

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
According to a study of the medical records of Korean amputees published in 1996 in Korea on the frequency of occurrence of amputation for each area of amputation, the ratio of upper extremity amputation to lower extremity amputation was approximately 1 : 2.2 with upper extremity amputation accounting for the relatively lower proportion.1 Since prosthetic limbs for the upper extremities have technical difficulties in reproducing delicate and complex movements and the tactile and proprioceptive sensory functions of the hand and upper extremities, upper extremity amputees experience an enormous sense of frustration and problems in the rehabilitation process.2 Although prosthetic limbs have been developed and recently used in combination with electronic technologies such as myoelectric prostheses, the prosthetic limbs themselves still remain heavy, fail to reproduce precision movement functions and have a slow movement speed. Clearly, there are continuing substantial problems in the prosthetic replacement of hands.3,4
In the case of those with unilateral upper limb amputation, unlike the lower limb amputees, a relatively large number of the amputees do not use their prosthetic limb because they can compensate adequately for the in conveniences in carrying out daily activities by use of their remaining upper limb. Moreover, the majority of amputees only use their prosthesis for cosmetic reasons. They have a low level of satisfaction with its functional use and are therefore poorly motivated and reluctant to use it for this purpose and undergo rehabilitation training.5
Accordingly, this study carried out a questionnaire survey of patients, who had been prescribed upper extremity prosthetic limbs by the Center of Prosthetics and Orthotics. The purpose of this survey was to assess the actual usage of a prosthetic limb by upper extremity amputees and to determine the impacts of its use on the performance of daily living activities and levels of satisfaction. Issues related to occupation and driving after injury were also explored. Our objective was to identify changes which might be occurring over time by comparing our results with those of previous studies. An additional purpose was to provide data, which can form the basis for helping in the future development of prosthetic limbs and the rehabilitation treatment of upper extremity amputees.
MATERIALS AND METHODS
Subjects
