de novo lesion (where a stent has not been inserted) of patients who received PCI with DES.
In this study, we compare the degree of stenosis progression in de novo coronary lesion of the CR group which received CR, with the control group which did not receive CR. Patients in both groups had DES insertion and received the latest drug treatments.
MATERIALS AND METHODS
Study subjects
The subjects of this study were patients who were hospitalized at our hospital's cardiovascular center due to acute coronary syndrome (ACS) and successfully received PCI using DES, between April 2008 and June 2010. These patients were scheduled to receive follow-up coronary angiography (CAG) after nine months. A PCI was considered 'successful' if the residual diameter stenosis decreased by less than 30% [14].
After the orientation on the necessity of CR, details of the program were distributed to all patients, and they were encouraged to participate in the CR program. The patients were free to decide, and those willing to receive CR program were placed in the CR group, and the rest were included in the control group. Patients in the CR group with a past history of CVD or cerebrovascular disease, or who had neuromusculoskeletal diseases and were restrained from participating in exercise programs were excluded from the study. The study protocol was approved by the Institutional Review Board of the hospital (IRB No. SPIRB-13-056).
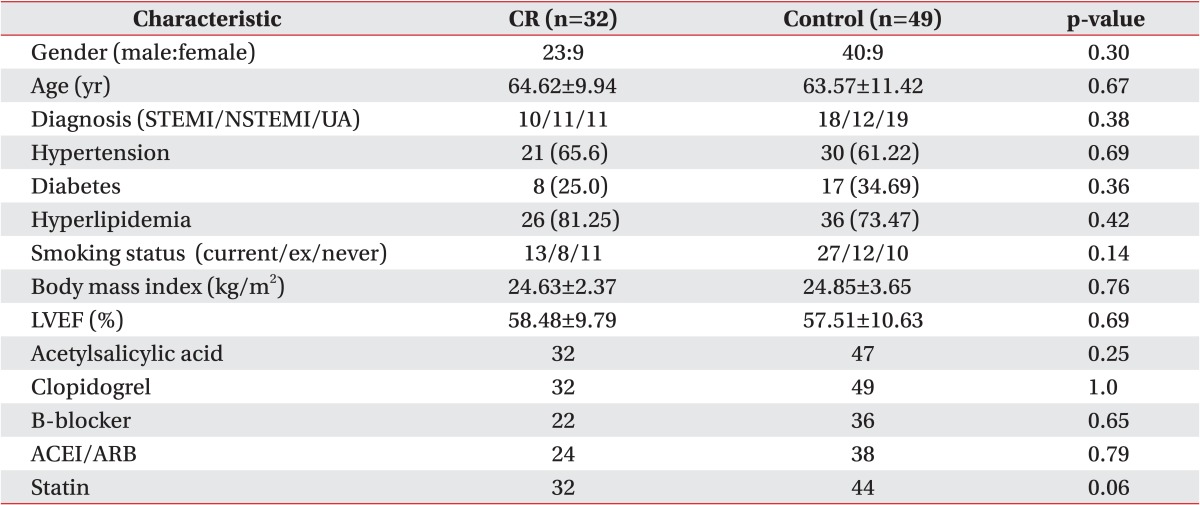
There were a total of 81 subjects, with 32 in the CR group and 49 in the control group. In the CR group, 23 were men and 9 were women; and in the control group, 40 were men and 9 were women. Thus, there was not much of a difference in the gender distributions of the two groups. The average ages of the CR and the control groups were 64.62 and 63.57 years, respectively, with a minimal difference. Table 1 compares the two groups according to the types of ACS, left ventricular ejection fraction (LVEF), number of CVD-related risk factors, and types of drugs taken on their first visit to the CR clinic.
Method
The patients in the CR group received PCI, and once they were discharged from the hospital, they were to visit the CR clinic for preliminary examination, including the graded exercise test (GXT). The exercise-based CR program was to start at the hospital fourteen days after the disease occurrence. GXT was performed using the limited approach to symptoms, as according to the modified Bruce protocol.
Heart rate (HR) reserve was calculated according to each patient's maximum HR and resting HR obtained by GXT; and 40%-85% of that value was set as the target HR. Each patient was monitored by objective measures of electrocardiogram, HR and change in BP, and subjective measure of Borg's rate of perceived exertion (RPE). Each exercise session was composed of a 10-minute warm-up, a 30-minute main exercise, and a 10-minute cool-down. The main exercise was composed in the following order: 8 minutes of treadmill, 3 minutes of rest, 8 minutes of ergometer, 3 minutes of rest, and 8 minutes of treadmill. Patients participated in the exercise program three times a week for eight consecutive weeks (24 times in total). Through the outpatient CR program, the CVD-related risk factors were also strictly controlled. After eight weeks of exercise program in the hospital, GXT was performed again. Based on the target, HR and RPE were obtained simultaneously, and patients were given exercise prescriptions for individual home exercises for nine months after the ACS occurrence. Following up on the exercise programs, the CR clinic encouraged the patients to exercise during the visits. The control group who did not participate in CR program was educated on risk factor management after occurrence of first ACS, and they were also obligated to perform individual exercises at home.
