

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Osteoporotic vertebral compression fractures (OVCFs) is the most common disease among bone fractures caused by osteoporosis. The volume and contents of the bony tissue decrease and the vertebral body is easily broken by a weak impact during daily living activities [1]. Due to an increase in the elderly population, OVCFs have been gradually increasing. Although various treatments have been conducted to treat OVCFs, a surgical treatment is difficult to conduct as most patients are elderly and have a state with high medical co-morbidities. In addition, a spinal fusion with instrumentation is required in the case of the surgical treatment, it is difficult to achieve its fixation effect due to osteoporosis. Furthermore, as the surgical treatment has disadvantages such as longer anesthesia, high risks of postoperative complications and relatively low success rate of bone union by bone graft, conservative treatment (analgesic treatment, orthosis use, and physical therapy) have been alternatively conduced [2].
In the recent days, a less extensive and minimally invasive surgical procedure (percutaneous vertebroplasty and kyphoplasty), which not only allows pain reduction but also a safer cement augmentation and achieve the stability of the vertebral body, is preferred [3]. When this treatment was conducted, it was reported that pain reduction was achieved and mobility was improved in approximately 90% of the patients who underwent percutaneous vertebroplasty within 24 hours after the surgery [4]. In the case of persistent axial back pain after vertebroplasty, however, it is not attributable to the vertebral body but to other reasons. In general, the vertebral body is a cause for pain in patients with acute compression fracture. As the structural deformity of the vertebra after fracture imposes more weight load on the facet joint, arthritis following fracture could be an important reason for pain in patients with vertebral fracture [5]. In addition, old compression fracture is incidentally observed in elderly patients with back pain in some cases. In this case, pain is also likely to be attributable to other factors such as facet joint, muscle, and tendon rather than the vertebral body [6]. It was reported that steroid injection at the facet joint was effective in the treatment of chronic facet joint pain in patients with thoracolumbar or lumbar compression fracture who underwent conservative treatment or vertebroplasty [5].
This study was conducted on patients who were followed-up for one year after medial branch block among those who had chronic facet joint pain following OVCFs. The correlation of the effect of medial branch block with patient satisfaction and radiological status such as local vertebral curvature and the sagittal alignment of the spine that might affect the treatment result with the clinical features of the patients were investigated.
Go to : 
MATERIALS AND METHODS
Subjects
This study was conducted on patients who visited the department of rehabilitation of Sanggye Paik Hospital due to thoracolumbar or lumbar axial pain, bilateral or unilateral hip pain, and referred pain of the low extremities from January 2009 to November 2011. Among the total 251 patients, those who had persistent pain 3 months after the surgery or who were diagnosed with old compression fracture located at the pain site by lumbar computed tomography, magnetic resonance imging, and radiology or who had osteoporosis (T=-2.5 or lower) were selected as the subjects. Among the subjects, 89 patients, except for those who had radiculopathy, spinal cord injury, cauda equina syndrome, or multiple facet joint pain caused by multiple facture, were selected, of whom the study was conducted on the 53 subjects who were diagnosed with thoracolumbar or lumbar facet joint pain as they had Verbal Numeric Rating Scale (VNS) that decreased 80% or more after diagnostic medial branch block conducted on the sites of vertebral segment of vertebroplasty or old compression fracture, and who underwent therapeutic medial branch block and then followed-up for one year or longer.
Methods
Thoracolumbar or lumbar medial branch block
All the medial branch blocks were performed utilizing a posterior approach with the patient in the prone position with a pillow under the chest.
For 1-4 medial branch block, in which the outline of the "scotty dog" is clearly evident, a puncture point is selected by placing the tip of the needle on the skin directly in line, along the X-ray beam, with the target point behind the "eye" of the dog [7,8]. Insertion is terminated once the tip of the needle strikes bone and this should be on the neck of the superior articular process, superodorsal to the silhouette of the transverse process [8]. Correct placement is confirmed by obtaining a posterior-anterior view, in this view the tip of the needle should be at least opposite the lateral margin of the superior articular process. Once the needle is in correct position, the bevel should be directed caudally so as to avoid spread of the injectate to the intervertebral foramen [7,8]. This having been done, 0.2 mL of the non-ionic contrast medium Omnipaque300 (GE Healthcare, Carrigtohill, Ireland) can be injected to test that venous uptake dose not occur and if it does, the needle must be re-adjusted by 1-2 mm and the test repeated [8]. If there is no venous uptake, 1% lidocaine HCL 0.5 mL is injected onto the target nerve.
