

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Joint hypermobility, a condition in which a joint stretches beyond the normal range of motion (ROM), is classified into single-joint or generalized subtypes [1]. Generalized joint hypermobility (GJH) is associated with inherited connective tissue disorders in children, musculoskeletal injuries in athletes, and rheumatic diseases in adults [2,3]. Controversy persists about whether asymptomatic GJH is pathologic in nature, particularly in children [1,4,5].
GJH is commonly diagnosed using the Beighton hypermobility scoring system, the most widely used screening test for hypermobility [1,6]. Using this method, various reports have examined the prevalence of GJH in different ethnicities, sexes, ages, and body sides. GJH is more common among West Africans, females, and the nondominant side than among other ethnicities, males, and the dominant side, respectively [2,4,7-9]. However, little is known about the prevalence of GJH in Koreans [10].
The prevalence of GJH has been suggested to decrease with age in children [2,6]; however, some controversy remains concerning the decline in joint mobility with age [1,11]. Moreover, few studies have examined differences in joint mobility in children vs. adults. Furthermore, whether the use of the adult Beighton cutoff score, generally 4 points, in children is appropriate remains to be clarified [5,6].
The present study was conducted to examine the prevalence of GJH in healthy East Asians and to determine whether the degree of GJH differs between children and adults. A comprehensive analysis was performed to investigate localized hypermobility in each joint and compare the side-by-side differences. Subjects were confined to the Korean race and female sex to minimize variations related to ethnicity and sex.
MATERIALS AND METHODS
Subjects
Two groups of females were enrolled from March to September 2008, a group of girls from an elementary school and a group of women from a directory assistance call center. All 491 female prepubertal girls from the first to sixth grades in an elementary school in Seoul were included in the study. Eighty-seven girls were excluded for musculoskeletal pain, history of fracture, history of menarche, and history of family diseases. As a result, 404 healthy students were included. We included 266 of 383 healthy female workers from a single call center who had no specific complaints or history of musculoskeletal injuries. This study was reviewed and approved by the local ethics committee.
Methods
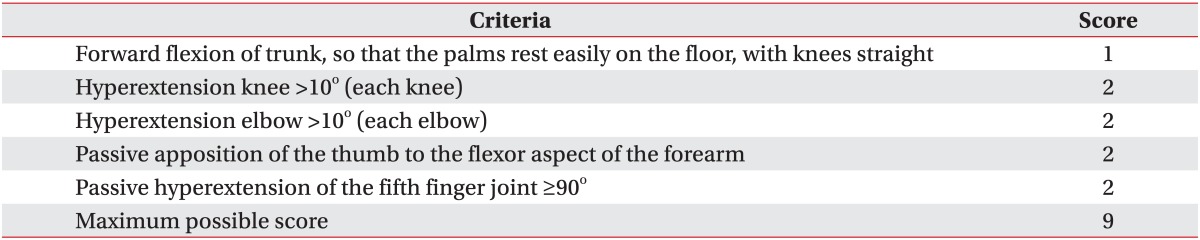
A Beighton cutoff score was used to determine the presence of GJH [12-14] (Table 1). Nine items are scored based on an ordinal scale of 0-9, with a higher score representing greater joint mobility. Each individual item was scored using a nominal scale in which "1" represents a positive sign and "0" represents a negative sign. All measures were obtained bilaterally using a goniometer, with the exception of trunk flexion. A threshold cutoff point of 4 of 9 was used to categorize participants with GJH, as described previously [11,12].
To determine the Beighton score, the subjects were asked to relax their muscles as much as possible, and their joints were then moved through their ROM without evoking pain (Fig. 1). A passive ROM was used to standardize and make the measurements less dependent on the subjects' notion of a full ROM, particularly the girls. Background information about the subjects, including age, dominant hand, and employment duration was obtained using a questionnaire.
We investigated whether the Beighton score significantly differed between the groups of girls and women. We determined the localized score for each joint in cases of a significant difference to determine which joint contributed to the significant difference in total score.
Statistical analysis
All statistical analyses were performed using SPSS ver. 17.0 for Windows (SPSS Inc., Chicago, IL, USA). First, a descriptive analysis was performed. Differences in the Beighton scores and percentages of GJH between the two groups were tested for significance using the t-test or chi-square test as appropriate. The t-test was used to compare differences in localized hypermobility of each joint, whereas Spearman correlation coefficient was used to evaluate the correlation between the Beighton score and several other factors including age and employment duration. The chi-square test was used to test independence or determine the kappa index. Statistical significance was set at a p=0.05 for all tests.
