

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Epidural steroid injection has been used for treating pain due to lumbosacral radiculopathy.1 The injections can be delivered into interlaminar, caudal, and transforaminal locations. Because of its advantage of selectively injecting drugs into a specific nerve root, transforaminal injection method is preferred.1,2 There are 3-4 types of well-known approaches in the transforaminal injection method, and among those, the most used is the infrapedicle transforaminal injection which has the injection needle approach the safe triangle below the underside of the pedicle so that contrast dye usually spreads to L4 root in case of L4-5 level, and if the L5-S1 level, mostly spreads to L5 root.3 Preganglionic approach accesses the suprapedicle level, and contrast dye is known to spread over to L5 root in case of L4-5 level, and to S1 root in case of L5-S1 level.4
In the case of infrapedicle approach, there are numerous cases where the injected drug would flow into the cephalic root of the nerve root, and in the case of severe foraminal stenosis, in many cases the injection needle is unable to reach the desired location after penetrating the intervertebral foramen.5 Furthermore, with regard to infrapedicle approach, there are even cases where drugs cannot be injected into the epidural and preganglionic part of the supraadjacent intervertebral disc.4 At that point, a retrodiscal (RD) approach can be used as an alternative method.
In determining the level of retrodiscal (RD) approach, it is critical to know to which nearby nerve root the contrast dye spreads. Current research is not clear on spread patterns of RD EPB contrast dye.
In this study, the authors investigated the spreading pattern and location of contrast dye and the clinical features of the transforaminal epidural block according to the retrodiscal (RD) approach, relatively unknown to the present.
MATERIALS AND METHODS
Subjects
The patients, who visited the Department of Rehabilitation at the authors' hospital with chief complaints of back pain and radiating pain, were diagnosed as L5 radiculopathy by physical examination, medical imaging, and electromyographic examination. Patients who were planning to receive transforaminal injection treatment were consecutively included.
Patients who had received steroid injections or prescriptions within the previous three months, or had a history of diabetes, general peripheral neuropathy, cerebrovascular accident, or inflammatory joint disease were excluded from the study. To examine which nerve root the drug injection spreads to, the subject patients were consecutively randomized into L4-5 RD approach group and L5-S1 RD approach group.
Methods
The subjects lay prone on the C-arm table with a pillow supporting the lower abdomen and upper iliac to reduce lumbar lordosis, and the C-arm was tilted from the cranial to caudal part in order to align the superior-inferior ephiphyseal plate of the relevant vertebrae. Then, the C-arm was rotated at a 40-45 degree angle to the limbs, and the superior articular process of S1 was set to be placed in the central point of the disc space. 22 gauge 5 inch spinal needle; Spinal needle Spinocan® (BRAUN, Melsungen, Germany) was inserted into the skin and was pressed forward to the side that is parallel to the axis of the X-ray route. Once the spinal needle passes through the extrapolation of the superior articular process and comes in contact with the retrodiscal (RD) surface, the needle is checked to see that it did not go over the virtual disc back line by turning the C-arm towards the lateral view.
To examine the spreading pattern of the contrast dye, 1 cc of non-ionic contrast dye; Omnipaque™ (GE Healthcare, Cork, Ireland) was injected, and through the anterior-posterior and lateral views of the X-ray, the spreading pattern of the contrast dye and the nerve root it usually spreads to were observed. In addition, for the treatment, 1 cc of 0.5% lidocaine mixed with 20 mg of triamcinolone was injected.
To examine if there is an association between the spreading pattern of contrast dye and pain reduction, a visual analogue scale (VAS) was obtained before and 2 weeks after the procedure.