For L5 dorsal ramus block, the protocol is the same as for block at higher levels. The difference that obtain are that the target nerve is not the medial branch but the dorsal ramus itself and that target point is the junction of the ala of the sacrum with superior articular process of the sacrum [7-10].
For blocks of the T11 and T12 medial branches, the technique is the same as that for lumbar medial branch blocks (Fig. 1) [8]. A seemingly minor anatomical point is of critical importance for accurately recording and communicating thoracic medial branch blocks. The segmental number of the nerve is the same as the number of the vertebral from under which its parent dorsal ramus and spinal nerve issues. When medial branches subsequently cross a transverse process, it will be the transverse process of the vertebral with the next segmental number, thus, the Tm medial branch will cross the T(m+1) transverse process. Each medial branch innervates the zygapophysial joint of its own segment ant the one below. Thus the Tm medial branch innervates the Tm-T(m+1) joint and the T(m+1)-T(m+2) joint. Conversely, the Tm-T(m+1) joint is innervated by the T(m+1) and Tm medial branches [8].
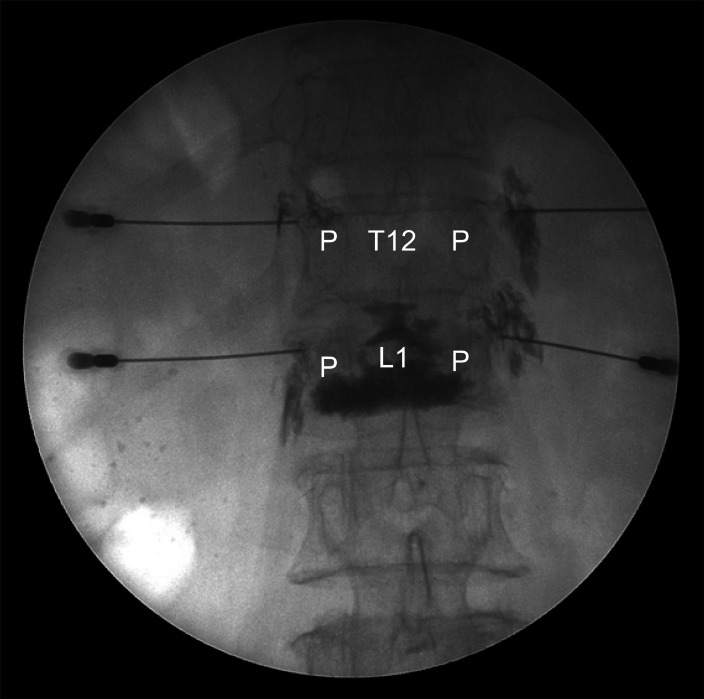 | Fig. 1T11, T12 medial branch block in patient with L1 compression fracture (vertebroplasty state). The T12-L1 joint is the medial branch of the T11 and T12 dorsal ramus. Anteroposterior radiography of contrast medium injected onto the target point for T11 and T12 medial branch blocks. The needle tip point to the contrast medium at the site for T11 and T12 medial branch blocks on the T12 and L1 superior articular processes. P, pedicle.
|
Repeated medial branch block was indicated if the VNS measured before injection increased 50% or more. As the frequency of therapeutic medial branch block using steroid and local anesthetic agent is allowed up to 6 times for one year based on the results of previous studies and the treatment guideline [11-13]. The conduct frequency was limited to up to 6 times in this study.
Outcome assessment
VNS was measured before the treatment, and 2 weeks, 3 months, and 12 months after the treatment to assess the effect of injection treatment. The VNS was obtained at 2 weeks and 12 weeks after the procedures to grade the treatment effects. When using VNS, the patients were asked to rate their pain on a scale from 0 to 10: 0 and 10 represented "no pain" and "the worst pain possible," respectively, in whole number with 11 integers including zero. A medical investigator marked the scale for the patients incapable of marking for themselves by directing and slowly moving from 0 to 10 on a VNS scale board. The patients nodded at the appropriate score.
