

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Degenerative arthritis of the knee is the type of arthritis which most commonly occurs in the elderly, and the increasing prevalence of degenerative arthritis of the knee in the rapidly increasing elderly population in Korea has become a new issue of concern.1,2 Until now, an accurate prevalence rate for degenerative arthritis of the knee in Korea has not been measured, but the high prevalence rate for degenerative arthritis of the knee could be calculated the basis of recently conducted studies conducted in certain regions of Korea. Cho et al.1 reported that 38.1% of adults over age 65 residing in Seongnam-Si, Gyeonggi province have radiologically diagnosed degenerative knee osteoarthritis, and Kim et al.2 reported that 37.3% of adults over age 50 residing in Chuncheon-Si, Gangwon province have radiologically diagnosed degenerative knee osteoarthritis.
This degenerative arthritis of the knee often accompanies severe pain in knee joints and results in disorder in daily living activities related to ascending the stairs, hunkering down, standing up from a chair, etc.3 However degenerative arthritis of the knee is a disease that spreads slowly, and if proper treatment is conducted upon early detection, the need for surgical treatment can be delayed.4 Therefore, the conservative treatment approach is very important in degenerative arthritis of the knee, and Osteoarthritis Research Society International (OARSI) and European League Against Rheumatism (EULAR) emphasized the importance of the non-pharmacological treatment approach among conservative treatments.5 For knee osteoarthritis, conservative treatments include braces, insoles, exercises, diet, and patient education. Their common goal is modification of the load applied to the part of the knee affected by degenerative arthritis.
Degenerative arthritis of the knee occurs mainly in the medial compartment of knee joints,6,7 and as an external device to reduce the load concentrated to the medial compartment, the laterally wedged insole and the off-loading knee brace are widely used. The laterally wedged insole is an aid attached to the hindfoot of heel inserts and plays the role to decrease the knee varus moment in the stance phase of patients with degenerative arthritis of the knee. Marks and Penton8 reported that after using the laterally wedged insole for patients suffering from medial compartment degenerative arthritis of the knee, the pain in knee joints decreased significantly, but Pham et al.9 argued that the decrease in pain could rather have resulted from intake of the NSAID drugs after using the laterally wedged insole. However, according to the study of Baker et al.,10 the effects of the laterally wedged insole were insignificant in patients of medial compartment degenerative arthritis of the knee, and Hinman et al.11 said that no significant change of the knee adduction moment was seen even though the laterally wedged insole was used continuously for one month. Based on these studies, the medical effects of the laterally wedged insole are still controvertible.
However, many studies with on patients with unilateral degenerative arthritis of the knee report decrease of pain, increase of muscular strength and improvement in daily living activities after using the off-loading knee brace.12-15 In addition, the effects of the external moment of the brace that increase the weight load to the affected leg during the stance phase by reducing the pain of knee joints at the time of walking, and increase the speed of walking by reducing the imbalance of the step length with the non-affected leg, were reported.16 In these instances, as the effects of the off-loading knee brace decrease knee joint pain by reducing the load from the medial compartment of narrowed knee cartilage, the demand for the off-loading knee brace is on the rise in Korea.
So far, most published examinations related to the off-loading knee brace focused on the mechanical effects of the brace such as the proof of the decrease of pressure of the medial compartment of knee joints and the resulting short-term changes, but there is no study on the changes of muscle activation around the femoral region following the use of the brace and related problems. This study intended to examine what changes are caused in the activity of the muscles around the femoral region at the time of squatting and walking in normal adults by using the Kneelove2® (Davinci Meditec, Wonju, Korea) which is the off-loading knee brace model developed in Korea, and thereby predict whether the muscular strength of the muscles around the femoral region is weakened following the long-term wearing of the brace and to examine the necessity for provision of this model or the development of a new brace.