A postal questionnaire survey was conducted with 968 amputees, who had received an upper extremity prosthetic device from the Center of Prosthetics and Orthotics in the Department of Rehabilitation Medicine at Seoul Veterans Hospital during the period January, 2000, to June, 2008. Questionnaires were returned by 344 amputees, but 37 were incomplete and excluded from the analysis. Additional exclusion criteria were cases with disabilities affecting the functioning of their lower extremityies, and those with nervous system lesions and diseases, which could affect activities of daily living or their occupation. There was no case in 307 amputees.
Composition of questionnaire
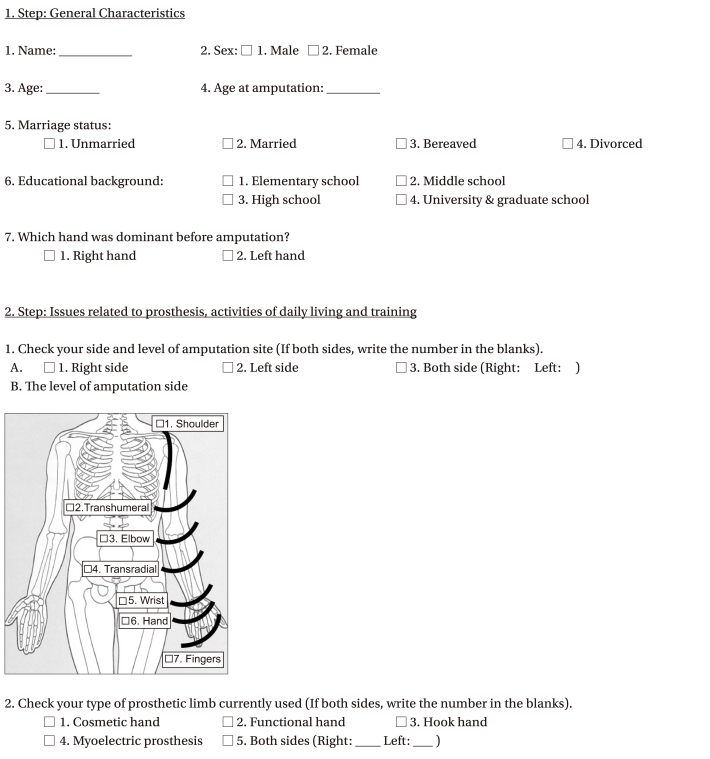
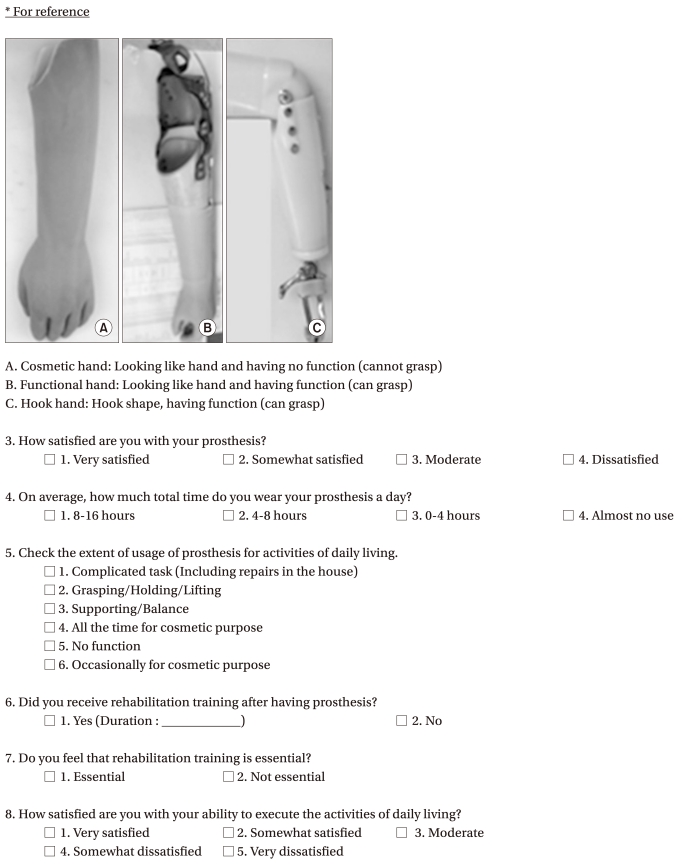
The content of the questionnaire (see Appendix) included items about the general characteristics of the respondents, questions about their prosthetic limbs, and issues related to activities of daily living, rehabilitation training, occupation and driving. More specifically, the information requested about general characteristic included gender, current age, age at the time of amputation, educational background, side of the dominant hand prior to amputation, and side and level of amputation. Questions about their prostheses included the type of prosthetic limb used most frequently, levels of satisfaction with their prosthetic limbs and the average duration of daily usage of the prosthetic limbs. Information was obtained about whether amputation was unilateral (right or left) or bilateral and about the levels of the amputation on the left and/or the right side. Pictures along with explanations were included in the questionnaire in order to assist the the respondents' understanding of the questions relating to levels of am putation and type of prosthetic limb used. If the responses to these questionnaire items were missing or inadequate, the relevant information was obtained from the medical records kept at the hospital as well as the records available at the Center of Prosthetics and Orthotics.
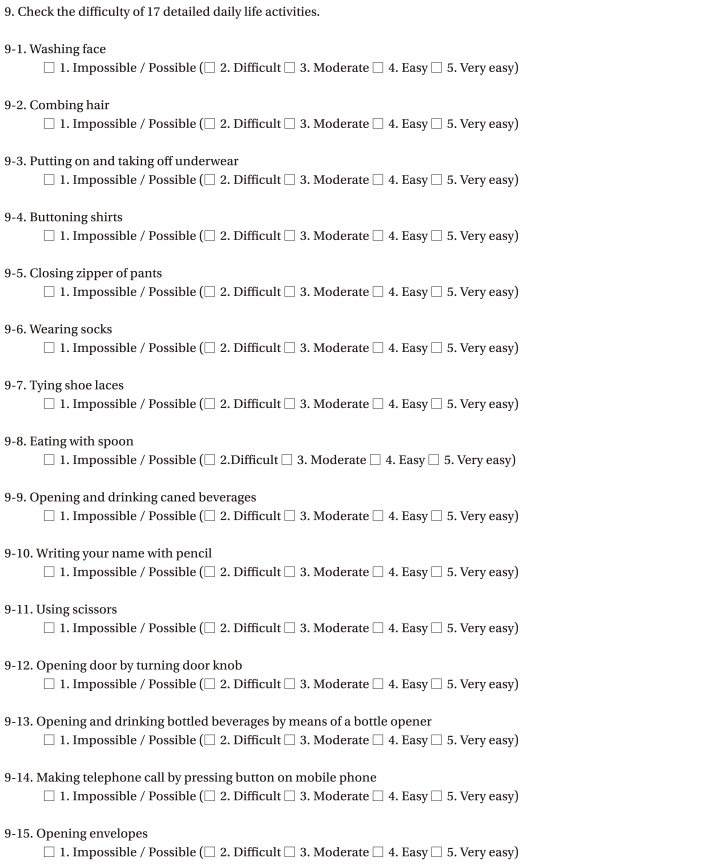
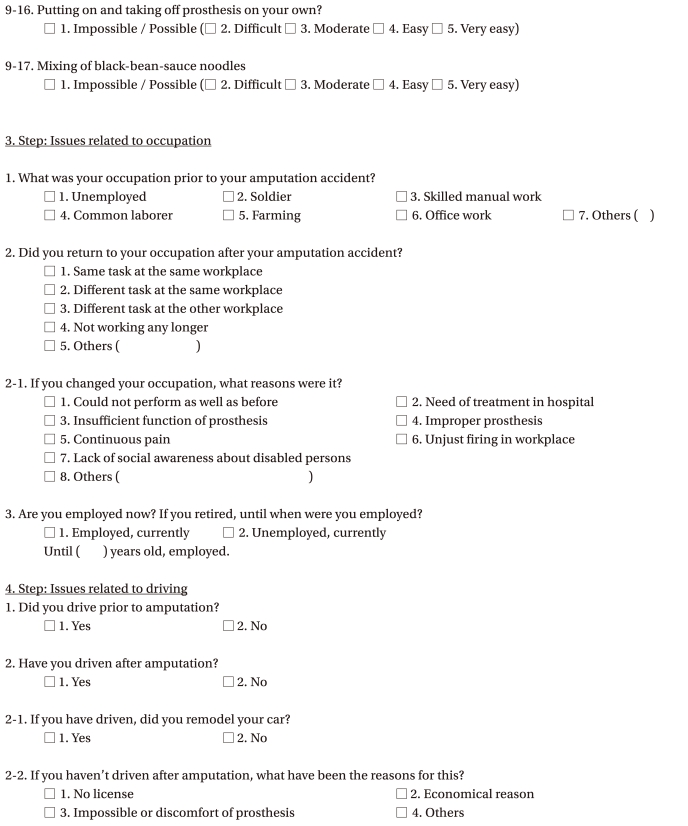
