

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In order to assess swallowing difficulty a variety of examinations are available. The videofluoroscopic swallowing study (VFSS) is widely used as a standard examination to diagnose swallowing difficulty.1 VFSS consists of a lateral and an anterior-posterior view, and the lateral view is mainly used in order to judge the severity of swallowing difficulty and decide on a feeding formula, through the presence and degree of airway aspiration and penetration on the glottis. On the other hand, although the anterior-posterior view can evaluate an aspect of swallowing laterality, this method poses difficulties when assessing airway aspiration and penetration on the glottis, the most important consideration in swallowing difficulty. This is why in a considerable proportion of cases, AP view is often ruled out from a routine inspection.
A few studies have researched swallowing laterality, but the mechanism is unclear. An older study of swallowing laterality noted that a malfunction in the pharynx on one side results in food material passing through easily to the healthy side.2 Other studies which followed have reported the reverse.3 Also, a study by Seta et al.,4 had been conducted on normal population who did not have any symptoms of aspiration, reported that 42% had swallowing laterality. Thus, it is controversial whether swallowing laterality should even be defined as a malfunction of swallowing.
In a literature review in the studies concerning swallowing laterality as a disorder, there was only one analysis of swallowing laterality with Wallenberg syndrome. Particularly, research about the mechanism of swallowing laterality in hemiplegic patients who have suffered strokes and how it contributes to swallowing difficulty was nonexistent. These authors have seen not uncommon swallowing laterality when assessing swallowing difficulty in hemiplegic patients with strokes using VFSS, questioned whether it had a marked difference on the severity of swallowing difficulty such as the frequency and quantity of aspiration in the presence of swallowing laterality.
Hence, by inspecting the aspect of appearance of swallowing laterality and how this affected the severity or prognosis of swallowing difficulty in hemiplegic patients with strokes, this research was intended to clarify how swallowing laterality influenced swallowing difficulty.
Go to : 
MATERIALS AND METHODS
Participants
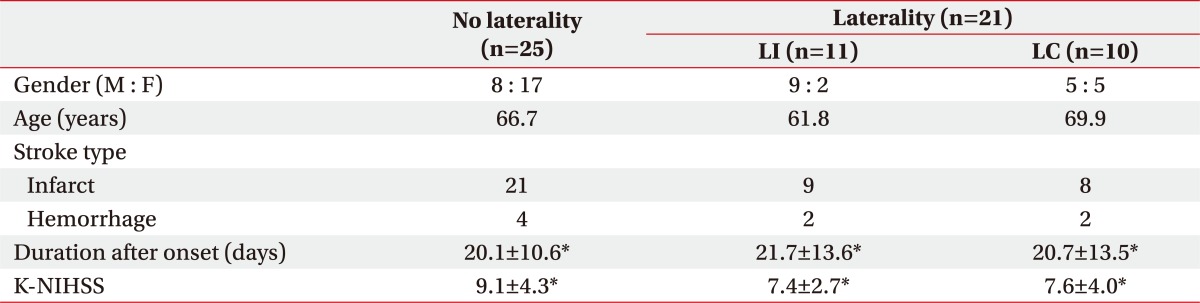
Forty-six patients (22 males and 24 females) were included who were admitted or transferred to the Department of Rehabilitation Medicine due to dysphagia with hemiplegia caused by their first stroke between March 2010 and April 2011. Their mean age was 67.5±13.1 years (ranged from 34 to 89 years) and the duration after stroke was 20.6±11.7 days (ranged from 7 to 47 days). Patients excluded were those who had unstable sitting balance in a wheelchair, or who were expected to be uncooperative due to cognitive impairment, and those with a neurologic deficit. Dysphagic patients with infratentorial lesion and without definite hemiplegia were also excluded. Of the 21 (45.7%) patients diagnosed with swallowing laterality in VFSS, 14 were male and 7 were female. Twenty-eight patients (13 males and 15 females), there was no evidence of aspiration. The remaining 18 patients (9 males and 9 females) and 1 patient who had severe penetration without aspiration reexamined 2 to 6 weeks later. The trial was performed under the approval of the Institutional Review Board for Clinical Studies.
Methods
Clinical symptoms prior to the VFSS that were checked included: confirmed lip and tongue movement, gag reflex, facial palsy, dysarthria and voice change. The subjects were then given a bedside physical examination to check for airway aspiration when swallowing; cough or choking.
As a thin liquid, barium sulfate liquid (Solotop Suspension 140) diluted with water into 70% liquid solution was used, and as a thick liquid, 200% liquid solution was used which was made from 140% barium sulfate liquid with additional barium sulfate powder.
The VFSS examination was performed as follows: the table used in general gastrointestinal fluoroscopy was raised vertically, and the patients, sitting on wheelchairs, were placed on the right side. In the lateral view they were given 5 cc of thick liquid and 5 cc of thin liquid to swallow 5 times each. Then in the anterior-posterior view, they were given 5 cc of thick liquid to swallow 3 times.
