

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Strokes in adults lead to neurological disabilities including limited walking ability, which restricts the patient's social and daily activities. Walking ability is one of the most important factors that allow a person to carry on with their daily activities [1]. Therefore, the assessment of walking ability is essential for future management planning and for the evaluation of patient condition. The World Health Organization (WHO) has stated that the assessment of walking ability and mobility through the International Classification of Functioning, Disability and Health in rehabilitation is fundamental [2].
Since the enhancement of walking ability plays a central role in the rehabilitation of patients who have had a stroke, it is important that there is an accurate tool to assess this improvement in function. Various tests and tools are currently being used in rehabilitation medicine to evaluate a patient's locomotive ability. Examples of these include the Functional Walking Category (FWC) [3], the Functional Ambulation Category (FAC) [4], and the Functional Independence Measure (FIM) [5] of which there are 12 items that assess walking ability. However, these tools have limited capacity to be generalized toward all patients. For example, the FWC was developed to assess outpatients [3], while the FIM and the FAC are more appropriate for assessing inpatients with relatively lower walking abilities [6]. Another limitation with the use of such tools is that these tools show a ceiling effect [7], meaning that they cannot quantify the improvement in the walking ability once patients start to make a certain level of recovery. Other walking speed tests, such as the 10-meter walking test (10MWT) or the 6-minute walk test (6MWT), are useful tools; however, they have been criticized for their limited generalizability because they are conducted under controlled environments, implying that they do not always indicate the actual walking ability in daily life [8]. To overcome such limitations, the ABILOCO (a measure of locomotion ability for adults) was developed by Caty et al. [7] based on the Rasch measurement model [9] in 2008. This was targeted for stroke patients, assessing only the walking ability of such patients in various environments. The test includes 13 tasks, which assess a range of motions ranging from simple movements to more complex movements. It allows an appropriately graded assessment of walking abilities needed for daily life. This tool was first introduced in 2008 by the stated authors and since then, has undergone testing and retesting to show a high validity between the patients and the test as well as high reproducibility [10]. In another test assessing the walking ability of stroke patients before and after botulinum toxin injection, the ABILOCO was shown to reflect well the quantitatively changes in walking ability [11].