Go to : 
MATERIALS AND METHODS
Subject of the study
This study was conducted with 10 volunteers who were healthy male adults without knee joint pain, medical history of knee joint surgery or any other musculoskeletal disorder. The range of motion of knee joints of all subjects was normal, and the muscular strength of both legs was normal on the manual muscle testing. The Q-angle of the subjects was observed to be in the normal range in both legs. Participants who agreed to volunteer signed appropriate consent forms and the average age of the participants was 26.6±1.3 (26-30). The dominant leg was determined after the evaluation of the execution ability of simple exercises such as kicking a ball,17 and the dominant leg was the right leg in 9 subjects and was the left leg in 1 (Table 1).

Method of the study
Exercise program
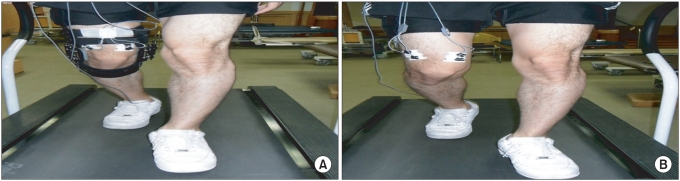
The exercise program was composed of squatting and walking and was conducted in the following order. First, squatting began from a neutral position with the feet shoulder width apart and then bending at the knee joints to up to 90 degrees with the back straightened and the arms stretched forward. At this position, the heights of the apex of patella and the gluteal fold were measured, while fixed bars were established with rubber bands at the point that comes under the respective heights (Fig. 1). Afterwards, to confirm the correct position at the time of squatting, the angle of knee joints bent at 90 degrees when the apex of patella and the gluteal fold respectively coincided with the height of the their fixed bars was checked. Squatting was performed after conducting sufficient education and training so that the subjects would be acclimated to the test method prior to test commencement, and sitting and standing up were repeated 10 times with intervals of 1.5 seconds using a metronome. After a sufficient rest of 5 minutes, Kneelove2® was worn on the dominant leg, and squatting was conducted according to the same method. Next, walking on a treadmill was conducted after proper training was given. Walking was conducted for 1 minute at a low speed (3 km/h) and for 1 minute at a high speed (6 km/h). After a sufficient rest of 5 minutes, Kneelove2® was worn on the dominant leg and walking was conducted in the same manner (Fig. 2).

Measurement of electromyographic signal
The surface electromyographic signals of the VMO, VL and BF were collected by using TeleMyo 2400T dynamic electromyography (Noraxon Inc., Arizona, USA). The skin over the bellies of these muscles were wiped with alcohol in order to reduce skin resistance, and the surface electrode (Bioprotech Inc., Wonju, Korea) composed of disposable silver/silver chloride coated with adhesive substances was attached in the parallel direction of fibers of the VMO, VL and BF of the dominant leg (Table 2).18 The surface electrode was attached prior to the start of the exercise program, and was maintained on the same are until the completion of the entire exercise program. In terms of squatting and walking, the electromyographic signals were digitized by using dynamic electromyography, and the sampling frequency was set at 1,500 HZ and was stored in the computer.

Measurement of the maximum isometric contraction of the muscles around the femoral region
After attaching the surface electrode to each muscle, Contrex® isokinetic dynamometer (CMV AG, Dubendorf, Switzerland) which is an isokinetic exercise machine was used in order to measure the maximal voluntary isometric contraction (MVIC) of the muscles of the femoral region. The subjects sat on the chair of the dynamometer completely snug to the back of the chair by using a 3-point belt and aligned the knee joint axis of the legs on which the test was executed with the exercise axis of the machine, fixed the femoral region with a velcro strap, and fixed the upper part of two malleoli with a resistance pad. The knee joints of the leg on which the test was not executed were fixed on the front side of the upper part of two malleoli with a stability bar at the bending position. During the test, both hands were allowed to hold the fixed handle, and the hip joint and the knee joints were flexed by 90 degrees and 45 degrees respectively, while the angle of the ankle joints was not controlled. The test was conducted in the described order, and the maximum isometric extension strength of knee joints was measured for 5 seconds, and after taking a 5 minute rest, the maximum isometric flexion strength was measured for 5 seconds. The medium 3 seconds excluding the first and the last second from the value obtained during the 5 seconds were selected for analysis of MVIC. During the maximum isometric extension, the average value of the root mean square (RMS) of the VMO and the VL was measured, and during the maximum isometric flexion, the average value of the RMS of the BF was measured and those were taken as the MVIC of each muscle. This means a muscular activity of 100% was used as the standard value of the activity of each muscle (Fig. 3).

