

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Locked-in Syndrome (LIS) introduced by Plum and Posner in 1966, represents a severe pontine infarction syndrome in which quadriplegia, lower cranial nerve paralysis and mutism are caused by vertebral and basilar artery thromboses. The LIS is a condition in which functions of consciousness and cognition are maintained but there are defects of all movements other than eye blinks and vertical eye movements.1
The LIS patient's possible voluntary movements are eye blinks and vertical eye movements; hence, these functions play a role as a means of communication with the surrounding environment.
The recent development of assistive technology has invited patients who cannot conduct verbal communication to widen the options of augmentative and alternative communication (AAC), whereby each of these patients can attempt to satisfy his/her demands. Further, the distribution of computers has been expanded and internet access has become easier. Therefore, various attempts have been made for the communication of patients who cannot carry out any physical activities.
Nevertheless, no research has been conducted on LIS patients' communication in Korea. Therefore, this research discusses the training of communication using AAC, together with a review of related literature.
CASE REPORT
In our hospital, a 52-year-old male patient was hospitalized who had paralyses of the upper and lower limbs, mutism, respiratory disorder, and dysphasia. The patient had entered a Korean oriental medical clinic with dizziness and dysarthria 5 months prior to the hospitalization. He showed a sudden progress of altered mental status, quadriplegia, for 3 days. Due to these symptoms, he was transferred to the ER at a general hospital. While hospitalized in the general hospital, in tests using Magnetic Resonance Imaging (MRI) scan and angiographical inspection he was diagnosed with infarctions of cerebella, pons, midbrain, corpus callsum, of the left occipital lobe and the right thalamus caused by bilateral vertebral and basilar artery occlusions. At ICU, he received acute phase treatments (e.g. tracheostomy and respirator, anticoagulation therapy, etc.). After these treatments, he was in a stable condition, receiving hospital treatments for approximately 4 months. In order to receive comprehensive rehabilitation therapy, he entered our hospital approximately 5 months later after he showed the previously mentioned symptoms. When showing these symptoms 5 years ago, he was diagnosed with diabetes and high blood pressure and he was then administered drugs continuously. He had no particular family history of these diseases.
After he was admitted into our hospital, he received a neurological examination. The test showed that he was in a conscious state. However, his cognitive and perceptual abilities could not be determined due to the difficulty in communicating with him. The cranial nerve examination showed a voluntary minute tilt of the right side of his head. He could move his eyeballs in limited perpendicular and horizontal directions and blink his eyes. Also, bilateral facial paralyses were observed. He could not project his voice nor could he swallow anything. He could not move his tongue and the gag reflex did not occur.
The muscular strength of the upper and lower limbs measured by Manual Muscle Testing (MMT) is grade zero. The spinal reflex of the limbs increased. The muscle tone assessment showed that the right upper and lower limbs and the left limbs were in Steps 2 and 3 respectively. The patient's Korean modified Barthel index (K-MBI) was Grade 0/Grade 100 because he needed the carer's absolute help when performing all physical activities and activities of daily life.
The patient did not make an attempt to express himself. After he entered our hospital, he was trained to express "Yes" or "No" by using a certain number of eye blinks. At the Rehabilitation Center attached to our hospital, he received alternative communication training to express himself more concretely and actively, by using a software program related to the alternative input device.
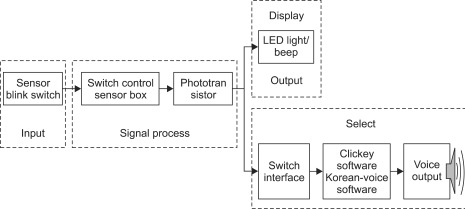
We fitted glasses on the side of his left eye by attaching these glasses to SCATIR (Self-Calibrating Auditory Tone Infrared) Switch (TASH, Roseville USA), which detects an infrared reflection stimulated by physical activities because he could not perform activities other than eye blinks (Fig. 1). Further, Switch Interface Pro5.0 (Don Johnston, Illinois, USA) was used, which delivers the input signal sent by the switch, operated when the patient blinks his eyes, to software programs and NeoSpeech Yumi (NextUp Technologies LLC, North Carolina, USA), a voice output software program (Fig. 2).
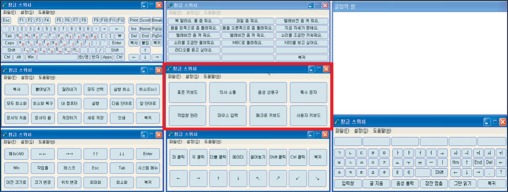
According to the situation, he received training in the position of sitting on a bed or a wheelchair 40 minutes a day for 3 weeks. During the first week, the software programs Evaluware (Tobii Assistive Technology, Massachusetts, USA), Northern Grid For Learning activity (Northern Grid, Tyne and Wear, UK), and Sim tech single switch software for preschoolers (Don Johnston, Illinois, USA), etc., were used to improve the accuracy and speed of eye blinks, (Fig. 3). This would encourage the patient to correctly click at regular time intervals (Fig. 4). For 2 weeks after the first week, he received training in the use of Clickey2.0 (Seong-Pil Kim, Seoul, Korea), which enables the relevant person not only to use all functions of a keyboard only by clicking but also to output the chosen expression (i.e. a target word or sentence automatically scanned after its input operation) into a voice (Fig. 5).