However, there is not yet a standardized Korean version of the ABILOCO (K-ABILOCO) and its validity has not been tested. The aim of this study is to produce a standardized K-ABILOCO and assess the reproducibility between the testers through testing and retesting the total score as well as the results of each item of the test. In addition, the association between the K-ABILOCO, the age of the patients, the Korean Mini Mental State Examination (K-MMSE) and the Korean Berg Balance Test (K-BBS) [12] were used for clinical assessment of locomotion. Furthermore, the mobility score of the Korean Modified Barthel Index (K-MBI) and the Korean Modified Barthel Index Mobility (K-MBIM) [13] were tested.
MATERIALS AND METHODS
Korean translation of the ABILOCO
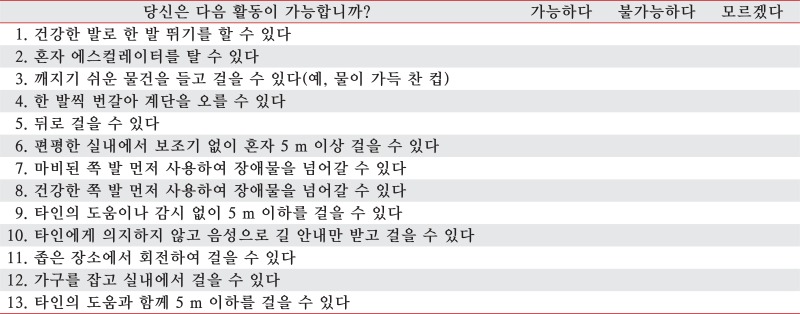
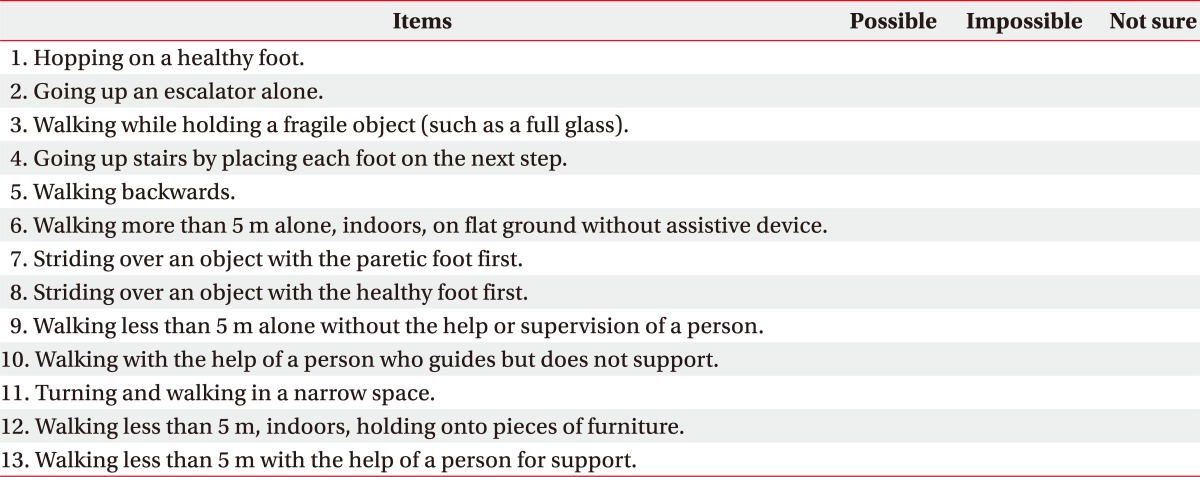
We received permission from Caty et al. [7], the original author, to undergo a Korean translation of the ABILOCO (Table 1). Two physiatrists translated the ABILOCO into the Korean language, and the translated version was back-translated into English by another two physiatrists fluent in English for a comparison with the original version. Items which did not match the original meaning or which could potentially have a different meaning were edited again, followed by a translation and back-translation for comparison. The final product was made into a questionnaire in order to educate the physiatrists participating in this study. The doctors were instructed to study the principles of each detailed item before participating in the study.
Study subjects (Appendix 1)
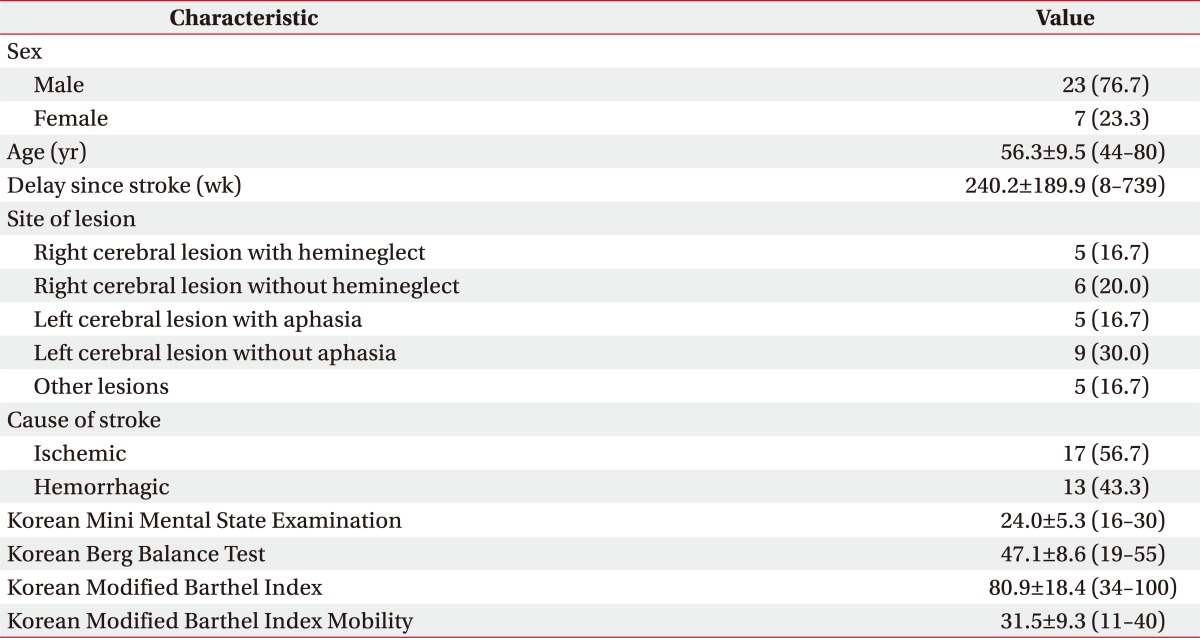
The subjects for this study consisted of 30 hemiplegic stroke patients (23 males and 7 females) who visited this hospital between March 1, 2011 and February 1, 2012 without changes in their walking ability or manual muscle test (MMT) for at least 1 week to 2 months after the stroke. The age of the subjects ranged from 46 to 80 years, with a mean age of 56.3 years. For the location of the lesions, 11 patients had lesions in the right cerebral hemisphere, 14 patients had lesions in the left cerebral hemisphere, and 5 patients had lesions elsewhere in the brain. The mean period after the lesion formation was 240.2 weeks. Thirteen cases were caused by cerebral hemorrhage and 17 cases were caused by cerebral ischemia. The mean values of the MMSE, K-BBS, K-MBI, and K-MBIM are presented in Table 2.