RESULTS
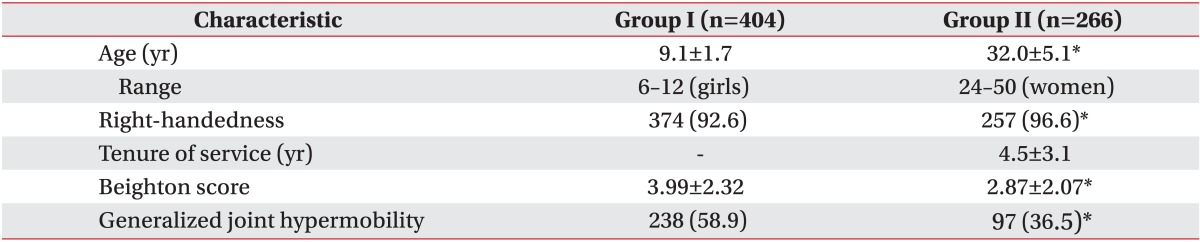
In the group of girls, 404 subjects (age, 6-12 years) were included in the study, the mean (standard deviation [SD]) age was 9.1 (1.7) years. In the group of women, 266 female workers (age, 24-50 years) were included. The mean (SD) age was 32.0 (5.1) years, and the mean employment duration was 4.5 (3.1) years. A total of 374 girls (92.6%) and 257 women (96.6%) were right-handed, indicating a significantly higher percentage in the group of women. A significant difference in mean Beighton score was found between the groups of girls and women (3.99 [2.32] vs. 2.87 [2.07], p<0.05). A total of 238 girls (58.9%) and 97 women (36.5%) had GJH. The percentage of GJH, defined as a score ≥4, was significantly higher in the group of girls than that in the group of women (Table 2). The Beighton score was significantly inversely correlated with age in the groups of girls and women, the correlation coefficients (R) were -0.165 (p=0.001) and -0.143 (p=0.029), respectively. However, no correlation was found between the Beighton score and employment duration in the group of women.
Each localized score was compared by joint to investigate the difference in total Beighton score between the two groups. The right and left side scores were added. Significantly higher scores in the thumbs and fifth fingers were noted in the group of girls than in the group of women (p<0.05). The mean (SD) scores of the thumbs were 0.88 (0.47) and 0.36 (0.35) in the group of girls and women, respectively. The mean (SD) scores of the fifth fingers were 1.23 (0.46) and 0.66 (0.47) in the group of girls and women, respectively. No significant differences in Beighton score were found regarding the back, knee, or elbow joints (Fig. 2).
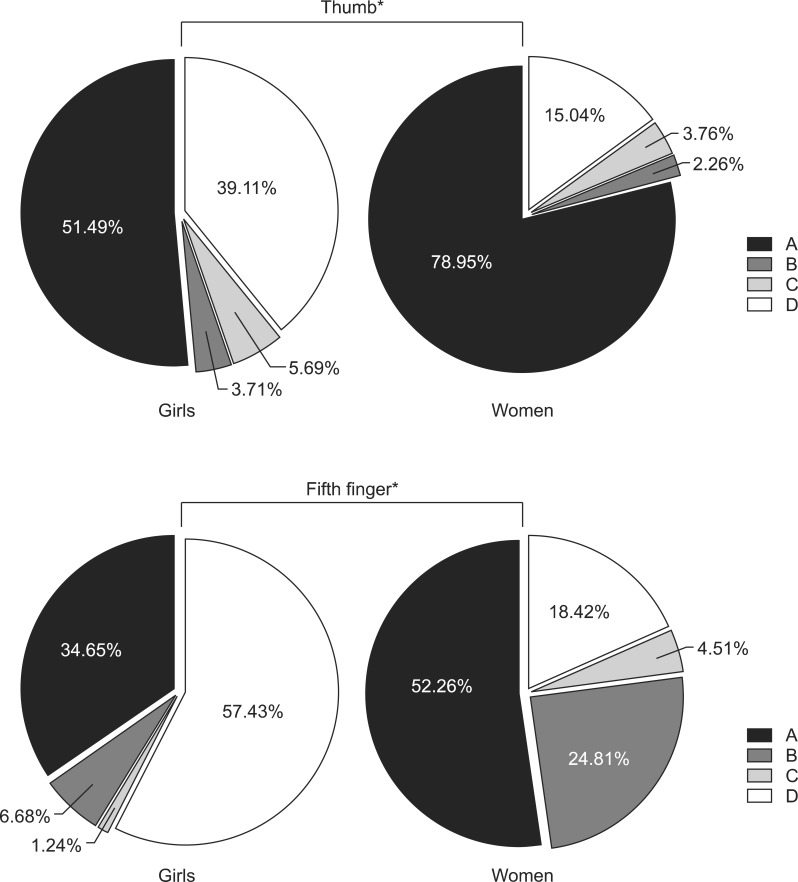
We examined the pattern of hypermobility in the thumbs and fifth fingers between the groups of girls and women using a pie chart (Fig. 3). To reflect bilaterality of hypermobility, the patterns were divided into four groups-A, bilateral nonhypermobility; B, left-sided hypermobility; C, right-sided hypermobility; and D, bilateral hypermobility. First, using the independence test, we confirmed that patterns A-D were significantly different between the two groups for both joints (p<0.001).
