

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lower limb nerve conduction studies are performed when lumbar radiculopathy or peripheral neuropathy of the lower limb is suspected. The deep peroneal motor nerve (DPN) is one of the most frequently tested nerves in the lower limb. In conventional DPN conduction studies with extensor digitorum brevis (EDB) muscle recording, the nerve is stimulated approximately 8 cm proximal to the active recording electrode and just lateral to the tibialis anterior (TA) tendon, and is also stimulated at the fibular neck.1,2 Typically, the amplitude of the compound muscle action potential (CMAP) obtained on distal stimulation is higher than that produced by proximal stimulation due to phase cancellation.
However, distal stimulation may produce lower CMAP compared to proximal stimulation. In these cases, we should suspect the presence of an accessory peroneal nerve as well as confirming the location of the optimal distal stimulation suggested by the literature.3-5 In the absence of an accessory peroneal nerve, the location of the distal stimulation should be reconsidered.
In a previous study, we assessed the optimal location of distal stimulation for the DPN conduction study in a sample of healthy volunteers. In most cases, the optimal stimulation site for maximal CMAP was 2 cm lateral to the TA tendon.6 However, the study only revealed the surface distance of the stimulation point from the TA tendon. We could not discern the structural location of the DPN related to the TA, extensor hallucis longus (EHL), and extensor digitorum longus (EDL) tendons.
The purpose of the present study was to investigate the relative location of the DPN around the ankle through anatomical studies of cadavers, to identify the optimal distal stimulation point for use in conventional peroneal motor nerve conduction studies.
MATERIALS AND METHODS
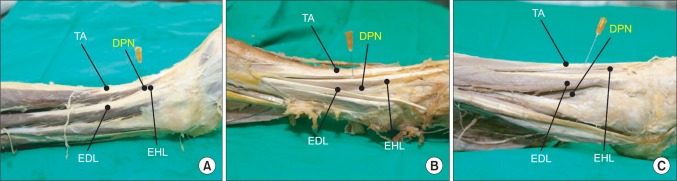
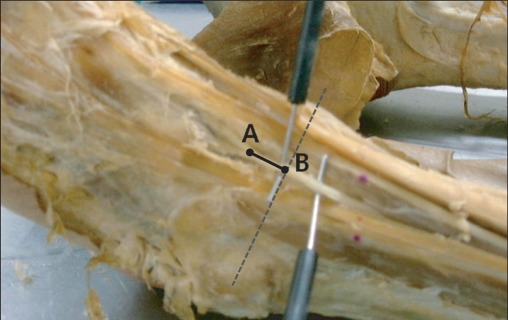
We dissected 30 ankles from 20 cadavers (eight women and 12 men; median age, 53 years; age range, 41-88 years) to identify the location of the DPN. The ankles in 10 cadavers were dissected bilaterally. The ankles in the other 10 cadavers were dissected unilaterally because the other ankles were already dissected for medical student practice. We measured the distance (DPN_TA) between the DPN and the TA tendon at a point 8 cm proximal to the central point of the EDB muscle, and examined the relationship of DPN to the TA, EHL, and EDL tendons with the ankle plantar flexed about 45 degrees. Depending on the location of the DPN at this point near the ankle, its course was categorized as Type 1, lying between the TA and EHL tendons; Type 2, lying between the EHL and EDL tendons; and Type 3, lying lateral to the EDL tendon (Fig. 1). We also measured the distance (DPN_CP) between the bifurcation of the DPN at the ankle and the point at which the DPN crossed the mediolateral malleolar line (CP) (Fig. 2).
Statistical analyses
Non-parametric analysis for all data was performed with the statistical package SPSS version 12.0. Wilcoxon signed rank test was used to test for side-to-side differences and Kruskal-Wallis test for DPN_TA differences according to types of relative location of DPN. A p-value <0.05 was considered statistically significant.
RESULTS
The median DPN_TA was 10 mm and the range of DPN_TA was 1-21 mm. The relative location of the DPN was between the TA and EHL in nine cases (Type 1, 30%), between the EHL and EDL in 18 cases (Type 2, 60%), and lateral to the EDL tendon in three cases (Type3, 10%) (Table 1). The median DPN_TA was significantly different according to type of relative location of DPN (Table 1).
In the side-to-side comparison, six of the 10 cadavers dissected bilaterally showed the same type of DPN location (Table 2). Also, there was no statistically significant difference of DPN_TA between both sides.