The respondents were asked whether they had received rehabilitation training after wearing their prosthetic limb and the perceived importance of the rehabilitation training. Questions were also asked about levels of satisfaction and the extent to which the amputees could perform daily living activities after receiving their prosthetic limb. A total of 17 examples of the daily living activities were included: washing face, combing hair, putting on and taking off underwear, buttoning shirts, closing zipper of pants, wearing socks, tying of shoes laces, eating with spoon, opening and drinking canned beverages, writing name with a pencil, using scissors, opening doors by turning door knobs, opening and drinking a bottled beverage using a bottle opener, making telephone calls by pressing buttons on a mobile phone, opening envelopes, putting on and taking off prosthesis without the help of another person and mixing of blackbean-sauce noodles. The questions asked whether it had been possible to perform the above tasks and, if so, the extent of the difficulties in carrying out such tasks. In reality, almost all the subjects, who said the task was possible, failed to indicate the extent of difficulty in carrying out the task. For the purpose of analysis, the subjects were therefore coded into two groups: capable and or incapable of conducting the task. For the 17 detailed items, reference was made to the list of activities associated with upper extremities used by Davidson,6 but these were modified to make them more representative of daily living in Korea. For the extent of return to their previous occupation after amputation, the amputees were asked about occupational changes and the issues, which were problematic in terms of returning to their initial occupation. For the question about whether the amputee currently has an occupation, subjects were given the opportunity to indicate whether they had ceased employment due to their age. The items related to driving inquired whether the amputee drove vehicles before and after amputation, whether the vehicle had been remodeled if amputee continued to drive, and the reasons for not driving if the amputee had ceased to drive after amputation. Finally, items were included, which related to the presence, extent and types of pain/discomfort at stump sites.
Statistical analysis
All analyses were performed with PASW Statistics 18, and statistical significance was set at p<0.05. General characteristics and issues related to prosthetic limbs were summarised with descriptive statistics and frequency counts. Pearson's chi-square test was used to analyse variables related to the usage of prosthetic limbs, rehabilitation training and driving. ANOVA and independent t-tests were conducted to examine differences in the variables related to activities of daily living and occupation.