After their first ACS occurrence, patients in both groups received identical follow-up and drug treatment at both the cardiology outpatient clinic and CR clinic. After nine months of ACS occurrence, patients in both groups received CAG and took their first PCI with the interventional cardiologists, who also delivered them one-on-one comparison test with de novo coronary artery. The de novo lesion was defined as coronary lesion of diameter stenosis between 30%-70% without coronary intervention at the time of first CAG.
We defined de novo lesion as vessels whose degree of stenosis was from 30% to 75% and were not within the target of first PCI. We measured the residual diameter stenosis (%) of target lesion using minimal luminal diameter, and calculated late luminal loss and percent luminal loss at the time of first PCI and nine months thereafter. We compared the results between the CR group and the control group. Thus, we defined the newly developed binary stenosis as cases in which coronary stenosis was less than 50% at the time of the first PCI, but progressed to over 50% at CAG follow-up [15].
Statistical analysis
The data was statistically analyzed with SAS Enterprise Guide 4.1 (SAS Institute Inc., Cary, NC, USA). In order to compare the gender, age, and LVEF at the time of first GXT between the CR group and the control group, independent t-test was used. Pearson χ2 test was used to compare the number of patients with ST elevation myocardial infarction (STEMI), non-ST elevation myocardial infarction (NSTEMI), unstable angina, hypertension, diabetes and dyslipidemia, the smoking status, body mass index, and drugs that were currently taken. For comparison of the rate of stenosis of de novo coronary lesion between the CR group and the control group, independent t-test was used. For comparing the data at baseline and at nine months within the group, paired t-test was used. Pearson χ2 test was used to compare the binary stenosis in the CR group with the results at nine months. Using R, the observed power of late luminal loss and late loss were analyzed. Statistical significance was defined as p-value of less than 0.05.
RESULTS
Quantitative coronary angiography results at nine months
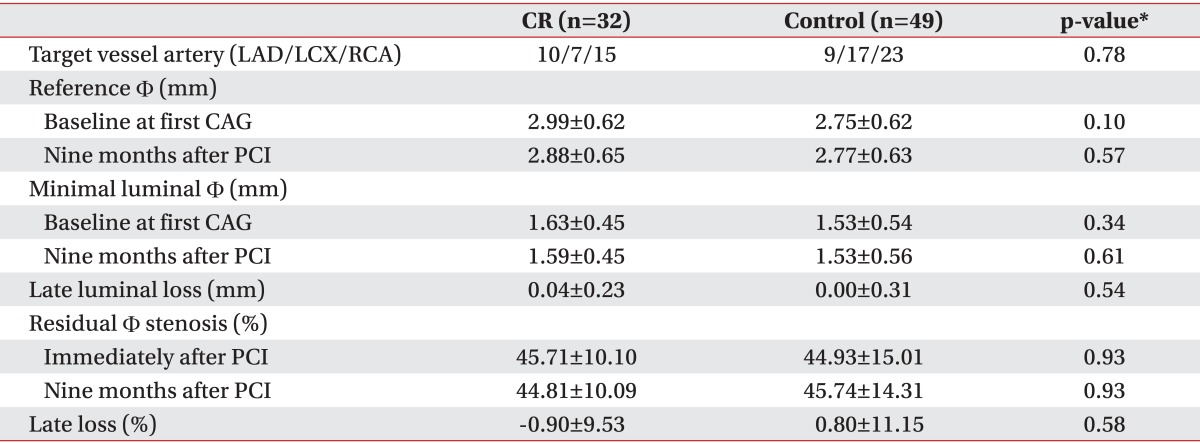
The location of target vessel artery and early reference diameter did not show statistically significant difference between the two groups. The follow-up CAG performed at nine months after the first PCI showed that there was no statistically significant difference from the minimal luminal diameter measured at initial PCI. There was also no statistically significant difference in the late luminal loss between the two groups (p=0.54, observed power=0.10). The residual diameter stenosis (%) after PCI and at nine months also showed no difference within the two groups (p=0.93, p=0.93). The late loss in the CR group changed by -0.90%±9.53% and 0.80%±11.15% in the control group, but the difference was not significant (p=0.58, observed power=0.05) (Table 2).