In the case of the thumb, the group of girls had the following patterns: A in 208 (51.49%), B in 15 (3.71%), C in 23 (5.69%), and D in 158 girls (39.11%). The group of women had the following patterns: A in 210 (78.95%), B in 6 (2.26%), C in 10 (3.76%), and D in 40 women (15.04%). The group of women had a higher percentage of pattern A and a lower percentage of pattern D in the thumbs compared with the group of girls. In the case of the fifth finger, 140 (34.65%), 27 (6.68%), 5 (1.24%), and 232 girls (57.43%) had patterns A, B, C, and D, respectively, whereas 139 (52.26%), 66 (24.81%), 12 (4.51%), and 49 women (18.42%) had patterns A, B, C, and D, respectively. The percentages of patterns A, B, and C increased, and the percentage of pattern D decreased in the fifth fingers of the women compared with the girls. The fifth finger had a higher increase in the frequency of pattern B compared with the thumb.
A significant agreement was found between the hypermobile fifth fingers and the nondominant hand, mainly the left side, in the group of women for the discrepant patterns B and C (kappa=0.133, p=0.018). Agreement was also observed in the group of girls, though it was statistically insignificant (kappa=0.216, p=0.167).
DISCUSSION
We investigated the prevalence of GJH in healthy female Koreans and determined whether an age-related difference existed. We demonstrated a 50.0% prevalence of GJH in Korean females (58.9% of the girls and 36.5% of the women). We found significantly decreased hypermobility with increasing age, the difference mainly stemming from the loss of localized hypermobility in the fifth finger of the dominant side as one ages.
Our results correspond well with those of earlier studies, which reported that GJH decreases with age in children [6,8,15]. Our study confirmed that GJH decreased with age in adults as well and revealed an age-related difference between prepubertal girls and adult women. Localized hypermobility of the thumbs and fifth fingers decreased significantly in the women compared with the girls; however, the decreasing patterns were not identical. The decrease in mobility with aging originated from the loss of bilateral hypermobility in the thumbs, whereas the decreased hypermobility on the right side was the main cause in the case of the fifth fingers, a finding that was consistent with those of studies suggesting reduced mobility on the dominant side [1,6,16]. Our study showed a GJH prevalence of 50%, a finding that was different from those of other ethnicities (19.5% of Dutch and 57.0% of Nigerians) [4,7]. This is the first study to report on the prevalence of asymptomatic GJH in East Asians. We postulate that Koreans have greater joint mobility than Caucasians but less joint mobility than West Africans.
GJH is associated with localized joint pain, sport-specific injuries, and rheumatic diseases in adults [10,17,18]. GJH is often asymptomatic and poorly recognized in children [1], but subclinical GJH is believed to be associated with inherited collagen disorders, such as Marfan and Ehlers-Danlos syndromes [2]. An effective assessment tool is needed for proper screening and management of GJH. However, a standard cutoff Beighton score to diagnose GJH in children has yet to be confirmed. Our findings indicate that the percentage of GJH in the group of girls decreased when the cutoff point ≥4 was changed to ≥5, demonstrating a decrease from 58.9% to 42.3%. Based on our finding regarding the significant decline of GJH in proportion to age, it seems to be reasonable to set 5 points as the cutoff value of GJH in children, which is 1 point higher than that in adults. These findings correspond to those of earlier studies [1,5,6]. Considering the relatively high prevalence of asymptomatic GJH in children, setting 5 points as the standard cutoff score may increase specificity, suggesting that the Beighton hypermobility scoring system is an efficient screening tool for GJH.
An important finding of our study was that the loss of localized hypermobility in the fifth finger of dominant side, mostly the right, was observed with aging, which mainly contributed to the decreased prevalence of GJH in the women vs. the girls in our study. This decreased mobility is presumed to be attributed to the social and economic features of the Korean society and to anatomical causes. First, degenerative changes in collagen levels in the articular cartilage and skin lead to reduced joint mobility with increasing age [19,20]. Furthermore, Schweitzer [21] postulated that increased tension in the volar plate and flexor tendon in the fingers could limit ROM, which is in close agreement with our findings. Second, there is a predominance of right-handedness in Korea at a significantly higher incidence rate than that in the West and continued enforcement of the use of the right hand as a child grows [22]. The amount of time individuals spend using Internet-related devices has been steadily increasing worldwide, including in Korea [23]. In particular, because the dominant hand is used to grip the mouse, the function of the little finger can be limited to a supportive role compared with the active use of the thumb for gripping and the index finger for clicking; therefore, the restriction is postulated as being the cause of decreased mobility in the fifth finger.
These findings are coincident with those of earlier studies that reported that the fourth and fifth fingers are less functional than the other three fingers due to the differential peripheral motor control in the dominant hand [16,24,25]. Molenaar et al. [26] emphasized the individual evaluation of each localized joint rather than the overall hand function, such as grip power, almost identical to our results. We propose that it is important to consider the physiologically increased generalized hypermobility and decreasing tendency of dominant-hand mobility during the evaluation and follow-up of prepubertal children.
The present study had some limitations. First, it included only females. Second, the applicability of the Beighton score was confined to some joints, so other joints could not be analyzed for hypermobility. Further cohort studies including the male sex and other evaluation tools are needed to evaluate whether the pattern of joint hypermobility in children changes throughout the life cycle.
In conclusion, we demonstrated that female Koreans in our study had a high prevalence of GJH. The incidence of GJH decreased as age increased, as a result of the decreased mobility of the fifth finger on the dominant side.


 XML Download
XML Download