

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although the primary sensorimotor cortex in the contralateral hemisphere is normally an area of primary activation while performing motor tasks,1,2 reorganization patterns in the post-stroke brain are diverse and reflect the interaction between connected brain regions, including more remote areas.3-5 To determine the characteristics of reorganization related to functional recovery, functional brain imaging modalities and functional topography, such as transcranial magnetic stimulation (TMS), have been used.6-10
Some studies have investigated whether ipsilesional and contralesional activation are relevant to functional restoration after stroke. Perilesional activation was observed in patients with good motor recovery.11,12 Furthermore, a decrease in contralesional and an increase in ipsilesional activation have been found to be related with better motor recovery in previous cross-sectional and longitudinal studies.3,7-11,13
FDG-positron emission tomography (FDG-PET) allows quantification of regional cerebral glucose metabolism in relation to neural activity, and enables the investigation of neural networks and functional associations in the brain.14 However, PET has limited temporal and spatial resolution. On the other hand, TMS, which maps cortical excitability with excellent spatial and temporal resolution, provides information about intracortical excitability and the intactness of the corticospinal pathway.15 However, TMS enables mapping of the motor-specific area only. Therefore, the integrated application of PET and TMS could lead to a better understanding of the mechanisms underlying post-stroke brain reorganization with regard to clinical recovery, and to better prediction of motor recovery outcome, which would allow the formulation of more specific therapeutic strategies for post-stroke recovery.
Therefore, we investigated motor reorganization patterns using PET and motor cortical excitabilities using TMS, and then searched for correlations between these and motor recovery after stroke, in a series of stroke patients that achieved various levels of motor recovery. We hypothesized that corticospinal output integrity is critically associated with functional reorganization, and that ipsilesional brain activation benefits clinical motor recovery.
Go to : 
MATERIALS AND METHODS
Ten patients with first-ever subcortical stroke (55.7±17.3 years, 5 ischemic strokes) were enrolled in this study. Stroke sites were identified by brain CT or MRI. All patients were right-handed according to the Edinburgh handedness questionnaire.16 The following exclusion criteria were applied: cortical stroke, multiple cerebral lesions, brainstem stroke, preexisting neurological or psychiatric disorders, deafness and/or blindness, aphasia, and the inability to obey 2-step commands.
Clinical evaluations
Initial assessments were performed at 37.7±25.2 days after stroke. Clinical evaluations included Mini-Mental Status Examination, Brunnstrom staging, manual muscle power testing according to the Medical Research Council scale, the Fugl-Meyer assessment (FMA), modified Barthel index (MBI) assessment, and manual function testing (MFT). Motor function was assessed at 6 months after stroke using Brunnstrom staging, manual muscle power testing according to the Medical Research Council scale, the FMA, the MBI, and MFT. We categorized patients into 3 groups according to motor function at 6 months. Patients were classified as having achieved: (i) "good recovery" if Brunnstrom stages of arms and hands were ≥5 and the patient could walk independently with/without a single cane; (ii) "fair recovery" if rated as being between "good" or "poor recovery"; and (iii) "poor recovery" if the Brunnstrom stage of an arm or hand was ≤4, or if the patient could not walk with a quad-cane.
PET study protocol
Images were acquired using a Phillips Allegro PET scanner (Philips Medical Systems, Cleveland, USA). The instrument used had an intrinsic resolution of 12 mm full width at half maximum (FWHM) and was able to simultaneously image 90 contiguous planes of 2 mm-thickness simultaneously for a longitudinal field of view of 256 mm. Subjects had fasted for more than 6 h before FDG-PET. Two FDG-PET studies were performed: one during rest and a second during a motor task. "Rest" PET scans were performed after a 30-minute rest within 1-2 days of the initial clinical evaluations. Patients were instructed to rest during the scan. An "activation" PET scan was performed on the day following the "rest" PET. Participants were asked to perform thumb-to-finger opposition using the affected hand as accurately and quickly as possible, keeping all other body parts still. The motor task began 30 seconds before a bolus infusion of 4.8 MBq/kg of FDG and continued for 30 minutes. An investigator observed directly any mirror hand movements during the task. Patients that could not accomplish the finger task were asked to dorsiflex the ankle as an alternative task. Brain imaging was conducted over 30 minutes in one table position and attenuation maps were obtained using a Cs-137 transmission source before radiotracer injection for 3D imaging. Attenuation-corrected images were reconstructed using the 3D-RAMLA (Row-Action Maximum-Likelihood) algorithm and a 3D image filter.