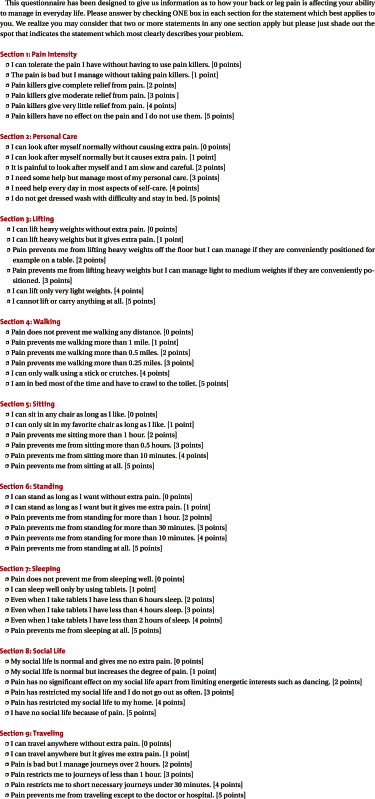
The Korean version of Oswestry Disability Index (ODI) (Appendix 1), which was standardized to have 9 items by Kim et al. [14], was used for the severity of physical disability. Each item has a 6-point scale ranging from 0 to 5 points. Back pain is severer in proportion to the score. The total score is calculated by summing the scores of the 9 items, and expressed as percentage (%). There are 4 subgroups mild (0%-20%), moderate (21%-40%), severe (41%-60%), and highly severe impairment (60% or more) according to the percentage of the score [15].
Patient satisfaction levels were measured with a 5-point scale (<0, no effect at all; 1, bad; 2, fair; 3, good; ≥4, excellent) at 12 weeks. 'Excellent' was defined as satisfied with the treatment result as expected; 'good' was defined as, not as satisfied as expected but willing to try this treatment next time when pain redevelops; 'fair' was defined as had some effect but not enough to choose the same treatment next time when pain redevelops; and 'bad' was defined as the same effect with prior treatment or worse [16].
Correlation of the treatment effect with various factors
Successful treatment occurred when patients obtained significant pain relief (as measured by >40% improvement in the VNS score and >20% improvement in the ODI score) and reported a patient satisfaction score of 3 or 4 points at 12 weeks after the injections [17-19].
Body mass index (kg/m2) was 7 measured using the age, height, and weight of the patients. The previous history of systemic diseases such as diabetes, hypertension, and cardiac diseases were reviewed. As for the presence/absence and status of osteoporosis, segments with old osteoporotic compression fracture between T12 and L5 or site that received vertebroplasty was excluded, and the bone density and t-score were obtained based on the mean bone density of the cancellous bone and cortical bone of the four region of the spinal segment, respectively, using peripheral quantitative computed tomography (p-QCT; Siemens, Erlangen, Germany).
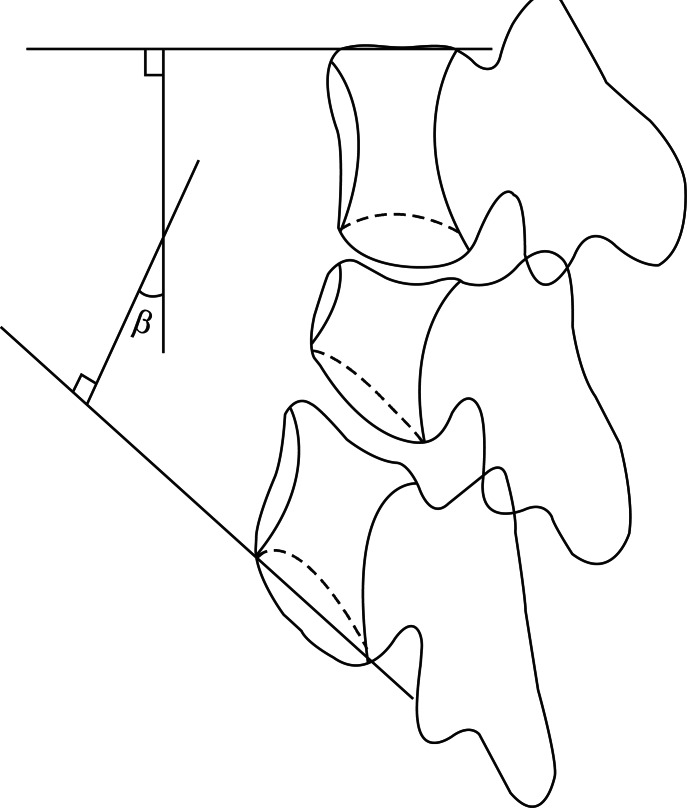
As for radiological examination before medial branch block, the anteroposterior and lateral region of standing full spine and standing lateral bending views of the lumbar spine including the hip joint and cervical vertebra were photographed using a 14×36 inch cassette. The sagittal kyphotic angle of local segment was obtained by measuring the acute angle between the upper vertebral upper margin and lower vertebral lower margin of the collapsed vertebral body (Fig. 2), the sagittal plane alignment was obtained by measuring the distance between C7 plumb line and anterior margin of S1. The compression fracture rate was calculated using the following equation: height loss=estimated prefracture height-pretreatment fractured height. The estimated prefracture height was applied by obtaining the mean value after summing the upper and lower vertebral body height of the adjacent fractured vertebral body [20]. All the results of radiological analysis were obtained by measuring three times by independent measurers and calculating the mean values. Subsequently, the correlation of the patient's status, radiologic parameters before injection, and the treatment effect was investigated.