Progression of de novo lesion at nine months
In the CR group, cases of binary stenosis with diameter stenosis of over 50% decreased from 11 at the start of the study to 10 at nine months. In the control group, the numbers increased from 18 to 19 (p=0.76, p=0.74). There were four and five new cases of binary stenosis in the CR and the control group, respectively. There were seven and four cases in which diameter stenosis of target vessel with binary stenosis decreased to less than 50% in the CR and the control groups, respectively. At the follow-up of nine months, there were two patients who needed revascularization procedures in the control group, while there were none in the CR group (p=0.24). There was no statistical significance for any of the above measurements (Table 3).
Improvement of exercise capacity following exercise-based CR
In the cardiac rehabilitation group that performed the rehabilitation program for nine months, mean maximal oxygen consumption (VO2max) improved significantly from 24.36±5.00 to 27.68±5.24 mL/kg/min (p=0.00001) (Table 4). In the control group, there was no data for VO2max.
DISCUSSION
Mortality rate of coronary heart disease is decreasing, while the prevalence rate is gradually increasing [16,17]. In the case of AMI, ability to perform activities of daily life decreased even after PCI, with a decline in quality of life [18]. Coronary atherosclerosis and its risk factors persist after PCI, and the possibilities of stent thrombosis and restenosis also remain. Such may lead to recurrence of AMI and eventually death [5]. The importance of CR has been gaining attention as a solution, and it has been shown that exercise program with exercise prescription, nutritional counseling, smoking cessation program, drug treatment and weight management can improve the quality of physical activities in daily life and prognosis in secondary prevention [19].
The authors have indicated in a preceding study that the progression of in-stent stenosis rate and in-stent restenosis over 50% were significantly different in CR and control groups, while irrelevant with the type of DES in each generation [12]. Coronary atherosclerosis and its risk factors prevent arterial dilatation by endothelial dysfunction, inflammatory cell, and platelet dysfunction [19,20]. The proliferation of arterial endothelium corresponds to late luminal loss following stent insertion [21]. It is closely related to the endothelial sheer stress [22] and inflammatory responses from damages in blood vessels, accompanied by an increase in high sensitive C-reactive protein (hs-CRP) [23]. Munk et al. [24] states that when high-intensity exercises were performed for over 3-6 months, the in-stent restenosis decreased in patients who received PCI. This is due to the activation of nitric oxide synthase from the improvement in endothelial function. Therefore, such a decrease in hs-CRP facilitating the atherosclerosis will lead to a decrease in endothelin-1 production, which worsens the entire endothelial function [24].
In this study, we compared the degree of stenosis in de novo lesion, at the time of PCI and nine months after the PCI, between the CR and the control groups. Between the two groups, we compared the cases of binary stenosis and cases in which revascularization procedures were needed, and there was no statistically significant difference. We believe that this is due to the efficacy of the latest drug treatment which delays the progression of atherosclerosis of de novo lesion, regardless of participation in the CR program.
Schuler et al. [25] reported that coronary artery disease not only progresses slowly but even regresses in some cases, as compared to the control group. This group received the usual care, while the patients in the experimental group underwent intensive physical exercise involving 30 minutes of daily ergometer program (with intensity of reaching target heart rate). The regimen was exercised everyday with an hour of group exercise twice a week, combined with a low-fat diet [25]. Ornish et al. [13] also reported that when intensive lifestyle modifications, including aerobic exercise, was prescribed to patients in place of PCI, the regression of coronary atherosclerosis occurred one to five years later compared to control group, who received the usual care only. It seems that we may not have statistically significant results, because our study was of relatively short duration at nine months. A study of longer than one year duration is likely necessary.
The limitations of the study are as follows: First, as the patients chose to participate in the CR program or not, those with high risks of exercise-related cardiac attacks were not assigned to the self-exercise group, and hence it was not a random comparative study. Second, we did not see the difference between the two groups when managing for risk factors, such as hypertension, diabetes, dyslipidemia, obesity, and/or smoking. Third, there were a small number of patients, with the small sample size considered a common limitation in studies comparing restenosis after DES insertion. Fourth, while a patient's previous exercise level has an effect on the results, there is no evaluation of such. Fifth, the study period was at nine months, which was somewhat short for the study of the long-term effects of exercise regimen on coronary atherosclerosis. In future, a longer period of randomized study involving more participants is necessary.
In conclusion, short-term CR of nine months did not show significant efficacy on progression of atherosclerosis of de novo lesion, for patients which did not receive PCI. It seems to be from the effectiveness of the latest drug treatments in preventing the progression of atherosclerosis. However, the positive effect of CR on blood vessel with stent insertion in PCI has been shown in preceding studies. Thus for patients who received PCI, a proper drug treatment and CR are essential to prevent relapse and death.


 XML Download
XML Download