The median DPN_CP was 7.5 mm distal to the CP. However, the DPN_CP was located above the mediolateral malleolar line in only four cases. There was no statistical significance of DPN_CP according to types of DPN location.
DISCUSSION
The identification of optimal points for placement of recording and stimulating electrodes is critical for obtaining accurate results from nerve conduction studies. In cases of abnormal findings, despite precise electrode placement, anatomical variation must be considered before the neuropathy is diagnosed.
In a conventional DPN conduction study in which the CMAP amplitude is weaker after distal stimulation at the ankle than after proximal stimulation near the fibular head, the distal site should be examined for anatomical variation first, followed by suspicion of an accessory deep peroneal nerve. When present, the accessory deep peroneal nerve is a motor branch separated from the superficial peroneal nerve that travels posterior to the lateral malleolus before innervating the lateral aspect of the extensor hallucis brevis muscle. An accessory peroneal nerve has been reported to occur in 17-28% of individuals.3-5 The presence of the accessory peroneal nerve is confirmed when the CMAP of the EDB muscle is detected after electrical stimulation of the posterior aspect of the lateral malleolus.
In a previous study, the greatest CMAP amplitudes were recorded most frequently after stimulation applied 2 cm lateral to the TA tendon in 17 (46%) of 40 ankles, and after stimulation applied 1 cm lateral to the TA tendon in 27.5%.6 The greatest CMAP amplitudes were obtained when stimulation was applied precisely over the nerve. Therefore, the variety of appropriate distal stimulation sites that have been identified in the literature may be explained by the anatomical variations of individual patients. This hypothesis is supported by the variation in locations of the DPN that we observed in the present study.
The DPN contacts the anterior tibial artery above the middle of the leg and descends with the artery between the EHL and TA muscles. Needle-induced paresthesia may be occasionally encountered during needle electromyography examination for EHL muscle, despite the maximal effort at precise insertion. In this case, the needle electrode should be immediately withdrawn from the muscle. Possible causes for the unexpected event include various course of deep peroneal nerve around the EHL.
A number of anatomical studies have investigated the course of the DPN. Horwitz dissected 100 lower extremities and reported that the DPN was typically located between the EHL and EDL 2.5-5 cm above the ankle and that it divided into medial and lateral branches at the ankle.7 Lawrence and Botte dissected 17 ankle and foot specimens and reported that the DPN travels distally between the TA and EHL in the middle portion of the leg and then crosses the EHL at a point 41.0±22.5 mm proximal to the mortise.8 They also found that at a point approximately 12 mm proximal to the mortise, the DPN was typically located between the EHL and EDL. Takao et al. reported that the mean distance between the EHL and DPN at the ankle was 4.2 mm with a range of 0-11 mm in 21 DPNs from 11 cadavers.9 Along with the current study, previously published descriptions of the courses of the DPN and its branches reveal the remarkable diversity of its route and explain the difficulties faced by clinicians seeking to identify the most appropriate distal stimulation points for the deep peroneal motor nerve conduction study.
The findings of the current study indicate that the DPN is located approximately 1 cm from the TA tendon in most ankles. The discrepancy between the results of this cadaveric and our previous electrophysiologic studies6 may be attributed to the three-dimensional DPN pathway around the ankle. The distance between the TA tendon and DPN stimulation point was measured superficially in the previous study,6 whereas the distance between the TA tendon and DPN was measured in the relatively deep location in this anatomical study. Also, this difference may reflect statistical errors induced by the small sample size, which is also a limitation of our study. However, the results of both studies differ from those of previous reports suggesting that the optimal distal stimulation site for the DPN is a point just lateral to the TA tendon.
Locating the appropriate point for electrical stimulation is important as it affects not only the results of the examination but also patient comfort. Naaman et al. reported that electrical stimulation causes more discomfort when applied to muscle than when applied to nervous tissue.10 It follows that, if the point of applied stimulation departs from the nerve during conduction studies, the application of intensities more powerful than supramaximal intensity may be necessary to obtain maximal CMAP amplitude, leading to patient discomfort.
CONCLUSION
In conclusion, the results of the present cadaveric study demonstrate that the most appropriate stimulation point for use in conventional DPN conduction studies is approximately 1 cm lateral to the TA tendon at a distance of 8 cm proximal to the EDB muscle between the EHL and EDL tendons. However, if the distal CMAP is not evoked or is weaker than that elicited by proximal stimulation in individuals lacking an accessory peroneal nerve, distal stimulation should be applied to a point just lateral to the TA tendon.


 XML Download
XML Download