Statistical analyses
At each time point, the VNS and ODI scores were compared using repeated measures analysis of variance (ANOVA), and Bonferroni corrections were utilized for post hoc comparisons. The treatment outcome and variables (patient's age, sex, duration of the disease, cause, radiologic finding) were compared with logistic regression analyses. All analyses were performed with SAS ver. 4.1 (SAS Institute Inc., Cary, NC, USA) with a significance level of p<0.05.
Go to :
RESULTS
General characteristics of the patients
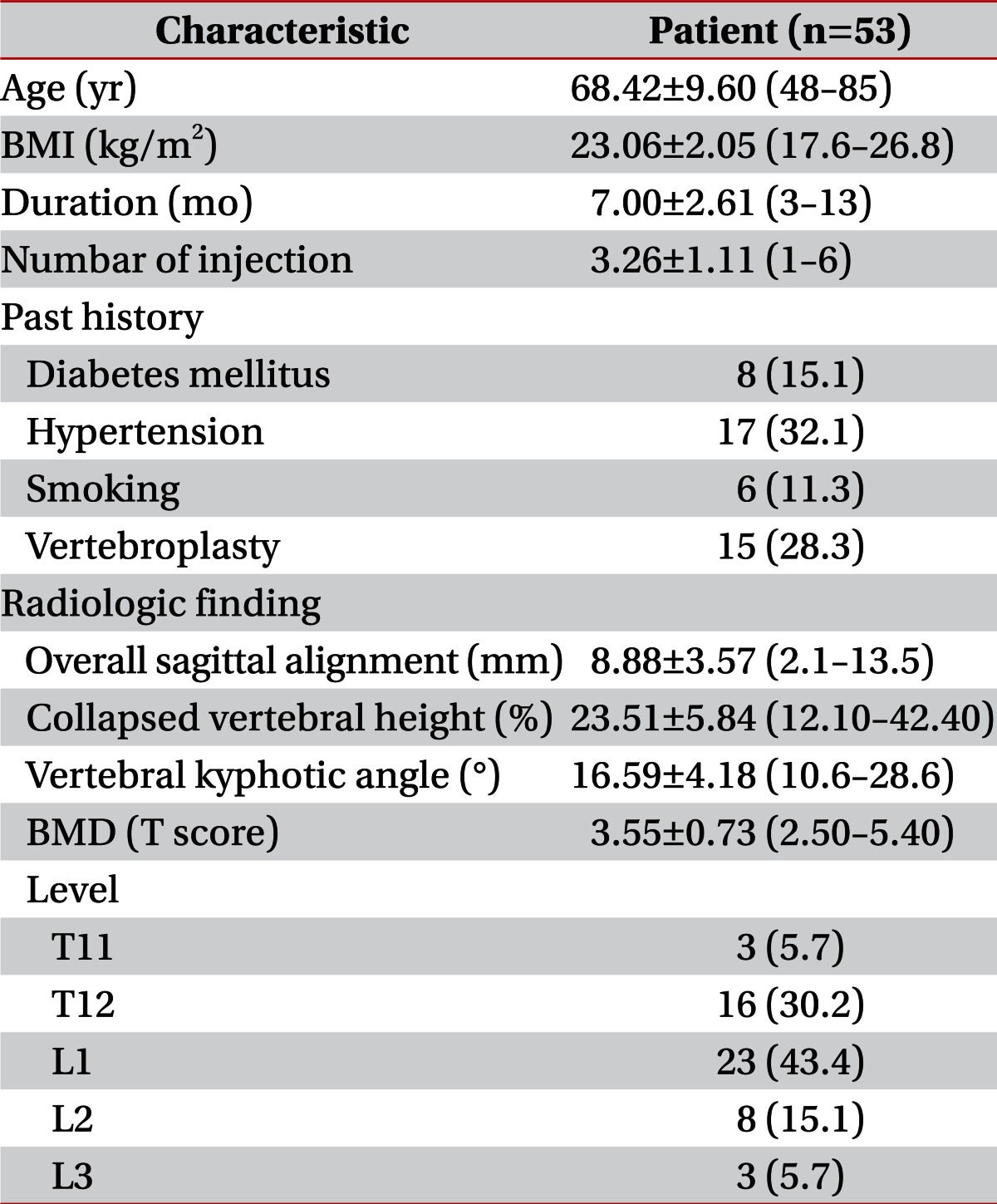
A total of 53 subjects had the mean age of 68 years (range, 48 to 85 years), and BMI of 23.06 kg/m2 (range, 17.6 to 26.8 kg/m2). All the subjects were female patients and their mean pain duration was 7 months (range, 3 to 13 months). The radiologic parameters included mean compression rate 23.51% (range, 12.10% to 42.40%), kyphotic angle 16.59° (range, 10.6° to 28.6°), and sagittal alignment 8.88 cm (range, 2.1 to 13.5 cm) before the treatment (Table 1).