The exclusion criteria included patients who could not complete the questionnaires or follow instructions due to cognitive disability or language disabilities (Glasgow Coma Scale of 7 or less, inability to follow 3-step instructions, inability to read, inconsistent 'yes' and 'no' answers), patients with orthopedic disabilities or neurological disabilities other than stroke, immobile patients who are bedridden or who can only move in a wheelchair, and patients with deteriorating walking ability due to the relapse of stroke or due to fractures during the research period. Patients whose walking abilities had recovered to normal levels and who had no walking disabilities had been excluded in the original study [7]. Before the study, the objectives and the methods of the study were explained to patients and written informed consent was obtained. This study was approved by the board of ethical committees of our institution.
Methods
All 30 patients were assessed twice at one week interval. The first assessment was conducted at least 1 week after the onset at a point where there was no changes in muscle strength or walking ability. A physiatrist evaluated the medical history and other clinical data related to stroke for each patient and conducted physical and neurological examinations. K-MMSE was used to assess the cognitive ability of the patients, while the K-BBS and K-MBI were used to assess the walking ability and balance in daily life. From the K-MBI, item number 5, 'walking up the stairs', number 9 'walking', and number 11 'moving into a chair/bed' were used to create the K-MBIM score, this index was recorded for study purposes.
To assess the walking ability of patients, a physiatrist asked 13 items from the K-ABILOCO during an interview, such as asking whether the patient was either 'able' or 'unable' to conduct the relevant movements. If a patient answered that they were 'unable' to do a particular movement because they have never tried the particular task, the answer was changed to 'not sure'. After this, the physiatrist asked the patients to conduct each of the tasks of the K-ABILOCO under observation in order to confirm their ability to perform each task. To check the intertest consistency of the test, a second assessment was conducted after 1 week. The assessment method was the same as the first assessment; however, to prevent the learning effect, a different combination of questions using K-ABILOCO was used. During the second assessment, the patients were video-recorded while completing the tasks and the video recordings were viewed by a blinded third party physiatrist (who was not informed of the neurological or walking abilities of the patients). The third party physiatrist then assessed these patients using the K-ABILOCO for comparison with the second assessment conducted by the same doctor who conducted the first assessment of the patients. The raw data for each item was calculated using the Website, provided by the original authors of ABILOCO, and the calculated value was analyzed further using the Rasch analysis method [14] in order to produce a final log value.
Statistical analyses
Statistical analyses were conducted using the MedCalc ver. 12.1.4.0 (MedCalc Software, Ostend, Belgium). Because the recorded ABILOCO value was converted to a continuous variable, a logit value, the intraclass correlation coefficient (ICC) was also calculated to confirm the validity of the test-retest method. To test the validity of the test-retest method, the ICC was calculated between the first and second visits in the patient and the physiatrist groups. To test the inter-rater validity, the ICC value was calculated between patients and physiatrists in the first visit; between patients and physiatrists in the second visit; between the observer and patients in the second visit; and between the observer and physiatrists in the second visit. Since the category values of the intra- and inter-rater consistency are discontinuous variables, it was analyzed by a weighted kappa value. The consistency between each class was defined as poor when the kappa value was 0.20 or less; fair when the kappa value was between 0.21 and 0.40; moderate when the kappa value was between 0.41 and 0.60; substantial when the kappa value was between 0.61 and 0.80; and very good when the kappa value was 0.80 or greater [15]. The correlation between the K-ABILOCO total score and patient age, K-MMSE score, K-BBS score, K-MBI score, and K-MBIM score was calculated using the Pearson correlation coefficient (r). p-values of 0.05 or less were defined as having statistical significance in all statistical analyses.