RESULTS
General characteristics of subject patients
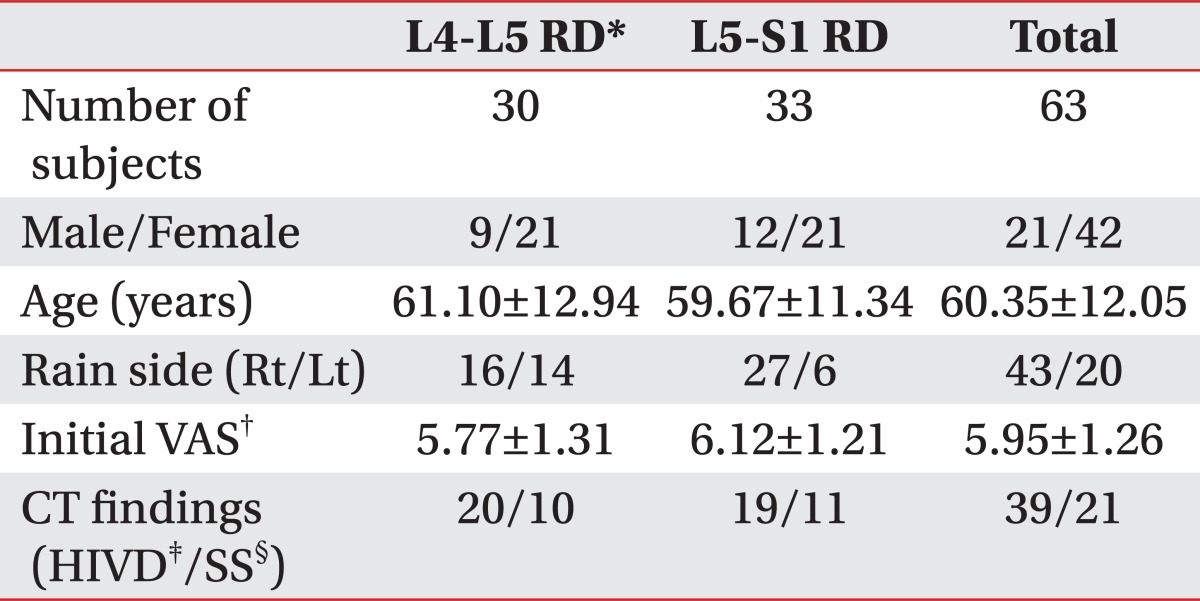
There was 30 people (Men: 9, Women: 21) in the L4-5 RD group, and 33 people in the L5-S1 RD group (Men: 12, Women: 21). The average age of L4-5 RD group was 61.10±12.94 years, and that of L5-S1 RD group was 59.67±11.34 years. In the L4-5 RD group, 16 people had the pain on the right side and 14 had the pain on the left, in the L5-S1 RD group, 27 people on the right side, and 6 on the left side. The visual analogue scale (VAS) was 5.77±1.31 in the L4-5 RD group, and 6.12±1.21 in the L5-S1 RD group. CT revealed L5-S1 herniated intervertebral disc in 20 people, spinal stenosis in 10 in the L4-5 RD group. In the L5-S1 RD group, 19 had L5-S1 herniated intervertebral disc and 11 had spinal stenosis. There was no significant difference between the two groups in general characteristics (Table 1).