Effect of medial branch block
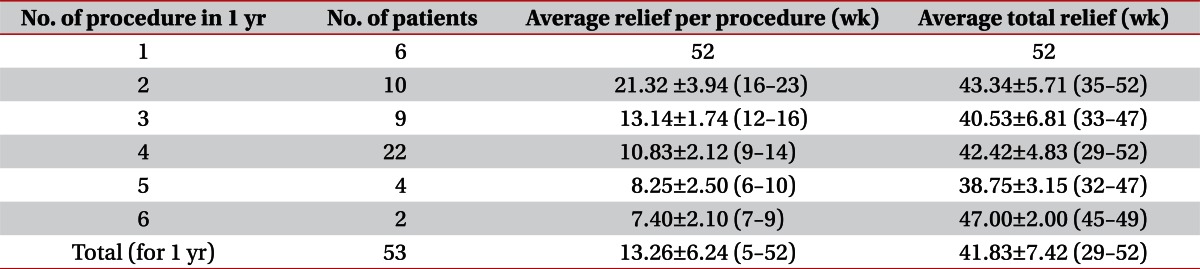
The mean frequency of medial branch block, average total relief over a period of 1 year, and average relief per procedure were 3.26, 41.83, and 13.26 weeks, respectively. The mean duration of average total relief over a period of 1 year, and average relief per procedure of each group according to the frequency of medial branch block are presented in Table 2.
The VNS scores and ODI scores were significantly reduced immediately after the treatment and remained reduced at 2 weeks, 3 months, and 12 months after the injections (Table 3).

The treatment effect was defined successful when the VNS and ODI increased 40% or more and ODI 20% or more, respectively, in the patients who had a patient satisfaction of 'gOdds ratioood' and 'excellent' in the 12-month follow-up. As a result, 100%, 81.1% (43 patients), and 78.9% (42 patients) of the patients showed the improved result 2 weeks, 3 months, and 12 months after the treatment.