Analysis of muscular activity
During the exercise program, the activity of each muscle was stored in the computer as data. The stored electromyographic signals went through a dual-pass filter process using the Butterworth filter plus a Band-pass of 15 through 350 Hz by using the built-in MyoResearch XP master Edition 1.06 (Noraxon Inc., Arizona, USA), and went through the full wave rectification process upon which the average value of RMS was obtained. The used window length was set at 125 msec.
At the time of squatting, a video was filmed with a PC camcorder (Samsung electronics Inc., Seoul, Korea) in order to distinguish the movements of flexion and extension of knee joints. The classification into the knee joints flexion period and extension period of squatting was conducted by using the electromyographic data combined with the synchronized video, while the activity of each muscle was used as the average RMS value. The activity of each muscle was standardized as the percentage of MVIC to the value of RMS and was indicated as the ratio to the maximum muscular strength value (%MVIC).
In walking, the foot contact sensor switch (Noraxon Inc., Arizona, USA) was attached to the first metatarsal head of each foot and heel, and was synchronized with the electromyographic data where the stance and swing phases were distinguished in the walking cycle. At the time of walking, the activity of each muscle was converted into the average value of RMS during the stance phase and swing phase and later indicated as the ratio to the maximum muscular strength value (%MVIC).
Statistical analysis
For statistical analysis, SPSS 12.0K was used. The degree of activation of the muscles around the femoral region following the before and after of wearing the brace was analyzed by using the Wilcoxon signed-rank test in order to compare the impact of the knee brace on the muscles around the femoral region during squatting and walking, and p<0.05 was considered statistically significant.
Go to :
RESULTS
Comparison of the muscular activity before and after wearing the knee brace in squatting
In the extension period, the activity of the VMO before and after wearing the knee brace was measured as 43.30±8.5% and 36.92±5.7% respectively, and in the flexion period, the activity of the VMO before and after wearing the keen brace was measured as 43.99±11.07% and 35.91±9.9% respectively (Fig. 4). In both the extension and the flexion periods, at the time of wearing the knee brace, all activities of the VMO, VL and BF showed a decreasing trend, however there was a significant difference in only the VMO (p<0.05), while there was no statistical difference in the VL and BF.
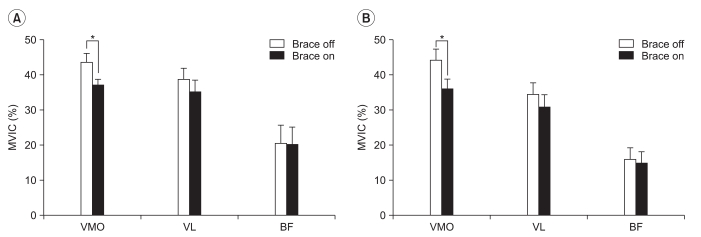 | Fig. 4The changes of electromyographic activities expressed as percentage of maximal voluntary isometric contraction of the VMO, VL and BF muscles during squatting exercise. (A) extension phase, (B) flexion phase. VMO: Vastus medialis oblique, VL: Vastus lateralis, BF: Biceps femoris, MVIC (%): Percentage of maximal voluntary isometric contraction; *p<0.05.
|
Comparison of the degree of muscle activation before and after using the knee brace in slow walking
In the stance phase, the activity of the muscles around the knee joints showed an increasing trend in each VMO, VL and BF after wearing the knee brace but there was no significant difference (Fig. 5). In the swing phase, the muscles around the knee joints showed a decreasing trend in activity in the VMO and increasing activity in the VL and BF after wearing the knee brace, but there was no significant difference.