The three-week training enabled the patient to express simple words (e.g. "bada (sea)" and his name by the combination of words using functions of the keyboard. Further, it enabled him to deliver some of his ideas and feelings by outputting the selected sentences (e.g. "I love you," "When am I leaving the hospital?" etc.) into a voice with an audio glossary function.
DISCUSSION
According to the existing studies, the mortality of LIS patients is approximately 67%2 and the survival rate of the patients who survived 5, 10 and 20 years is 83%, 83% and 40%, respectively.3 The 19-month follow-up investigation of LIS patients' functional recovery showed that only 21% of patients were able to perform some activities of daily life and the other patients (79%) needed other peoples' absolute help for living.4
LIS patients who survive with clear consciousness for a long time and whose functional activity recovery is difficult need a communication method for living at home and in society. Therefore, various types of devices and methods have already been introduced and used. In 2001, the application of AAC was attempted, which used the activities of thumbs, the chin, the head, and shoulders of 17 LIS patients in Finland; of these, 9 patients were finally able to use a computer for Internet access or for sending and receiving daily e-mails.5 In addition, in research carried out in the United States in 2003, 2 LIS patients diagnosed 11 years prior to 2003 returned to their position (i.e. lawyer and mathematics teacher) by communicating with eye blinks and a mouse stick.4
LIS is classified into three categories according to whether or not physical activities and communication can be performed. Classic LIS refers to the loss of physical activities other than vertical eye movements, as defined by Plum and Posner. Incomplete LIS represents a condition in which voluntary activity functions except for vertical eye movements remain and total LIS refers to a condition in which the functions of all physical activities are lost and communication between the relevant patient and others is impossible.6
It was observed that the patient in this study had a voluntary minute right head tilt. The patient could move his eyeballs perpendicularly and horizontally and blink his eyes. According to the above classification, he can be classified as an incomplete locked-in syndrome (LIS) patient. However, he showed an intermittent rotary nystagmus of the eyeballs; he could functionally use the blink of the eyes. Therefore, we attempted to communicate with him by using this behavior.
If the eyes are close to the blink switch due to the characteristic of the input device while that device is being operated, the sensor will respond perceptively to the weak blink of the eyes and the operator cannot correctly click the scanning object. It is important for the operator to fix the correct position by adjusting properly the distance between the switch and the eyes. For the patient, at first we attempted to click by attaching the switch to the fixing frame attached to the bed. However, we devised a way for the patient to wear the glasses in which the switch is attached so that the distance between the switch and the eyes can be maintained and that the carer can attach it easily. The patient received training in clicking every three seconds 5 days after the location is set up; the training showed a 70% average accuracy. The patient was able to click every two seconds, five days after the training. The last one week's training included his actual use of the device.
The problem with the training is that the use of the device is greatly influenced by a patient's will and physical condition on the actual day of training. The relevant patient consumed a great deal of time because, in the method, a phoneme was input into the patient, in which the cursor is circulated every two seconds. The frequent expelling of Phlegm caused the problem of a fall in concentration and accuracy of the training. In addition, the patient received training in the seated position and in tilting postures with various angles because the patient had difficulty in maintaining a suitable position due to strained cervical muscles during the training. Finally, the patient received training in the seated position of tilting the truncus back at approximately 15 degrees, maintaining the head in the forward direction by attaching a Velcro strap to the head rest of a wheelchair. This study will be able to further contribute to the creation of training effects and to an increase in quality to compensate for the defect of the training position in order to maintain the optimum position by manufacturing a rest for supporting a trunk or an inner made of polyurethane for fitting the body shape.
When completing the training, the patient said that he had difficulty in directly combining words by using phonemes but useful vocal sentences were convenient due to their relatively easy use. Further, he added that he wanted to use this system continuously for his communication in the future.
The interaction between the patient and the surrounding environment including with other people is not only a human's basic desire but also an important factor for improving the quality of life. We cannot completely replace normal language or emotional communication with the system applied for the patient. However, this AAC can form and express not only a patient's basic demands but also personal decision-making or deeper ideas. We can consider the return of a patient skilled in the system to his/her career.
In the field of rehabilitation, the actual use of assistive technology needs the interest of the whole rehabilitation team and its continuous efforts. Also, it requires the development of a program convenient to use as well as professional training. This case proved that the efforts of the relevant persons (i.e. the medical team, therapists, the research team, the patient and his family) and the collection of their opinions could make it possible to devise an AAC (i.e. a possible communication method which is low-priced, convenient, and accurate that has not been suggested previously) by enabling the patient to install a free software program developed in Korea into his/her computer and to install only the switch and the fixing frame.
Therefore, this case study will supply not only the possibility and opportunity of communication to LIS patients, but it will also contribute to the generalization of the communication device and its actual use, for the relevant patients' return to their family and society.



 XML Download
XML Download