RESULTS
Characteristics and clinical aspects of the subjects of the study
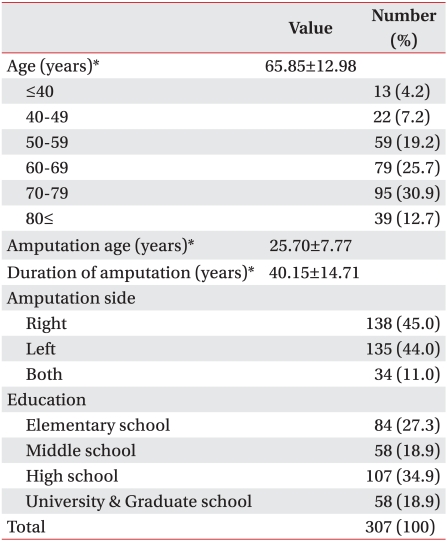
The results are summarized in Table 1. All of the 307 subjects were male and ranged in age from 27 to 88 years with a mean of 66.85 years. There were 95 subjects in their 70's (30.9%), 79 in their 60's (25.7%) and 59 in their 50's (19.2%). The mean age at the time of amputation was 25.70 years, and the mean time elapsing since the amputation was 40.15 years. In terms of educational background, 107 (34.9%) of the amputees were high school graduates. This was the largest group, followed by 84 (27.3%) with only elementary school education, 58 (18.9%) middle school graduates, and 58 (18.9%) with university or graduate school education. Among the total sample of amputees, 273 had anamputation only on one side of the body, while 34 had bilateral amputations. In the case of unilateral amputation, 150 (54.9%) subjects had damage on the dominant hand side.
Issues related to prosthetic limb
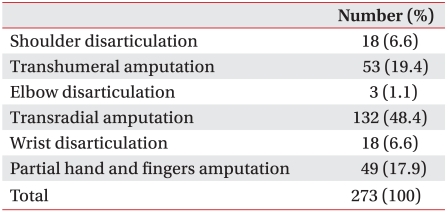
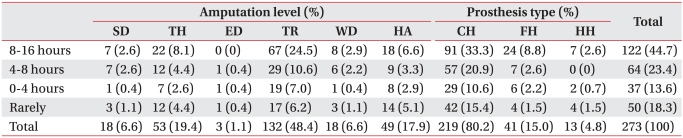
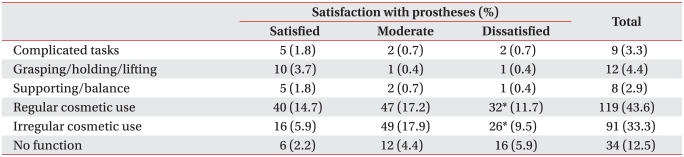
Among the 273 unilateral upper limb amputees, transradial amputation was the most frequent (n=132, 48.4%), followed by transhumeral amputation (n=53, 19.4%), partial hand and fingers amputation (n=49, 17.9%), shoulder disarticulation (n=18, 6.6%), wrist disarticulation (n=18, 6.6%) and elbow disarticulation (n=3, 1.1%) (Table 2). Among the unilateral upper limb amputees, the types of prosthetic limb currently used included cosmetic hands (n=219, 80.2%), functional hands (n=41, 15.0%), and hook hands (n=13, 4.8%). Only one amputee in the entire group surveyed (including the bilateral upper limb amputees) used a myoelectric prosthetic limb. Those with an amputation of the dominant hand were found to use functional and hook hands more frequently than those with an amputation of the non-dominant hand (p<0.05). In response to the question about the level of satisfaction with the prosthetic limb currently being used, largest number of subjects (n=113, 41.4%) reported it to be 'moderate'. The number of respondents, who reported being 'very satisfied' or 'somewhat satisfied' (n=82, 30.0%), was similar to the number, who were 'dissatisfied' (n=78, 28.6%). Differences in the degrees of satisfaction with prosthetic limbs according to the level of the amputation and type of prosthetic limb (Table 3) were not statistically significant. When the amputees were asked about the hours of daily use of their prostheses (Table 4), 122 (44.7%) subjects reported an average daily use of 8-16 hours, 64 (23.4%) answered 4-8 hours, and 37 (13.6%) used their prostheses for less than 4 hours. A group of 50 (18.3%) subjects indicated almost no use. There were no significant differences in the reported average duration of daily use of prosthetic limbs by level of amputation or by type of prosthetic limb.