Differences between the 2 conditions (contrast "activation" minus "rest") were analyzed using SPM2 software (Wellcome Department of Imaging Neuroscience, Institute of Neurology, London, UK) implemented in MATLAB 6.5 (Mathworks Inc., Natick, USA). Subject images were normalized to the standard space using the Montreal Neurological Institute (MNI) to remove individual anatomical variabilities. Spatially normalized images were smoothed by convolution, using an isotrophic Gaussian filter (FWHM 10 mm) to improve the signal to noise ratio and to compensate for small residual anatomical variations. Mean global brain uptake was computed and individual voxel counts were normalized by proportional scaling to a mean brain FDG uptake per scan of 100.
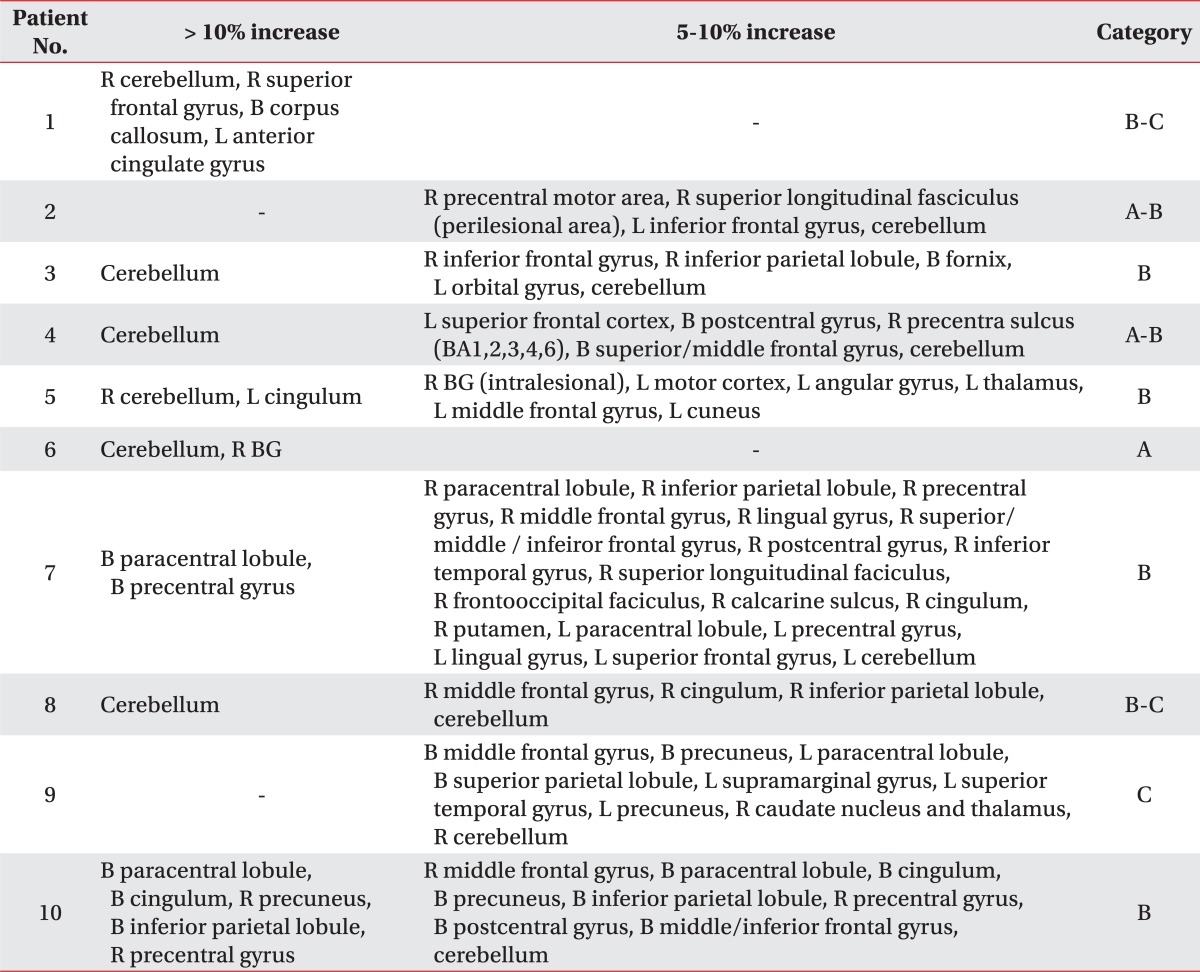
As the intra-individual variation of cerebral glucose metabolic measurement by FDG-PET has been known as low as 7.9%,17 the regions showing more than a 10% increase in glucose metabolism in "activation" PET scans versus "rest" PET scans by subtraction analysis was considered significantly activated. We categorized patterns of activation as follows: (i) category A as ipsilesional or perilesional activation; (ii) category B as contralesional activation; and (iii) category C as no definite activation.
TMS study protocol
TMS studies were performed within 7 days of the second PET using a figure-of-eight coil connected to a Magstim 200 magnetic stimulator (Magstim Co., Dyfed, UK). The external diameter of each loop was 90 mm and the peak magnetic field was 2.2 T. In each case, the coil was placed tangentially to the scalp, approximately 45° from the midline, and the handle of the coil was pointed 45° backwards and laterally. A combination of manual handling and mechanical fixation was used to ensure consistent coil placement throughout the study.