Nerve root spreading location of contrast dye according to procedure level
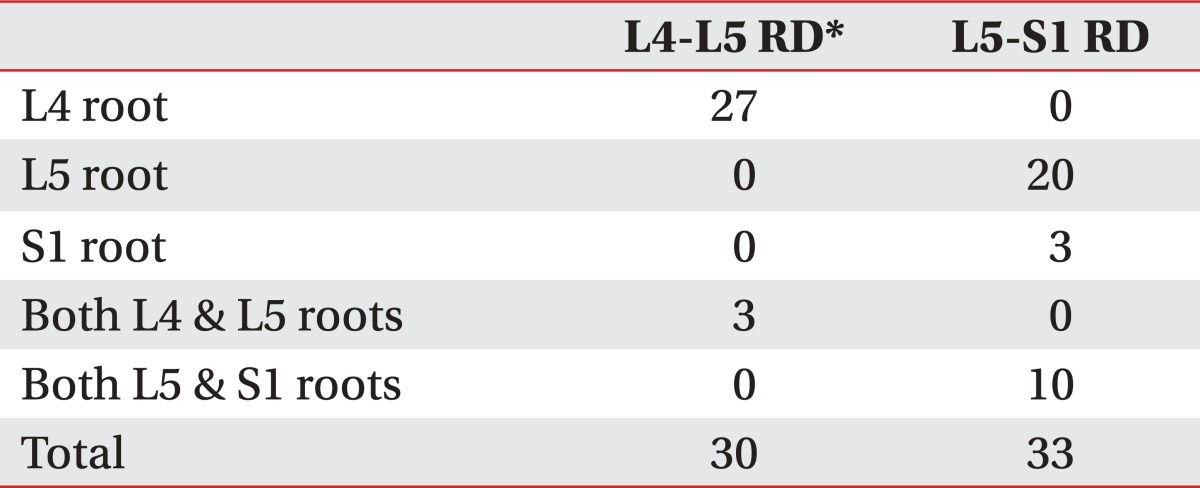
Contrast dye usually spread over to the upper nerve root. In the L4-5 RD group, the contrast spread over the L4 nerve root in 27 cases, and the L4 and L5 nerve roots in 3 cases. Out of the 33 subjects in the L5-S1 RD group, the contrast spread to the L5 nerve root in 20 cases, to both the L5 and S1 nerve root in 10 cases, and to the S1 nerve root in 3 cases (Table 2).
Contrast spreading pattern
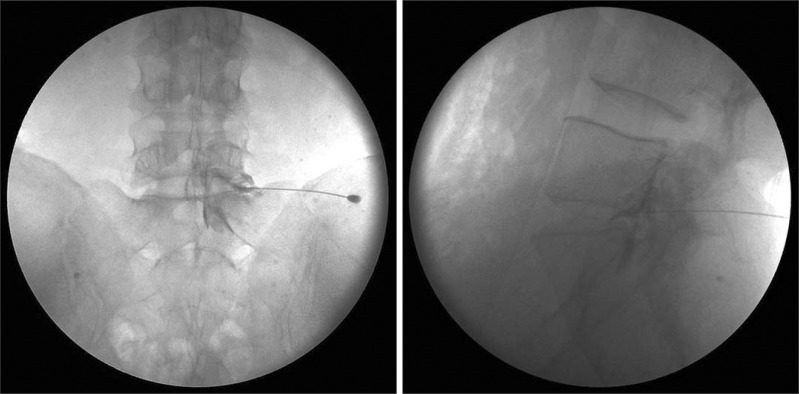
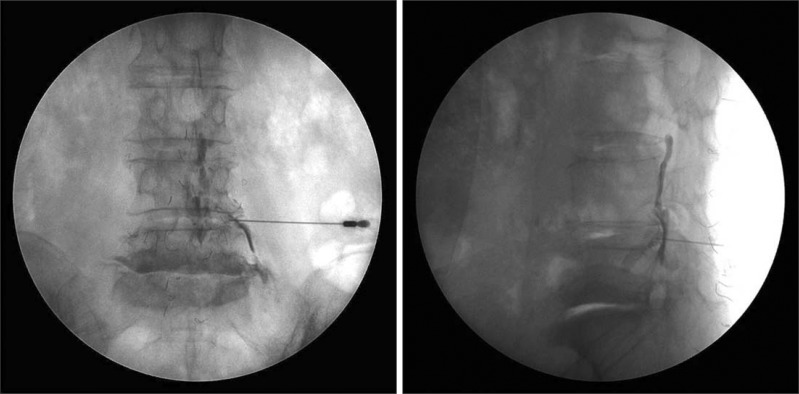
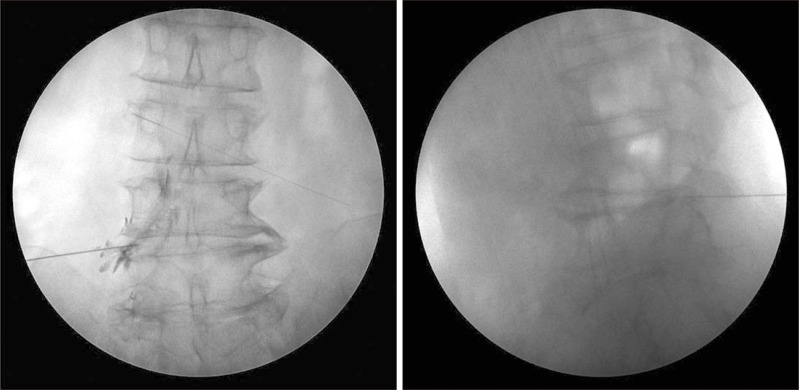
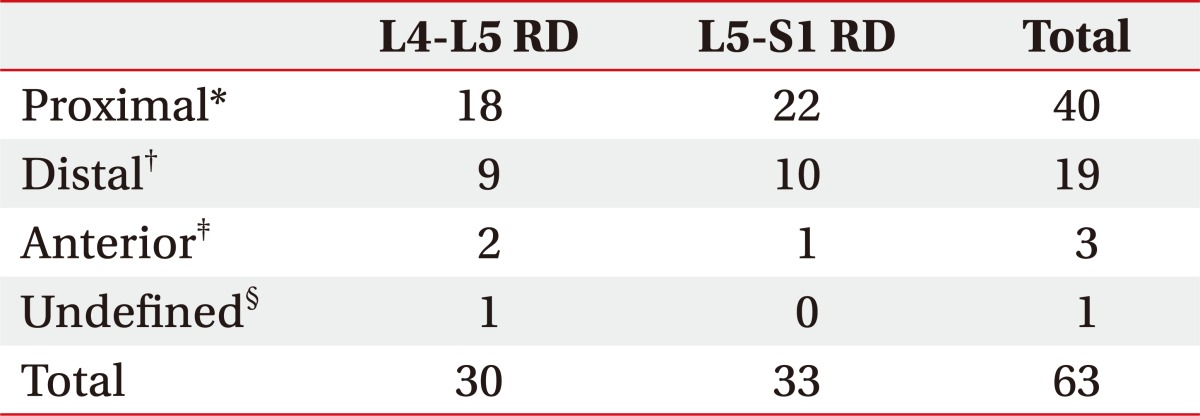
The contrast spreading pattern could be divided into four patterns (Fig. 1~4): 40 cases where the contrast dye usually spread to the distal target nerve root, 19 cases where