Activities of daily living and rehabilitation training
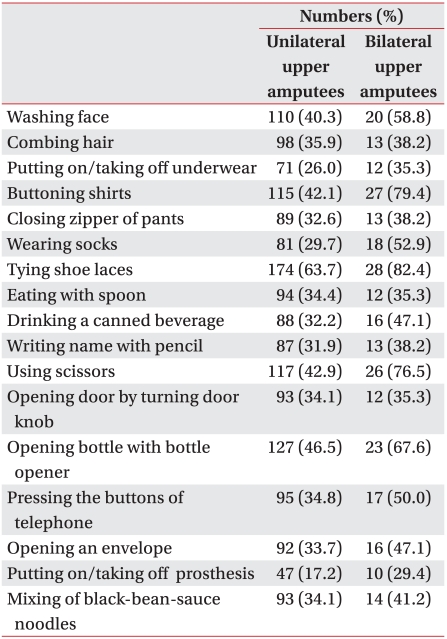
While only 20 (7.3%) of the unilateral amputees reported receiving rehabilitation training after being given a prosthetic limb, 59 (21.6%) responded that they felt rehabilitation training is essential. Although the group who received rehabilitation training was more aware of the importance of rehabilitation training (p<0.001), there were no significant clinical differences between the groups who and had not felt the need for rehabilitation training. On the question of the extent of usage of a prosthetic limb for the upper extremity in activities of daily living (Table 5), 9 (3.3%) subjects responded that they were able to perform complicated tasks, including repairs in the house, 12 (4.4%) reported that they could hold and lift objects, 8 (2.9%) responded they could hold onto their surroundings to prevent falling, 119 (43.6%) indicated that used their prosthetic limbs all the time for cosmetic purposes, 91 (33.3%) responded that they wore their prosthetic limbs occasionally for cosmetic purposes when going out, and 34 (12.5%) stated that their prosthetic limbs did not provide any functional assistance. A total of 210 (76.9%) subjects responded that they used their prosthetic limbs all the time or occasionally for cosmetic purposes. The amputees using prostheses for cosmetic purposes were not statistically different from those using them for functional purposes in terms of the type of prosthesis, average duration of daily usage of prosthetic limb, or level of amputation, but they did report a lower level of satisfaction with their prosthetic limbs (p<0.05). On the question of level of satisfaction with activities of daily living which they performed without the help of others, 7 (2.6%) subjects were highly satisfied, 57 (20.9%) were somewhat satisfied, 121 (44.3%) moderate, 36 (13.2%) were somewhat dissatisfied, and 52 (19.0%) were highly dissatisfied. There were no significant differences in the levels of satisfaction about the execution of activities of daily living according to the level of amputation or the type of prosthetic limb. Turning to difficulties encountered in performing the 17 detailed daily life activities, the most difficult tasks for the unilateral upper limb amputees were tying shoe laces (63.7%), opening and drinking a bottled beverage with a bottle opener (46.5%), using scissors (42.9%), and buttoning shirts (42.1%) (Table 6). The cosmetic and functional hand groups found tying shoe laces to be most difficult, while the hook hand group found that opening and drinking a bottled beverage with a bottle opener was the hardest task. In terms of level of amputation, the most difficult task for those with shoulder disarticulation, transhumeral or transradial amputation was tying shoe laces, for those with wrist disarticulation it was using scissors, and for those with partial hand and fingers amputation it was buttoning shirts.