With a subject sitting in a comfortable chair, a disposable self-adhesive 19 mm diameter surface electrode (VIASYS Healthcare, Wisconsin, USA) was placed as a recording electrode on the abductor pollicis brevis (APB) muscle of the affected side. A reference electrode was placed on the first metacarpophalangeal joint. Motor-evoked potential (MEP) signals were filtered (3 Hz to 10 kHz), amplified, and displayed on a conventional electromyograph (EMG) (Medelec Ltd., Surrey, UK). Audiovisual feedback was provided to enable complete muscle relaxation.
Stimuli, at suprathreshold intensities, were given over patients' M1 cortices, while the coil was moved in 5 mm steps to determine the optimal scalp position, and the "hot spot" for APB muscle activation (where stimulus-evoked motor potentials had maximal peak-to-peak amplitude) was determined. If there was any MEP in the affected APB, we then determined its resting motor threshold (RMT), which was defined as the minimum stimulation intensity required to evoke MEPs of more than 50 µV during at least 5 of 10 trials. Using the same method, we located the unaffected hemisphere hot spot and its RMT.
Intracortical inhibition (ICI) and intracortical facilitation (ICF) were assessed from bilateral APB muscles using the paired-pulse technique at interstimulus intervals (ISIs) of 2 and 5 ms for ICI, and 10 and 20 ms for ICF, respectively. The conditioned MEP amplitudes at each ISI were expressed as percentages of the mean MEP amplitude during the test stimulation given alone. Throughout the study, subjects wore a tightly fitting thermoplastic grid cap on which the "hot spot" was marked to ensure accurate stimulation and consistent repositioning of the coil. To assess ICI and ICF, 2 Magstim 200 stimulators were connected through a BiStim module to a coil. The conditioning stimulus was applied at an intensity of 80% of RMT, and the intensities of the test stimulus were set at 120% of RMT; these intensities were kept the same in all paired-pulse trials. The interval between stimulations was ≥6 seconds.