RESULTS
Translation of the questionnaire
The original ABILOCO questionnaire was translated into the Korean language and back-translated to English for a comparison with the original text. During this translation and back-translation process, a few items of the questionnaire were found to have their meaning altered. For example, the phrase 'each foot' in question 4, 'going up stairs putting each foot on the next step'; question 7, 'striding over an object with the paretic foot first'; the word 'object' in question 8, 'striding over an object with the healthy foot first'; the word 'guide' in question 10, 'walking with the help of a person who guides but does not support'; were found to show variability between translators and were thus translated and back-translated again.
The reproducibility and validity of the K-ABILOCO
The total log K-ABILOCO score calculated from the first and second visits showed high ICC values of 0.81 in the test-retest in the patient group, and 0.91 in the physiatrist group. The log score of the K-ABILOCO showed high inter-rater correlation values of 0.76 in the first visit and 0.84 in the second visit between the patient and the physiatrist groups. Lastly, there was a high intraclass correlation between the third party physiatrist and patients (ICC=0.87) and between the physiatrists (ICC=0.95) in the second visit based on the video recordings (Fig. 1).
The intra-rater validity for each item of the questionnaire
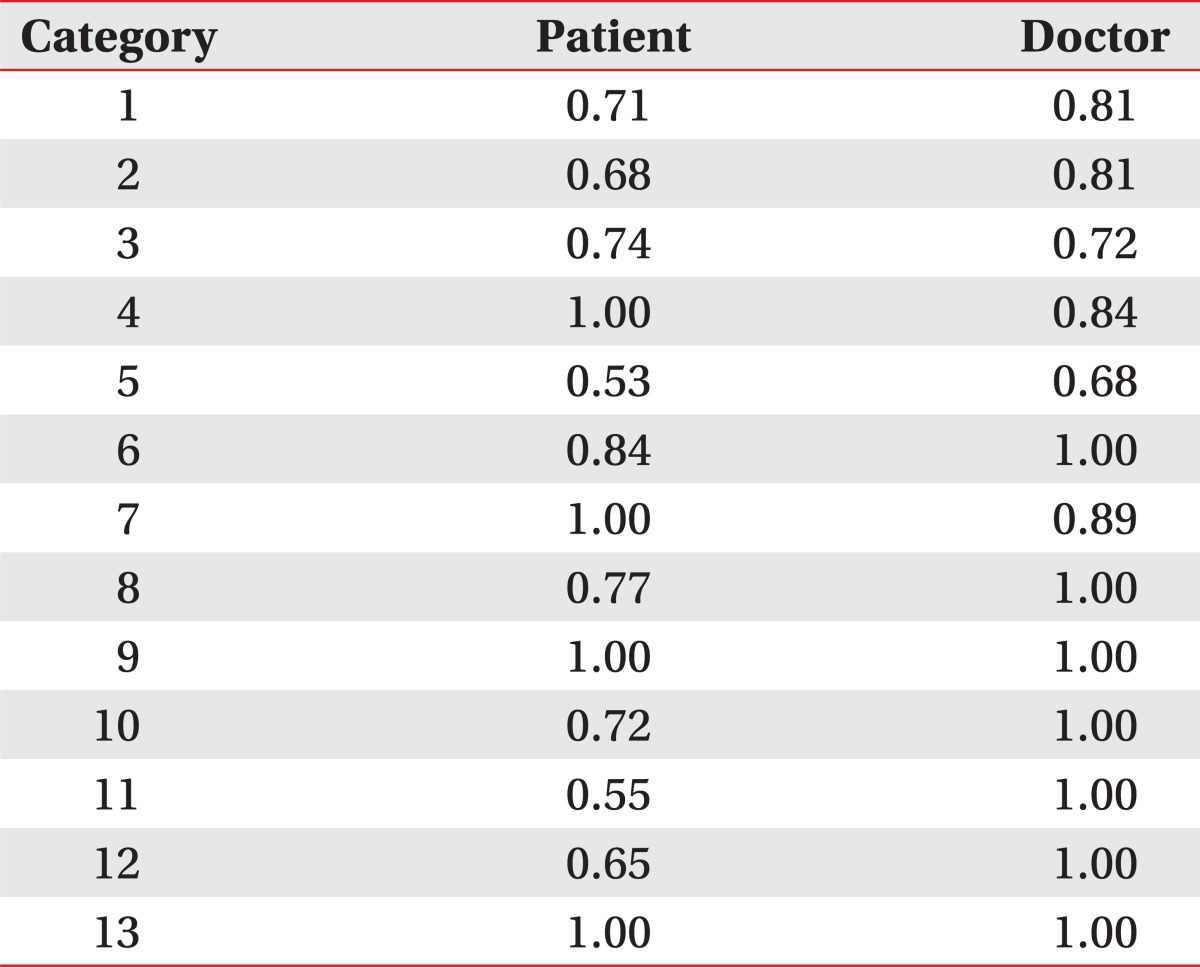
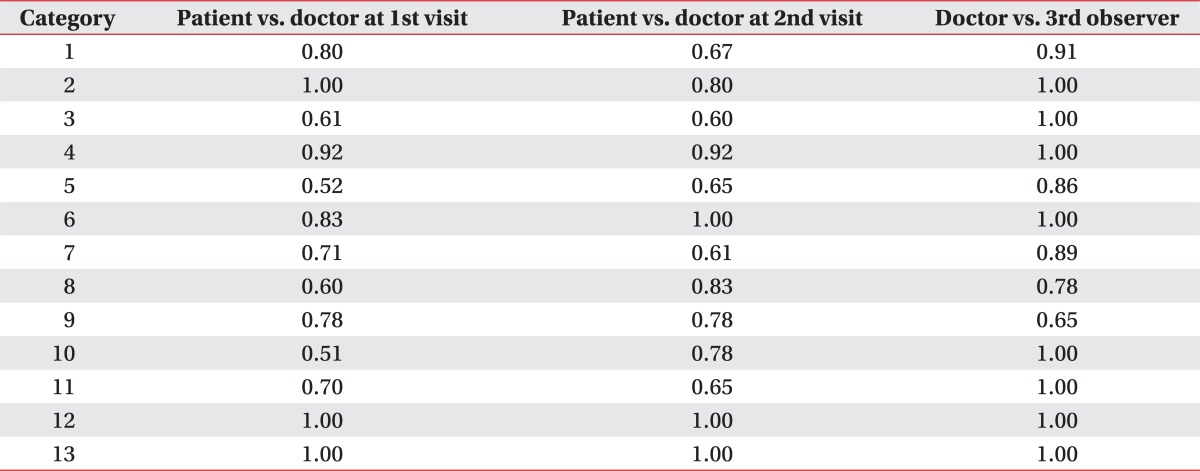
The consistency between each item of the questionnaire for the two visits presented a substantial consistency (weighted kappa=0.68-1.00) when the physiatrist assessed the patients, and a substantial consistency (weighted kappa=0.65-1.00) for most items when the patients completed the questionnaire on their own (Table 3). However, the intra-rater consistency was moderate (weighted kappa=0.53-0.55), for items 5 'can walk backwards' and 11 'can walk and rotate in a small space' in the patient group (Table 3).
The inter-rater validity for each item
The inter-rater consistency of the patients and the physiatrists for each item resulted in weighted kappa scores of 0.61 for the first visit and 0.60-1.00 for the second visit, showing a substantial level of consistency. The only exceptions were questions 5 'can walk backwards' (weighted kappa=0.52) and 10 'walking with the help of a person who guides but does not support' (weighted kappa=0.51) (Table 4). However, although items 5 and 10 showed a lower inter-rater consistency (moderate) compared to other items in the first visit, it showed a similar inter-rater consistency to other items in the second visit. In the assessment of the video recordings, most items in the second visit by patients and third party physiatrist resulted in inter-rater consistency of substantial levels (weighted kappa=0.65-1.00) (Table 4).