the contrast dye usually spreads to the proximal target nerve root, 3 cases where the contrast spreads to the anterior epidural space, and lastly, 1 case with an undefined pattern which does not fall under any of the previous three patterns (Table 3).
Contrast spreading pattern and clinical characteristics due to it
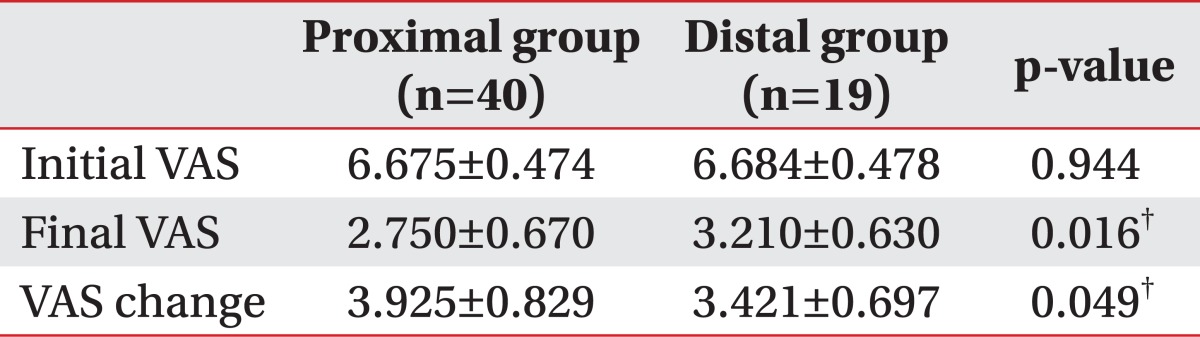
The pain intensity 2 weeks after the procedure (VAS) was 2.750±0.670 in the group where contrast spread to the proximal nerve root, and 3.210±0.630 in the group where it spread to the distal nerve root, a statistically significant difference. The changes in pain after the procedure (VAS change) also were statistically significant, comparing 3.925±0.829 in the group where the contrast spread to the proximal nerve root, and 3.421±0.697 in the group where it spread to the distal root (Table 4).