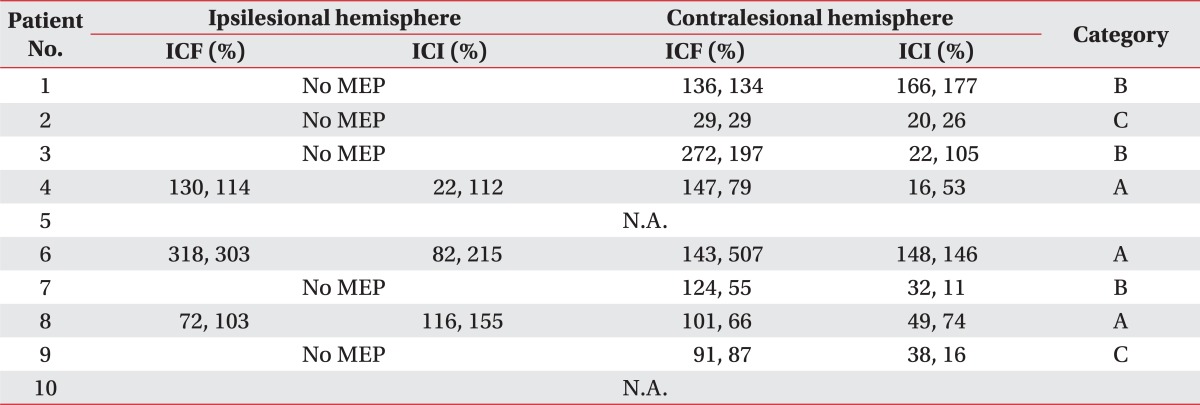
Then, we categorized TMS patterns as follows: (i) category A, when the MEP was evoked in the affected APB; (ii) category B, when the MEP was not evoked in the affected APB, but a normal ICF and/or ICI pattern was observed in the unaffected hemisphere; and (iii) category C, when no MEP was evoked in the affected APB and distorted ICI, and ICF patterns were observed in the unaffected hemisphere.
Go to :
RESULTS
The initial clinical characteristics of the 10 patients are listed in Table 1. Initially all patients showed distal upper limb weakness of less than grade 3. Brunnstorm stages of plegic hands ranged from 1 to 4. Mean FM scores in affected upper and lower limbs were 14.6±15.2 and 13.7±5.1, respectively. Mean MFT score was 3.5±4.3 in the affected limb, and the mean MBI score was 39.1±9.3.