Correlation between the treatment effects and variables
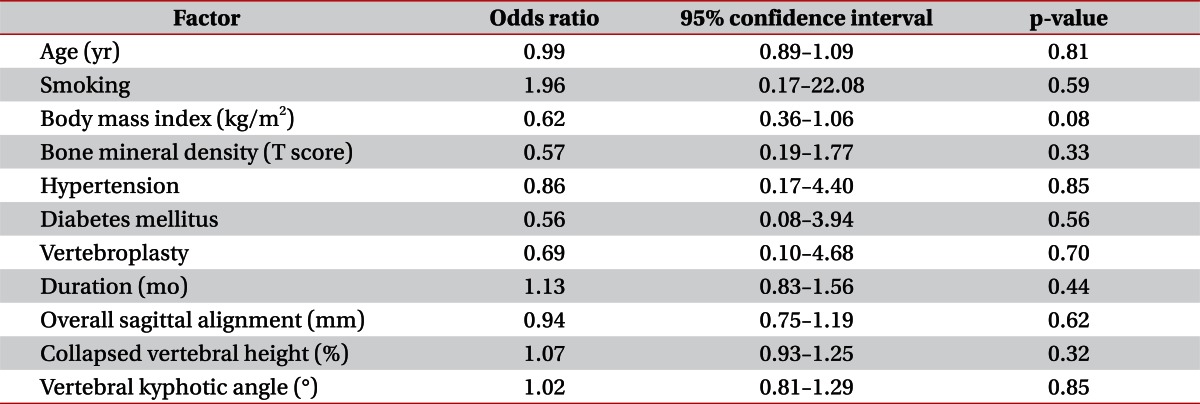
Successful treatment occurred when patients obtained significant pain relief (as measured by >40% improvement in the VNS score and >20% improvement in the ODI score) and reported a patient satisfaction score of 3 or 4 points at 12 weeks after the injections. Treatment success was unrelated to the disease duration, the age, sex of patients and radiologic finding (Table 4).
Complications
No major complication was observed during the treatment. Dizziness and transient muscle weakness were observed in six patients after injection treatment, but they were completely resolved when the patients were discharged. Hot flash was observed in 2 patients, but it was resolved 2 weeks later. No other complication occurred.
Go to :
DISCUSSION
The facet joint are true synovial joints with a joint space, hyaline cartilage surfaces, a synovial membrane, and a fibrous capsule. Lumbar facet joints are innervated with nociceptive fibers (pain-sensing nerves). As the nerve fibers, which contain the pain-mediator substance P, and calcitonin gene-related peptide, have been isolated in the joint capsules and degenerative facet joint subchondral bone, overload of this richly innervated capsule potentially causes pain transmitted by means of nociceptive nerves [21]. Facet joint syndrome is clinically present, and pain can be blocked by diagnostic block [21]. spinal fracture may cause pain at the upper and lower areas of fracture by vertebral body collapse, spinal instability, facet joint syndrome, nerve compression, and kyphosis after spinal surgery [5].
Although the biomechanical effect of lumbar thoracolumbar compression has not yet been completely elucidated, a previous study using cadaver reported that the anterior compression fracture of the vertebral body increased thoracolumbar bending moment and subsequently thoracolumbar kyphosis, thereby increasing stress in the posterior structure of the spine including facet joint. Kim et al. [22] reported that concurrent facet joint pain was observed in 88% of the patients due to body weight load caused by vertebral body compression fracture, and that dull pain with the unclear boundary along the rib and significant discomfort during wake up were observed even after vertebroplasty or kyphoplasty if medial branch block was not conducted.
Regarding the effect of medial branch block on facet joint pain, a double-blind randomized study, which was conducted by Manchikanti et al. [23], reported that 85% of patients with lumbar facet joint pain who received bupivacaine and steroid showed a pain relief of 50% or more and functional improvement of 40% or more in a one-year follow-up, and that pain relief was observed for 44-45 weeks/year in three or four times of injection treatments per year. The effect of steroids that was used for medial branch block against facet joint pain may be expressed as anti-inflammation, immunosuppression, anti-edema, and inhibition of neurotransmission in the C nerve fiber [24,25]. The use of a local anesthetic agent has long-term blocking effects achieved by suppression of nociceptive discharge, the blockade of sympathetic reflex arc, the blockade of axonal transport, the blockade of sensitization , and anti-inflammatory effects [26-30].
Georgy et al. [6] conducted a retrospective study and reported that of 144 patients who received vertebroplasty or sacroiliac joint surgery, 34 patients further underwent epidural steroid injection, facet arthritis injection, sacroiliac joint injection, trigger point injection due to persistent pain. They also reported that in addition to vertebral compression fracture, thoracolumbar pain was also caused by other spinal structures such as the disc, muscle, tendon, ligament, and facet joint [6]. Mitra et al. [5] reported that facet joints may be abnormally stressed due to the increasing thoracic flexion. In anterior compression fractures, which may serve as a secondary pain generator; intra-articular facet blocks may be an alternative to vertebroplasty. In this study, medial branch block was conducted on the patients who complained of persistent pain at the old compression fracture site or the patients with osteoporotic vertebral compression fractures (OVCFs) who complained of persistent pain after vertebroplasty. As a result, if the treatment effect was defined successful when the VNS and ODI increased 40% or more and ODI 20% or more, respectively, in the patients who had a patient satisfaction index of 'good' and 'excellent' in the 12-month follow-up, successful case was seen in 78.9% of the patient. In addition, The average procedures per year were 3.26 with an average relief per year of approximately 13.26 weeks per procedure and patients experiencing approximately 41, 83 weeks of relief during the period of 52 weeks with repeat blocks. Therefore medial branch blocks for OVCFs with chronic facet joint pain may be provide approximately 13.26 weeks of relief and requiring 3 to 4 episodes of treatment per year.