Issues related to occupation and driving
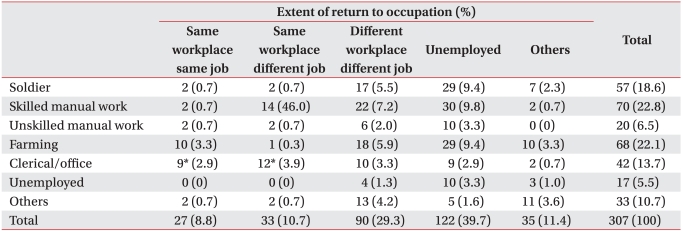
On the question of occupation before and after the upper extremity amputation for all the amputees (Table 7), before their amputations 70 (22.8%) subjects had been doing skilled manual work, 68 (21.5%) were in farming, 57 (18.6%) were in the military, and 42 (13.7%) had been office or clerical workers. After their amputations, 122 (39.7%) subjects could not work any longer, while 90 (29.3%) subjects worked at another workplace, 33 (10.7%) performed different tasks at the same workplace, and 27 (8.8%) performed the same tasks at the same work place. Although there were no statistically significant differences in the extent of return to their previous occupations in terms of the different types of prosthetic limb and different levels of amputation, there was tendency for a better extent of return to the original occupation in those with an amputation at a distal site than in those with an amputation was at a proximal site. Although there seemed to be no difference in the extent of return to the previous occupation according to whether or not the amputation was in dominant hand, the extent of return was found to be better for those working in offices than for military personnel, skilled manual workers or common laborers (p<0.05). In addition, those, who had been employed in farming, skilled manual work and common laboring prior to amputation, felt a greater need for rehabilitation training than those in the other occupational groups (p<0.05). On the question of reasons for not being able to return to their occupation following amputation, 143 (51.6%) subjects responded that they could not perform as well as before. The other reasons given (in order of descending frequency) were insufficient function of prosthetic limb (n=45, 16.2%), lack of social awareness about disabled persons (n=32, 11.6%), and continuous pain (n=15, 5.4%). In response to the questions about driving, 62 (20.2%) of all the subjects (unilateral and bilateral amputees) reported they drove prior to amputation. After amputation, 126 subjects (41.0%) stated that they drove, and 34 (26.9%) of this group said that their automobile had been remodeled. On the question of the reasons for not driving after amputation, the largest number of respondents (n=85, 47.0%) answered that they did not drive even before amputation. The next most frequent reason given was that driving with a prosthetic limb is uncomfortable (n=52, 28.7%). Although there were no differences according to side of amputation or type of prosthetic limb between the group which was driving after amputation and the group that was not , those with a more distal site of amputation were more likely to be driving (p=0.001) (for data, see Table 8).
Pain and discomfort experienced by amputees
Amongst all the subjects, 83 (27.0%) respondents reported experiencing pain or discomfort all the time, while 132 (43.0%) reported occasional pain. A group of 38 (12.4%) amputees indicated that the pain occurred when using their prosthetic limbs. On the issue of the types of symptoms related to pain and discomfort, 167 (54.4%) of the subjects complained of tingling at the amputation site, 112 (36.5%) reported pain at the stump, 93 (30.3%) complained of phantom pain, 65 subjects (21.2%) mentioned itching at the amputation site, and 43 (14.1%) reported paresthesia at the amputation site.
Characteristics of bilateral upper limb amputees
Transradial amputation on both sides was the most frequent (n=20, 58.5%) form of bilateral upper limb amputation, and the functional and hook hands were the most frequently used types of prosthetic limb, accounting for 20.6% and 41.2% of the bilateral upper limb amputees, respectively. Functional prosthetic limbs were statistically more frequent in the bilateral upper limb amputees than in the unilateral amputees (p<0.001). On the question of level of satisfaction with the currently used prosthetic limb, 13 (38.2%) subjects responded that they were 'moderate', while 12 (35.3%) were 'satisfied' and 9 (26.5%) were 'dissatisfied'. Most (n=23, 67.6%) used prosthetic limbs for an average of 8-16 hours a day, 4 (11.8%) for 4-8 hours, 3 (8.8%) for less than 4 hours, and 4 (11.8%) hardly ever used them. There were no significant differences between unilateral and bilateral amputees in levels of satisfaction or in average daily durations of use. However, on the question of the extent of usage of a prosthetic limb for daily life activities, 54.5% of the bilateral amputees responded that the prostheses were functionally helpful; this was significantly higher than the corresponding figure for unilateral amputees (p<0.001). In terms of the 17 detailed activities of daily living, the most difficult tasks for the bilateral amputees were (in the order of descending frequency) tying shoe laces (82.4%), buttoning shirts (79.4%), using scissors (76.5%), opening and drinking a bottled beverage with a bottle opener (67.6%), and washing one's face (58.8%) (Table 5). On the question of the extent of return to previous occupation after the amputations, 29 subjects (85.3%), could not return to work, while 5 (14.7%) worked on different tasks at a different workplace. Clearly, none of the bilateral amputees returned to the same workplace or performed the same tasks.