The correlation between age, K-MMSE, K-BBS, K-MBI, and K-MBIM
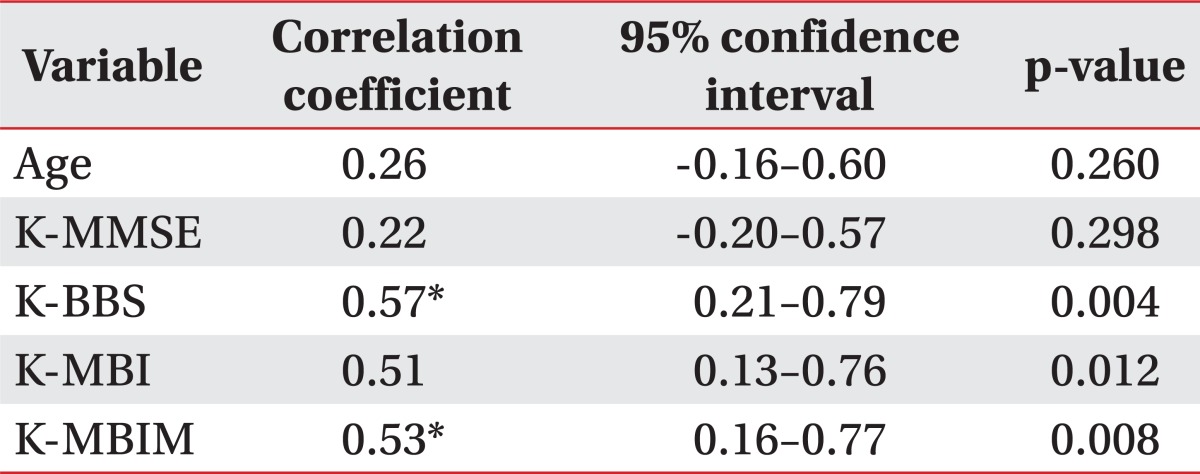
The total ABILOCO score and the K-BBS, K-MBI, and K-MBIM scores showed a statistically significant correlation (r=0.57, p=0.004; r=0.51, p=0.012; and r=0.53, p=0.008, respectively); however, there was no statistically significant correlation between age and K-MMSE scores (Table 5).
DISCUSSION
The aim of this study was to produce a standardized K-ABILOCO and to assess its reproducibility. In order to perform this goal, 30 hemiplegic stroke patients were assessed using the K-ABILOCO during the two assessments. The results showed a high intra- and inter-rater correlation, suggesting high reproducibility. Although the K-ABILOCO was of a questionnaire form, the intraand inter-rater consistency for each item in the questionnaire was high overall. This suggests that it allows a fairly accurate assessment of the walking ability of the patient without an assessment by a physiatrist. To confirm that the cognitive ability of patients does not affect the K-ABILOCO assessment, its correlation with the K-MMSE scores was checked. The results showed a non-significant correlation between the K-MMSE score and the K-ABILOCO score, meaning that the K-ABILOCO can be used in patients who are capable of basic communication even if their cognitive function is outside the normal range. Through this study, we have shown that the assessment of walking ability of hemiplegic stroke patients using the K-ABILOCO has a high reproducibility rate and can be a useful tool to assess patient walking ability in a clinical setting.
The results from this study are similar to those published in 2009 by the original authors of the ABILOCO regarding its reproducibility [10]. Assessment of the intraclass correlation resulted in a value of 0.81 in the patient group and 0.91 in the physiatrist group. These were high values similar to those published by the original authors (0.77 and 0.89, respectively). The intraclass correlation between patients and the observer, and that between physiatrists and the observer were 0.87 and 0.95, respectively, compared to 0.69 and 0.87 reported by the original authors. These results suggest that the standardization and translation of the K-ABILOCO was accurate.