The evaluation after examination using video material recorded by a camcorder was conducted by two physicians from the Department of Rehabilitation Medicine using a Picture Motion Browser 2.0 (Sony, Tokyo, Japan) on the monitor of the gastrointestinal fluoroscopy device. In lateral view, it was analyzed for the degree of aspiration or penetration, and in anterior-posterior view, swallowing laterality.
For the evaluation of the degree of aspiration, the Final Version of the 8-Point Penetration-Aspiration Scale was used.5 It was the scale which measured from 1 to 8 in original work, but in this study it was modified from 0 to 7. The average value of swallowing the thin liquid and thick liquid 5 times was used to analyze the results. The follow-up revaluation progressed till no more change in the degree of airway aspiration had been detected. The difference between the first and the last examination was used to compare the extent of improvement.
For an appraisal of the degree of laterality, width difference of barium sulfate liquid flowing out of the pharyngoesophageal segment was used.4 When it showed double or more of that from the opposite width in the pharyngoesophageal segment more than twice on 3 times of swallowing, it was judged as having laterality. When there was laterality, the patients were divided as two groups according to whether the laterality corresponded with the hemiplegic side.
For the functional degree of swallowing difficulty, the functional dysphagia scale suggested by Han et al.1 was utilized. The revaluation continued until there was no more change in the degree of aspiration. The difference between the first and the last examination was used to show the extent of improvement.
To analyze the results, comparisons were made between groups; a group which did not have laterality (NL), a second group in which the laterality coincided with hemiplegia (LI), and the third group in which the laterality did not coincided with hemiplegia (LC). In the first examination, the degree and frequency of airway aspiration and the functional degree in swallowing difficulty between groups was compared. The degree of improvement was also compared between groups with the result of patients who had done re-inspection.
Statistical analysis
Statistical analysis was performed using SPSS 12.0 for Windows SPSS version 12.0K (SPSS Inc., Chicago, USA). For comparison of sex and laterality according to the hemiplegic side, chi-square test was used; for comparison of ages, duration after onset, Korean Version of National Institutes of Health Stroke Scale (K-NIHSS), Score of Final Version of 8-Point Penetration-Aspiration Scale (8-PPAS), Functional Dysphagia Scale Score (FDSS) and interval changes in the 8-PPAS, FDSS of three groups, one way ANOVA, and post-hoc Bonferroni test were used. Null hypotheses of no difference were rejected if p-values were less than 0.05.
Go to :
RESULTS
Swallowing laterality
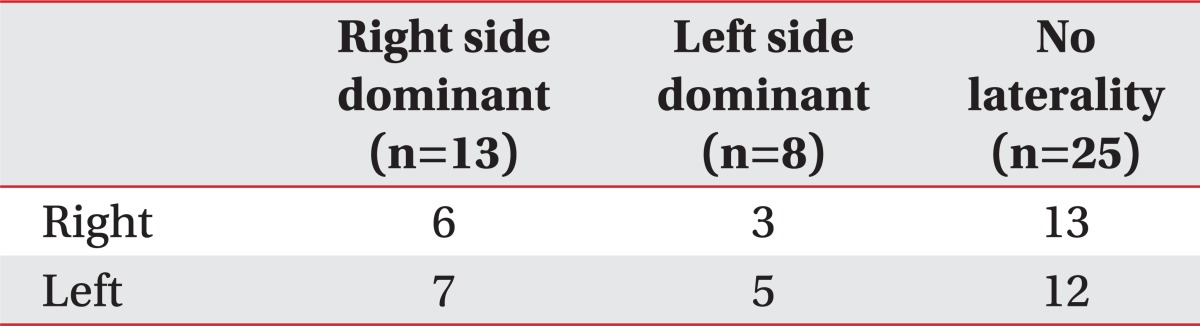
Laterality was observed in 21 (45.7%) patients, through the anterior-posterior view. Eleven (52.4%) patients out of 21 had swallowing laterality of the hemiplegic direction, and the remaining 10 (47.6%) had it in the opposite direction (Table 1). Classifying swallowing laterality according to hemiplegia laterality, swallowing laterality was not observed in half regardless of hemiplegia. When there was swallowing laterality, there was a tendency to occur to the right side with both right and left hemiplegia (Table 2).