Until now, previous studies have reported that there are the correlation of the effect of conservative treatment or surgical treatment following vertebral compression fracture with various factors. Weinstein et al. [31] reported that pain was observed in 90% of 83 patients with thoracolumbar burst fracture who underwent conservative treatment, but it was insignificant, and that the pain severity was uncorrelated with the patient's age, gender, hospitalization duration, and duration of follow-up. Willen et al. [32] reported the mean kyphosis of 27° and 19.5° were formed after conservative treatment and surgical treatment, respectively, and that direct compression to the fractured site was correlated with pain in the case of a kyphosis formation of 30° or more, but no correlation of treatment methods such as surgical or conservative treatment with patient pain was found. In this study, for the assessment of the treatment effect, the successful treatment effect was defined as a case of decrease in pain index ≥40% and function index ≥20% and patient satisfaction of 'good' or 'excellent'. Thus, no correlation of the treatment outcomes with patient's age, disease history, bone density, and radiological parameters was found. In this study, the mean kyphotic angle was shown to be 16.59°, which was insignificant compared to the result of the study conducted by Willen et al. [32] this is likely to be associated with the uncorrelation of the treatment effect. Reid et al. [33] reported that in the case of kyphotic angle ≤35° in patients with thoracolumbar burst fracture without neurologic symptom, pain or working ability was satisfactorily improved and kyphosis did not increase.
Day and Kokan [34] reported that job change was required in approximately 67% of patients with the compression fracture rate ≥50%. Meanwhile, Aglietti et al. [35] reported that approximately 80% of patients who underwent conservative treatments returned to their previous job. In this study, the mean severity of compression fracture rate was shown to be 23.51%, and no case of 50% or more compression fracture rate was found. Thus, the patients were likely to have showed a good response to the conservative treatment, which showed no statistical correlation. In general, 50% or more compression fracture rate and kyphotic angle of 20° or more increase the possibility of burst fracture. In these cases, a surgical treatment rather than a conservative treatment is preferably required due to the high frequency of posterior column injury [36].
In this study, medial branch block was performed if pain was persistent following vertebroplasty. Kim et al. [22] reported that facet joint block was recommended to be conducted before vertebroplasty or kyphoplasty. Facet joint block before vertebroplasty or kyphoplasty had two major roles, one was to let patients lie down during the procedure under the local anesthesia and the other was to let the operator find out the exact level among the multiple fractures by elimination of radiating pain to the flank, abdomen, groin or buttock. A further study is required to investigate the effect of medial branch block on compression fracture with facet joint pain by comparing the treatment group that underwent facet joint block before vertebroplasty with the control group.
This study has a few limitations. First, single diagnostic block of the lumbar medical branch using a single drug was conducted due to situations such as temporal and financial limitation and outpatient. However, in the case of uncontrolled single diagnostic block, the risk of false positivity was reported to be 38%, which has a high possibility of not completely ruling out discogenic pain or muscle pain [37]. Thus, this study was conducted at a response rate of 80% to rule out the false positivity. Second, this was a retrospective study which had various bias that may affect the treatment effect. Thus, a further prospective controlled study using a placebo is required. Nonetheless, this study is meaningful in that this was the first study that investigated the effect of medical branch block on chronic facet joint pain of compression fracture on a large scale. Considering the aforementioned limitations, a further prospective double-blind controlled study is required.
In conclusion, the result of this retrospective study showed that medial branch block resulted in the pain relief and functional recovery of the patients with OVCFs who complained of chronic facet joint pain following vertebroplasty or conservative treatment. A further prospective double-blind randomized controlled study is required to validate the results of this study.
Go to :
 XML Download
XML Download