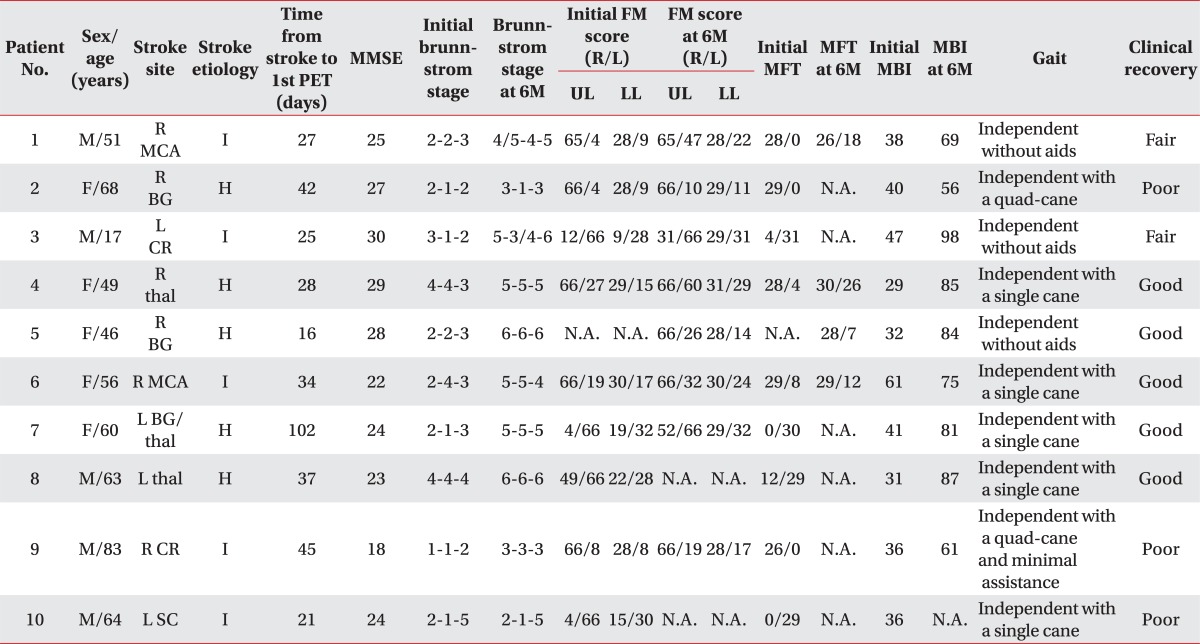
Table 1
Clinical Characteristics of Patients at Initial Evaluation and at 6 Months after Stroke Onset
MMSE: Mini-mental status examination, FM: Fugl-Meyer, UL: Upper limb, LL: Lower limb, MFT: Manual Function Test, MBI: Modified Barthel Index, MCA: Middle cerebral artery territory, BG: Basal ganglia, CR: Corona radiate, thal: Thalamus, SC: Striatocapsular, I: Ischemia, H: Hemorrhage, N.A.: Not available
![]()
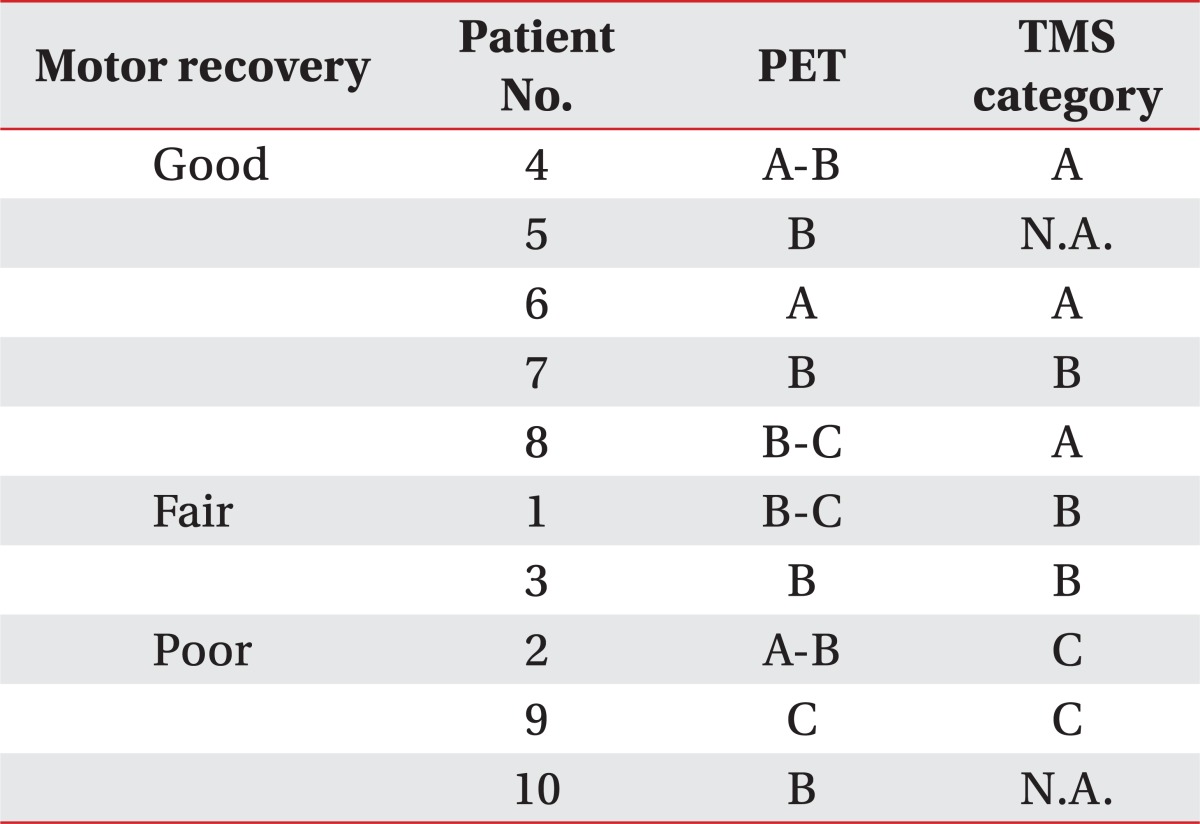
At final clinical assessments, Brunnstorm stages of plegic hands ranged from 1 to 6 (Table 1). All patients could walk and 3 patients were able to walk independently without any walking aids. According to our clinical recovery criteria, 5, 2, and 3 patients were referred to as having "good recovery", "fair recovery", and "poor recovery", respectively.