Difference of frequency and degree of airway aspiration between groups
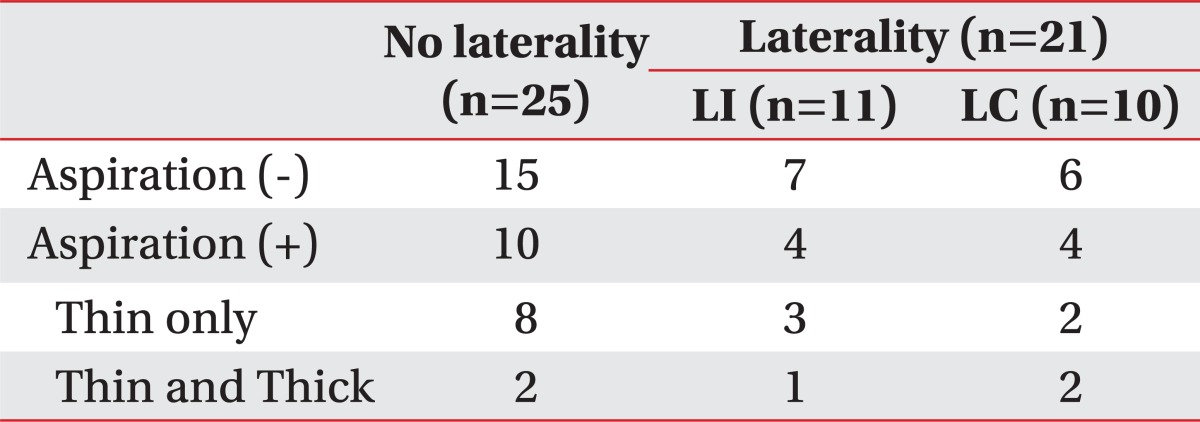
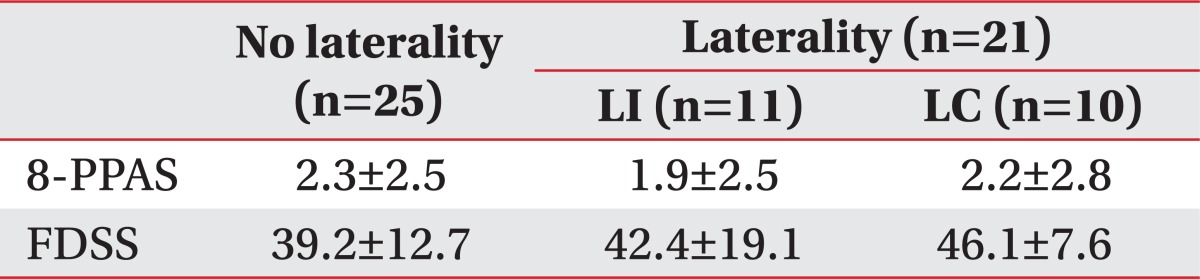
In the group without swallowing laterality, 11 (44.0%) patients from 25 had airway aspiration. In the group with swallowing laterality directed to the hemiplegic direction, 4 (36.4%) of 11 had airway aspiration. In the group with swallowing laterality towards the opposite direction of hemiplegic, 4 (40.0%) of 10 had airway aspiration. However, these differences were too small to distinguish statistically (Table 3). In the presence of aspiration, the frequency with which airway aspiration occurred on thin liquid was only 8 (72.7%) out of 11 patients when there was no laterality and 5 (62.5%) out of 8 patients when there was laterality but that was not a significant difference between groups (p>0.05) (Table 3). On the 8-Point Penetration-Aspiration Scale which evaluated degree of airway aspiration, the NL group averaged 2.3±2.5 points, the LI group averaged 1.9±2.5 points, and the LC group averaged 2.2±2.8. However, groups did not differ (Table 4).
Difference of functional level of swallowing difficulty between groups
With regards to the Functional Swallowing Difficulty Scale Point of hemiplegic patients, the NL group averaged 39.2±12.7 points, the LI group averaged 42.4±19.7 points, and the LC averaged 46.1±7.6. There was no significant difference between groups statistically (p>0.05) (Table 4).