DISCUSSION
The severing of a part of the human body not only causes functional and psychological disability but also induces social isolation.2 Although enormous efforts have been made in an attempt to overcome these difficulties, the majority of these attempts have been focused on lower extremity amputation.7 Moreover, in the case of unilateral upper limb amputees, most consider a prosthetic limb has an only supplementary role since most of the activities of daily living are conducted by using the upper extremity on the intact side.8,9 Since the level of expectations about prosthetic limbs differs widely and the frequency of upper extremity amputation is lower than that of lower extremity amputation, reports on the actual status of prosthesis usage of upper extremity amputees in Korea remain inadequate.
In the previous research by Song and Park,5 the frequency of amputation level was highest for transradial amputation at 51.9%, followed by 32.8% for transhumeral amputation and 8.2% for shoulder disarticulation. In assessing the cause of amputation, they found high proportions of shrapnel and gunshot injuries (67.9% and 16.8%, respectively). In this study, although the frequency of transradial amputation was the highest, accounting for 48.4% of the unilateral upper limb amputees, the frequencies of transhumeral amputation and shoulder disarticulation (19.4% and 6.6%, respectively) were less than those previously reported, and the frequencies of partial hand and fingers amputation and wrist disarticulation (17.9% and 6.6%, respectively in the two studies) were, higher. Although it is not possible to perform accurate analysis since no assessment of the causes of amputation was made in the present study, these results, when compared with those of the earlier research findings, indicate causes such as shrapnel injury, gunshot injury and damage from explosions, which damage proximal sites of the upper extremity, are decreasing, and that mechanical and electrical causes arising from industrialization, which bring about damage to the distal sites, are increasing.1
In the research reported by Wright et al.10 and Durance and O'Shea,11 the frequencies of the use of functional prosthetic limbs were quite high (84% and 77%, respectively in the two studies). However, previous reports in Korea, which studied the types of prosthetic limb used for the upper extremities, found lower frequencies of functional prosthetic and cosmetic prosthetic limbs (62.5% and 55.5%, respectively, of all the prosthetic limbs for upper extremities.2,8 Moreover, the frequency of cosmetic prosthetic limbs accounted for 79.8% of the total, which is substantially higher than that of functional prosthetic limbs at 1.5%, even in the research by Song and Park.5 In the present study, although the usage of a functional prosthetic limb increased to 15.0%, it was found that 80.2% of the unilateral upper limb amputees are using a cosmetic prosthetic limb. Such findings are believed to be the results of the very low frequency of those receiving rehabilitation training in the usage of a prosthetic limb (7.3%), the majority of the questionnaire respondents being old and familiar only with the prosthetic limb, which was prescribed for them in the past (40.15 years was the mean time since the of amputation) and therefore not having attempted to try a new functional prosthetic limb, and the substantially significant burden of manipulation and adaptation to a functional prosthetic limb.
On the question of the level of satisfaction with a prosthetic limb, the frequency of those reporting it as 'satisfactory' was 30.0%, which is slightly higher than the proportion found in the research by Song and Park,5 but proportion of those who were found to be 'dissatisfied' was still very high at 28.6%. However, 44.7% of unilateral upper limb amputees in the present study reported wearing their prosthetic limbs for an average of 8-16 hours per day. Gaine et al,12 considered that the wearing of prosthetic limb for a daily average of eight hours or more indicated success in the usage of a prosthetic limb and devised a prosthetic success score for which the duration of wearing of prosthetic limb was one of the component scores. The results of the present study demon strate an increase in the daily duration of wearing a prosthesis when compared with the 39.2%, who stated that they always wore their prosthesis, in the study by Song and Park.5 Nevertheless, the present study found that the level of amputation and types of prosthetic limb made no difference to levels of satisfaction or durations of wearing a prosthesis. Moreover, the extent of usage also appeared to be unaffected by the level of amputation and types of prosthetic limb. Most (76.9%) of the unilateral upper limb amputees reported using their prosthetic limb always or occasionally for cosmetic purposes, and this group's the level of satisfaction with their prosthetic was lower than that of the group using their prostheses for functional purposes.
On the questions about 17 detailed activities of daily living, tasks such as tying shoe laces, opening and drinking a bottled beverage with a bottle opener, using scissors and buttoning shirts were found to be more difficult than other activities. In general, there was a tendency for activities to be more difficult to perform, if they required delicate movements and substantial force of the distal extremities. In particular, for those with amputation of the hand or fingers, activities which required delicate movements of the terminal ends of the upper extremities, such as buttoning shirts and using scissors, tended to be more difficult. By adding and examining detailed tasks to the basic activities of daily living, it is thought that the results of the present study will provide information to assist in the development of rehabilitation training programs for upper extremity amputees.