Patients with a clinical "good recovery" (Patient 4-7 and 8)
The Brunnstrom stage of the arm and hand of patient 4 was 5 and she walked independently. Her PET showed significant activation in the cerebellum and less significant activation in bilateral cerebral cortices (PET category A-B). Normal ICI/ICF patterns (TMS category A) were observed in both hemispheres (Fig. 1).
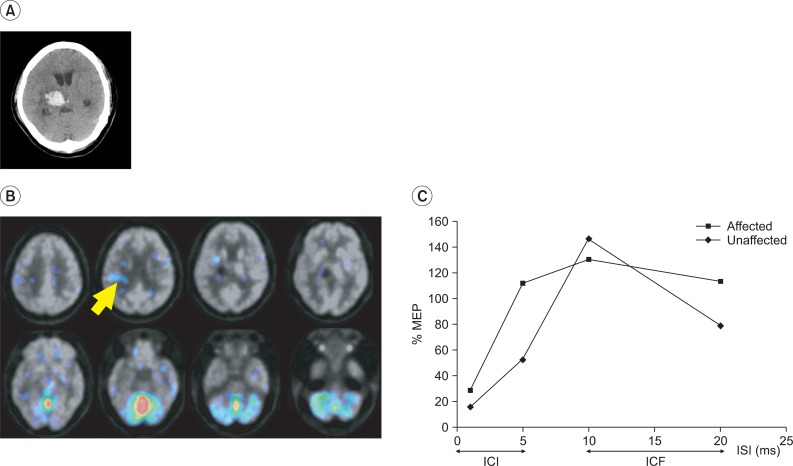 | Fig. 1A patient in a good recovery group (Patient 4). (A) Brain CT showed a hemorrhagic lesion in the right thalamus. (B) During the motor task, activation was observed in the cerebellum and perilesional motor cortex (arrow) on her FDG-PET. (C) Normal ICI and ICF response patterns were observed in bilateral motor cortices on the paired pulse TMS. ICI: Intracortical inhibition, ICF: Intracortical facilitation, ISI: Interstimulus interval, ms: Milliseconds.
|
Patient 5 had an upper extremity Brunnstrom stage of 6 and she walked independently without walking aids. She was at "PET category B" with significant activation in the ipsilesional cerebellum and contralesional cingulum. Activation of 5-10% was observed in the contralesional hemisphere, including the intralesional area. MEP data were not available.
Patient 6 had an upper extremity Brunnstrom stage 5, and she walked independently. She was at "PET category A" with significant perilesional activation. MEPs showed normal ICI/ICF patterns bilaterally (TMS category A).
Patient 7 had an upper extremity Brunnstrom stage of 5 and walked independently. She was at "PET category B", with widely distributed activations in the bilateral cerebral hemispheres and the ipsilateral cerebellum. No MEP was evoked in the hemiplegic APB, but normal ICI/ICF patterns were observed in the unaffected APB (TMS category B).
Patient 8 achieved full neurological recovery according to the Brunnstrom staging system and walked independently. However, his PET finding was categorized as B-C. Significant activation was observed in the cerebellum, and 5-10% activation was only observed in the contralesional cerebral hemisphere. The MEP revealed normal ICI/ICF patterns in both hemispheres (TMS category A).