Difference of improvement
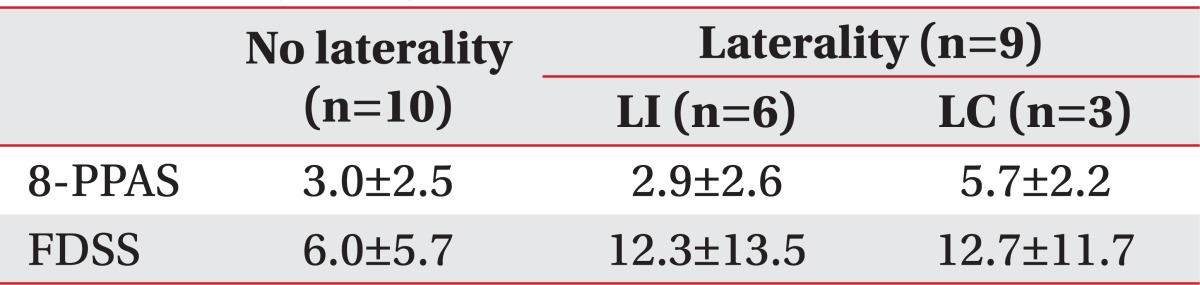
To 19 patients who had reexamination, the comparison between groups was made with regard to the improvement of airway aspiration and the change of functional degree in swallowing difficulty. VFSS was repeated in order to re-evaluate the 8-Point Penetration-Aspiration Scale and the Functional Swallowing Difficulty Scale Point of hemiplegic patients in the 10 patients from the NL group, the 6 patients from LI group, and the 3 patients from the LC group. On the 8-Point Penetration-Aspiration Scale, the NL group averaged 3.0±2.5 points, the LI group averaged 2.9±2.6 points, and the LC group averaged 5.7±2.2. There was no significant difference (p>0.05) (Table 5). Also, with regards to the change in the Functional Swallowing Difficulty Scale Point for hemiplegic patients, the NL group averaged 6.0±5.7 points, the LI group averaged 12.3±13.5 points, and the LC group averaged 12.7±11.7. Thus, the NL group had the lowest improvement, but they did not differ significantly from the other groups (p>0.05) (Table 5). Among the 19 patients, 5 patients showed a change in laterality; 4 of them showed resolution of laterality but only 1 patient had changed in laterality. However, 5 patients improved in the presence of airway penetration or aspiration.
Go to :
DISCUSSION
The mechanism of swallowing laterality is unclear. Studies of swallowing laterality are mostly aimed at people who do not have swallowing difficulty, so a study which analyses swallowing laterality as a disease faces an immaterial condition. In the research by Logemann et al.2 on 6 individuals without health problems, 2 had left laterality and 4 did not have it. Moreover, Seta et al.,4 studying 167 individuals without health problems, found that 7% of them had right laterality and 35% of them had left laterality, but 58% of them did not have laterality. Mosier et al.6 reported that the cerebral cortex's activity of the left hemisphere during swallowing was more dominant than the right hemisphere, using the functional MRI. Then, Seta et al.4 suggested, citing the results of the research performed by Mosier et al.6 that the existence of the dominant and non-dominant cerebral hemisphere could be applied in the swallowing function. Mikushi et al.3 proposed the mechanism of the swallowing laterality based on the research about swallowing laterality in Wallenberg syndrome. First, because of the discordance of cricopharyngeal muscles, disability in the opening of the pharynx occurred on the lesion side and, as a consequence, food material passed through the pharynx of the healthy side, resulting in laterality. Second, one side of the pharynx became narrower because of neurogenic atrophy of the cricopharyngeal muscles, causing food material to pass through the pharynx on the healthy side. As a result, laterality developed. Third, unlike the previous two mechanisms, it may be that food material passed through the affected side because it had less resistance than the healthy side due to flaccid palsy on one side of the cricopharyngeal muscles.
This is the first study to our knowledge which has researched the swallowing laterality of hemiplegic patient with swallowing difficulty caused by stroke. We found the direction of hemiplegia was not related to the direction of swallowing laterality and an aspect of swallowing laterality does not significantly affect the severity of swallowing difficulty. The existing literature on swallowing difficulty recommended using the compensatory technique of rotating the head towards the laterality side or tilting it in the opposite direction. In the light of this study, the existing compensatory techniques such as head tilt and head rotation can improve swallowing laterality, but the possibility of no improvement can be inferred, so further study is needed.
The most marked difference between prior studies aimed at disease free people and the results of our research targeted at hemiplegic patients with stroke was that swallowing laterality had occurred more on the right side, even divided and examined with right hemiplegia and left hemiplegia. Supposing that patients before contraction of a stroke mostly had left laterality based on the results of previous research from disease free people, our result suggested the possibility, that a stroke may change the aspect of swallowing laterality. But as the relationship between the direction of hemiplegia and swallowing laterality was not observed, and as evaluation of swallowing laterality before the stroke was realistically impossible, it was difficult to infer what mechanism made the change of swallowing laterality.
The research also studied the influence of swallowing laterality on recovery from swallowing difficulty. The existence and the direction of swallowing laterality did not noticeably influence the severity and recovery of swallowing difficulty.
The limitations of this study are as follows: First, the individuals who participated in the research in order to confirm statistically significant results were too few. Second, there was no evaluation of the swallowing state of patients before the occurrence of stroke. In future research, studying what differences exist between disease free people and patients with stroke, should be done to verify how strokes are involved in swallowing laterality.
Go to :
CONCLUSION
Through this study, we found that there was no significant relation between swallowing laterality and the severity or prognosis of swallowing difficulty. As mentioned earlier, it is not enough to explain the mechanism of swallowing laterality in hemiplegic stroke because the study had some limitations. Thus, more studies for swallowing laterality on stroke patients will be needed.
Go to :
 XML Download
XML Download