In contrast to the original study, this study also evaluated the intraclass validity. For the validity of each item and the intra-rater consistency, questions 5 'can walk backwards' and 11 'can walk and rotate in a small space' resulted in a moderate level of consistency, which was lower than that of the other items in the questionnaire. The reason for this lower consistency is believed to be due to patients replying 'unable' or 'not sure' for these two questions in the first visit due to a lack of attempt during rehabilitation, or limited attempts in daily life, or due to anxiety that one cannot perform the movement due to lack of practice; whereas in the second visit, they were able to perform these movements in the second assessment. The inter-rater consistency for each item resulted in a lower consistency (moderate level) for questions 5 'can walk backwards' and 10 'walking with the help of a person who guides but does not support'. Both of these questions had a high rate of response for 'unable' and 'not sure', the reason for which was explained above. Although the patients had answered negatively, they were subsequently found to be able to complete the tasks under the instruction of a physiatrist and were thus noted to be able to perform the tasks, causing a discrepancy between the first and the second assessments. However, in accordance to the criteria set by Fleiss et al. [16], a weighted kappa value between 0.40 and 0.75 was considered to be 'fair to moderate' and therefore, this weighted kappa value shows some consistency, suggesting that the test is suitable for use in a clinical setting. Considering these factors, it can be seen that K-ABILOCO had high consistency values for most of the questions; however, care should be taken in interpreting the results of a few questions; e.g., question 5. To correct for this, it may be necessary to include general walking and backward walking in the rehabilitation program prior to conducting the assessment so that patients can have a prior experience in conducting the stated tasks.
All K-BBS, K-MBI, and K-MBIM were shown to have a correlation with the K-ABILOCO score. This proves the association between the K-ABILOCO and the tools used in clinical rehabilitation medicine in Korea for the assessment of mobility. Therefore, the above mentioned assessment tools can be used to complement each other. The K-ABILOCO is a marker of the level of difficulty in walking, while K-BBS is useful for the assessment of the ability to maintain a stationary posture and make changes in the movements [12]. On the other hand, K-MBI and K-MBIM include items that address the movement into chairs/beds and walking using walkers [13] unlike the other mentioned tools. The combined use of these tools will aid in a more accurate assessment of the mobility of patients.
The ABILOCO has several advantages over other tools used for the assessment of walking ability. It is a cost-effective and efficient tool that is easy to use. It assesses various movements that are required for daily activities; hence, it can be said that this tool is more practical compared to other available tools of its type. FWC was developed for the assessment of outpatients [3], while FAC was used to assess inpatients with relatively low mobility in a validity study, implying that it cannot be generalized to all patients with stroke. A limitation with these two tools is that they show a ceiling effect [7], meaning that they are less useful to evaluate the improvement level in patients once they have reached a certain point of recovery. The value calculated using ABILOCO questionnaire can be converted to a logit value, which makes it useful for statistical analyses of clinical studies involving hemiplegic stroke patients. It also consists of 10 different forms of randomly ordered questions and difficulties in order to prevent the learning effect [7]. A limitation with this tool is that for question 2, 'can use the escalators alone', the patient must be evaluated using a pre-recorded video clip if there is no escalator available in the assessment room.
Another limitation of this study is the uneven gender distribution of the subjects. According to the original authors, the ABILOCO score is not correlated to the gender of the patient, so it seems that the tool can be used without any differences in gender in the clinical setting. The original authors repeated the test after 2 weeks in order to prevent the patients from recalling the contents of the first assessment [10]. In our study, we assessed the patients again after 1 week as per the study by Green et al. [17]. The original study was conducted in patients who were at least 3 months from the onset of a stroke [10], while this study included patients at 2 months post-onset of a stroke, which means that patients were relatively in subacute stages of the condition. This means that it was not possible to completely rule out the possibility that the changes in the environment or the condition of the patient between the test periods could affect the test results, which is why the second assessment was conducted 1 week after the first one. A limitation with this is that the patients could possibly recall the contents of the first assessment. To address this issue, we used a different questionnaire with different ordering of the questions in the second assessment to minimize the learning effect. Another limitation of this study is that the correlation between K-ABILOCO and FWC, FAC, and 10MWT were not tested, while these three tools were used in the original study to compare with those of the ABILOCO [7]. This is because the main aim of this study was to translate a K-ABILOCO and we believed that its correlation with K-BBS, K-MBI, and K-MBIM, which are more commonly used in rehabilitation medicine in Korea, would have more significance. In this study, we analyzed the reproducibility of the standardization of the K-ABILOCO; however, the validity with other markers was not analyzed. However, this analysis was already accomplished by the original authors of ABILOCO; therefore, it seems that such additional analyses will be needed for K-ABILOCO.
In conclusion, the results of this study showed that K-ABILOCO produced high intra- and inter-rater reproducibility similar to the original ABILOCO. It is expected that K-ABILOCO will prove to be a useful marker in evaluating walking ability and in planning the rehabilitation treatment of stroke patients in Korea.

 XML Download
XML Download