Patients with clinical "fair recovery" (Patient 1 and 3)
Patient 1 had an upper extremity Brunnstrom stage of 4 and walked independently without walking aids. He was at "PET category B-C" with significant activation in the ipsilesional cerebellum and the bilateral cerebral hemispheres. No MEP was evoked in the hemiplegic APB, but a normal ICF and an abnormal ICI pattern were observed in the unaffected APB (TMS category B).
The Brunnstrom stage of the upper extremity of patient 3 was 5 for the arm and 4 for the hand. He walked independently without walking aids, and was at "PET category B" with significant activation in the cerebellum and ≤10% activation in the contralesional cerebral cortex. No MEP was evoked in the hemiplegic APB, but normal ICI/ICF patterns were observed in the unaffected APB (TMS category B) (Fig. 2).
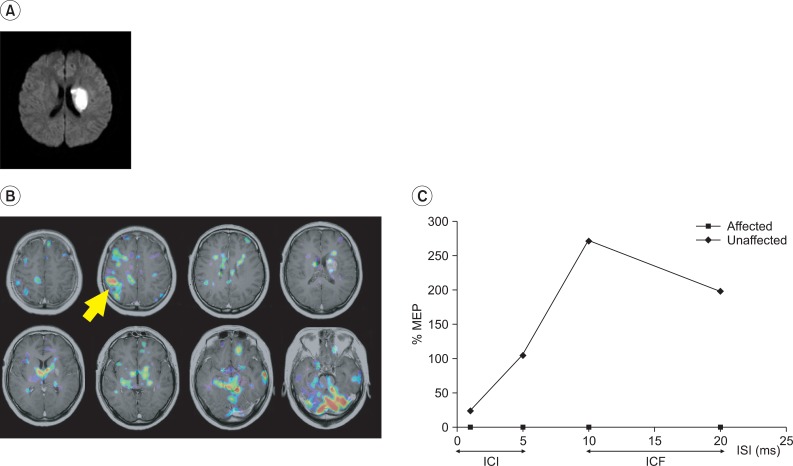 | Fig. 2A patient in a fair recovery group (Patient 3). (A) Brain MRI showed an acute infarct in the left corona radiata. (B) During the motor task, activation occurred in the contralateral motor cortex, the cerebellum, the perilesional area, bilateral frontal cortices and thalamus. (C) No MEP was observed in the affected APB, but normal ICI and ICF patterns were observed in the unaffected side. ICI: Intracortical inhibition, ICF: Intracortical facilitation, ISI: Interstimulus interval, ms: Milliseconds.
|
Patients with a clinical "poor recovery" (Patient 2, 9, and 10)
Patient 2 had an upper extremity Brunnstrom stage of ≤3. She needed a quad cane to walk, and was at "PET category A-B" with ≤10% activation in the ipsilesional cerebral hemisphere. No MEP was evoked in the hemiplegic APB, and normal ICI, but abnormal ICF patterns were observed in the unaffected APB (TMS category C).
Patient 9 had an upper extremity Brunnstrom stage of 3 and needed a quad cane and assistance to walk. His PET showed non-significant activation compatible with "PET category C". No MEP was evoked in the affected APB and abnormal ICI/ICF patterns were observed in the unaffected APB (TMS category C).
Patient 10 had an upper extremity Brunnstrom stage of ≤2, but walked independently. He was at "PET category B" with significant activation in the contralesional cerebral hemisphere. No MEP was available.
Go to :
DISCUSSION
In this study, we investigated activation patterns during a motor task using PET, and the integrity of corticospinal output and intracortical excitability using TMS in a group of patients with subcortical stroke during the subacute stage of motor recovery. It was found that the preserved integrity of the corticospinal pathway in ipsilesional hemispheres and of the intracortical networks in contralesional hemispheres is correlated with good functional recovery. However, the notion that ipsilesional or perilesional activation during motor tasks is related to good motor recovery is less supported by our data.
Post-stroke motor recovery relies on reorganization in the affected and intact hemispheres, which has been postulated to occur via the unmasking of latent synaptic connections and synaptogenesis.6 Increased contralesional activation reflects recruitment of the uncrossed motor pathway or disinhibition of the intact motor cortex via transcallosal fibers.18 The more severely a unilateral hemisphere is damaged, the more distinct the transhemispheric disinhibition is. Therefore, significant contralesional activation suggests more severe damage and poorer recovery.