DISCUSSION
Transforaminal epidural injection method has an excellent curative effect in treating chronic lumbar nerve root pain syndrome, and has been used extensively in a clinical setting due to its satisfactory effect in the long term.6
When transforaminal epidural injection method is performed, the contrast dye must spread over to the proximal region along the anterior lateral part of a specific nerve.7,8,9 However, a considerable amount of the drug injected via infrapedicle approach sometimes flows into the distal region along the spinal nerve, and it becomes difficult to insert the injection needle in the case of severe spinal stenosis when the needle is supposed to be located at the region more anterior to the intra-transforaminal epidural nerve root.10
As an alternative to this, the retrodiscal (RD) approach can be applied. The researchers have concluded that the epidural block by L5-S1 retrodiscal (RD) approach can reduce the stimulation to the nerve root during the procedure compared to the infrapedicle approach. This is a helpful method especially when the disc sequestrum is stuck in the medial intervertebral foramen or when spinal stenosis is severe.10
With regard to determining the level of RD approach, it is very important to be aware of which nearby nerve roots the contrast dye is spreading to. However, studies done on which nerve root the drugs spread to are insufficient. The authors found that the contrast dye mainly spreads over the upper nerve root regardless of the level of the procedure when performing a procedure with the RD approach (Table 2). This is likely due to the anatomical structure of the spinal epidural space. Although contralateral spread of the contrast dye was not observed in this study, the authors noted that in a considerable number of cases, the contrast spread to even the nerve roots below the level of the targeted nerve root apart from the targeted nerve root. When over 0.5 ml of contrast dye was injected, the contrast can spread to more than one of the nearby (superior, inferior, and/or contralateral) nerve roots.7,11 Because 1.0 ml of contrast dye was administered in this study, it was observed that the contrast spread to not only the targeted nerve roots but also to the nerve roots below the level of the targeted nerve roots.
The authors found that the contrast dye in the RD approach usually spread to the proximal target nerve root (40/63, 63.5%) (Table 3). In case of the contrast dye spreading to the distal root, the authors observed that the resulting changes in pain (VAS change) before and after procedure was less compared to the patients with a spread to the proximal root. This is attributed to the inability of the contrast dye to rise to the proximal nerve root and its flowing down to the distal root following the spinal nerve by the synechia of epidural space including the root sleeve.
This study has its limitations. First, when recruiting the subject group for this study, all patients with severe spinal stenosis or herniated intervertebral disc were included, and because some patients with severe synechia of epidural space were included among them, there were many cases where the injected drugs spread to the distal nerve root. Therefore, if a study is conducted in the future to judge the effect of the contrast spreading pattern on pain reduction, it should be carried out after excluding patients with severe spinal stenosis or severe herniated intervertebral disc. Second, the level of pain was recorded with VAS before the procedure and two weeks after the procedure. It seems that using another scale besides VAS would be helpful to enhance the objectivity of the results. Furthermore, the mid- to long-term effect of the procedures could be identified if follow-up is conducted not only two weeks but also six months or more after the procedure.
CONCLUSION
When performing lumbosacral transforaminal epidural block by the retrodiscal (RD) approach, the contrast dye mostly spread to the cephalic root regardless of the level of the procedure. The pain-reducing effect two weeks after the procedure was better when the contrast dye spread over to the relevant proximal nerve root rather than to the distal root.

 XML Download
XML Download