Most of the respondents in the present survey stated that after amputation they were either unemployed or performed different tasks at different workplaces (39.7% and 29.3%, respectively), and only 8.8% returned to the same task at the same workplace. While this is an increase from the 5.5% reported by Chang et al.8, it is still substantially lower than the occupation return rate of 30.4% reported in the research by Gaine et al.12 In addition, it was confirmed that there was no case of a return to the original workplace amongst the bilateral upper limb amputees. Considering the fact that amputation occurred at the average age of 25.70 years and that this age represents a productive stage in people's lives when they have substantial socio-economic capabilities, the socio-economic losses arising from amputation are believed to be enormous. As was the case in the previous researches,13 the results of the present study showed that the extent of return to an occupation was unrelated either to whether the dominant upper extremity was amputated or to the educational background of the amputee. Office workers experience less demand on the functioning of their upper extremities and the extent of their return to their previous occupation was found to be better than for military personnel, skilled manual workers and common laborers. In addition, farmers, skilled manual workers and common laborers, who face greater demands on the functioning of their upper extremities, see rehabilitation training more as more important than others do. On the question of the reasons for failure to return to ones' previous occupation, although an inability to perform as in the past accounted for 51.6% of the answers, many gave reasons such as insufficient functions of a prosthetic limb (16.2%) and lack of social awareness about disabled persons (11.6%). This illustrates that the social awareness about amputees or systems related to occupation rehabilitation is still insufficient. The development of prosthetic limb with faster and more accurate movement functions is also needed.
According to Davidson,6 68% of upper extremity amputees drove vehicles after amputation, with 73% of drivers using handle rotation knobs and 23% having extended winker levers. In the present study, 41.0% of all the amputees stated that they drove after amputation, with 26.9% of them using remodeled automobiles. The subjects were not asked to provide details of types of remodeling, and this makes accurate comparisons difficult, but the proportions of the drivers and the remodeling of automobiles were found to be relatively lower. Moreover, although there were no differences in the side of amputation and types of prosthetic limb between those who did and did not drive after amputation, the drivers and non-drivers were found to differ in terms of the level of the amputation. A statistically larger number of amputees drove if the level of amputation was closer to the distal site. Under the current domestic road and traffic laws of Korea, those, who have lost both arms above the elbow, or those, who are unable to use both arms at all, are not allowed to drive. However, there is exception for the cases in which such people are able to drive normally by using automobiles, which have been designed and built to suitably accommodate for the extent of the physical disabilities of the amputee driver. If rehabilitation services for driving, such as the development and supply of assistive devices appropriate for driving, are improved and if there is an expansion of rehabilitation centers for driving, then the proportion of upper limb amputees who drive will increase. This should improve their activities of daily living and also increase their satisfaction levels with their prosthetic limbs.
This study is limited in the extent to which the results can be generalized to everyone with upper extremity amputations, since subjects included only the patients who were prescribed prosthetic limbs for their upper extremities at a single hospital; furthermore, all the subjects were male and elderly. A second limitation is the study relied upon a postal questionnaire survey for the collection of data, and more detailed and useful information could have been obtained from the amputees by the use of personal interviews.
However, this study is meaningful in comparison to the previous researches in that it investigated a range of issues, including levels of satisfaction, the actual status of usage of a prosthetic limb for the upper extremities, activities of daily living, and the impacts on occupations and driving. It is believed that the findings of this study could be used in the future as basic information for the prescription and training for use of upper extremity prosthetic limbs and for rehabilitation training in relation to returning to employment.
CONCLUSION
This study used a postal questionnaire survey of patients with upper extremity amputations to investigate their current use of prosthetic limbs and levels of satisfaction in relation to their activities of daily living, occupation and driving. Although the extent of return to previous employment is considered to be improving, it is still highly unsatisfactory when compared with data from overseas countries. Moreover, it seems that a prosthetic limb for the upper extremities has greater significance for cosmetic and supplementary purposes than functional purposes. Finally, there appears to be a need for: firstly, the development of prosthetic limbs with functions more closely approximating the normal functions of the upper extremities; secondly, changes in social awareness about the amputees; and, thirdly, the establishment of policies designed to improve occupational rehabilitation.


 XML Download
XML Download