Although the roles played by ipsilesional and contralesional hemispheres in post-stroke recovery remains controversial, previous studies have shown that increased recruitment of the ipsilesional hemisphere and reduced recruitment of the contralesional hemisphere are related to good motor recovery.3,4,7-13,19-21 A meta-analysis also demonstrated that neural reorganization in the ipsilesional sensorimotor cortex accompanies motor recovery of the affected hemiplegic upper extremity.22
Our results are in line with previous results, with respect to the finding that significant activation in the affected hemisphere is more closely associated with good motor recovery than significant activation in the intact hemisphere or insignificant activation. However, in the present study, significant contralesional activation in PET was found to be less correlated with good recovery than contralesional activation on TMS.
TMS measures the excitability of underlying corticospinal neurons. In healthy subjects, cortical excitability measured using TMS reflects muscle strength and fine motor function.23 In stroke patients, changes in cortical excitatory and inhibitory systems have been described in TMS studies, such as, higher motor thresholds, lower amplitude MEPs, and prolonged silent-periods.5,24,25 In addition, studies have also shown that the intactness of corticospinal output, that is, the presence of MEPs, during the early post-stroke stage has predictive value in terms of the long-term motor recovery.5,7-10,24,26-31
In addition to evaluations of the integrity of the corticospinal pathway, measurements of the excitabilities of the excitatory and inhibitory intracortical pathways are possible using a paired-pulse paradigm in TMS. A suprathreshold "test" magnetic stimulus is suppressed by a previous "conditioning" subthreshold magnetic pulse delivered at ISIs of 2-3 msec, due to the activation of GABAergic interneurons, and facilitated by that delivered at ISIs 10-20 msec, due to the activation of glutamatergic interneurons.32 Although the results of studies investigating the clinical implications of intracortical excitability of the contralesional hemisphere have been contradictory, an increase in intracortical excitatory activity was demonstrated in the unaffected hemisphere in recovering stroke patients.12,33,34 This suggests that the mechanisms underlying increased ICF in the unaffected hemisphere are related to good motor recovery after stroke. The integrity of ICI in contralesional hemispheres was also found to predict good motor recovery, because it reflects the maintenance of transcallosal inhibition by affected hemispheres.32
This study has several limitations that should be considered when interpreting the results. First, because the activation PET study was performed during the early post-stroke stage in most cases, several patients were unable to perform the thumb-to-finger opposition task. For these patients, we substituted dorsiflexion of the plegic ankle for the motor task. Thus, the inconsistency of motor tasks performed and the accompanying different levels of task difficulty and the amount of concentration required would have influenced the region of activation. However, in the present study, we sought hemispheric patterns of activation, rather than specific localizations of activation, and thus, we consider that task inconsistency would have not affected our results. Second, we performed PET and TMS study just once. Previous studies have shown that there is an evolution of brain activation over time. Therefore, a longitudinal study would have undoubtedly benefited predictions of clinical outcome. Third, the subject group was not homogeneous with respect to stroke type: 5 patients had experienced an hemorrhagic stroke and 5 patients had experienced an ischemic stroke. Moreover, the time since stroke varied among subjects, from 16 days to 102 days. However, only one patient (patient 7) was enrolled significantly later than the other 9 patients, who were enrolled at post-stroke day 16 to day 45. This subject heterogeneity might have obscured the interpretation of the results. Fourth, there is limited power in the current small-sized study. We could only describe the results as a form of case series.
Despite the above limitations, we suggest that the integrity of corticospinal output and normal inhibitory and excitatory intracortical activities, as demonstrated by TMS, and an increase in task-related metabolism in the ipsilesional hemisphere, as demonstrated by PET, are relevant to the reorganization process required for good motor recovery after stroke. We suggest that our approach to investigating brain reorganization after stroke provides better insight into motor function recovery than previous approaches.
Go to :
 XML Download
XML Download