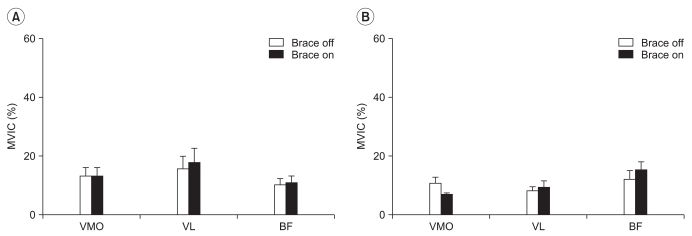 | Fig. 5The changes of electromyographic activities (expressed as percentage of maximal voluntary isometric contraction) of VMO, VL and BF muscles during slow walking exercise. (A) stance phase, (B) swing phase. VMO: Vastus medialis obique VL: Vastus lateralis BF: Biceps femoris, MVIC (%): percentage of maximal voluntary isometric contraction; *p<0.05.
|
Comparison the before and after of using the brace in fast walking
The activity of the VMO in the stance phase before and after wearing the knee brace was measured as 44.08±12.6% and 32.09±14.2% respectively, and the activity of the VMO in the swing phase was measured as 23.10±1.0% and 13.15±5.4% respectively. After wearing the knee brace, in both the stance phase and swing phase, the activity of the VMO and VL showed a decreasing trend and the activity of the BF showed an increasing trend, but a statistically significant difference was apparent in the VMO only (p<0.05) (Fig. 6).
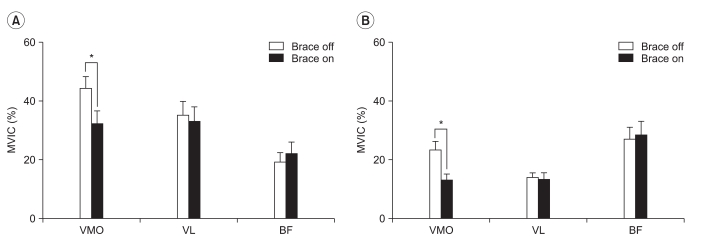 | Fig. 6The changes of electromyographic activities expressed as percentage of maximal voluntary isometric contraction of VMO, VL and BF muscles during fast walking exercise. (A) stance phase, (B) swing phase. VMO: Vastus medialis obique VL: Vastus lateralis BF: Biceps femoris, MVIC (%): percentage of maximal voluntary isometric contraction; *p<0.05.
|
Go to :
DISCUSSION
In stance phase, excluding the moment immediately after the initial contact in which the valgus moment occurs, the varus moment occurs and the load experienced primarily goes through the medial compartment of the knee joint.19 In walking, the load disperses through the medial compartment of knee joint causing continuous friction of the articular cartilage of the medial compartment, thus promoting degenerative arthritis of the knee comes. In addition, in patients suffering from medial compartment degenerative arthritis of the knee occurring on the unilateral side, genu varum occur together with the degenerative changes of the medial articular cartilage, and as the side comes to receive the varus moment which is relatively excessive compared with the normal side, the degeneration is further promoted,20,21 and the pain grows increasingly severe.
The off-loading knee brace was designed to reduce the load to the medial compartment of knee joints by generating the external valgus moment in the knee joints, and upon usage the improvement of pain and function was reported. According to Matsuno et al.14, in patients with serious medial compartment degenerative arthritis of the knee, after wearing the off-loading knee brace for 12 months, the decrease of pain, the decrease of the angle between the femur and tibia, and the increase of the isokinetic muscular strength of the quadriceps muscle of thigh were observed. According to Dennis et al.12, in patients that expereinced major medial compartment degenerative arthritis of the knee, walking on a treadmill before and after wearing the off-loading knee brace was analyzed with fluoroscopy, where the group reported the decrease of pain and the widening of the distance between the medial compartment of the knee joints after using the brace. In addition, Pollo et al.15 confirmed that after using the off-loading knee brace, the pain decreased and the intensity of activity increased, and as the valgus moment functioning in the outside of knee joints grew larger, the load to the medial compartment of knee joints decreased. These studies collectively demonstrate that the off-loading knee brace increases the space of the medial compartment of knee joints and effectively reduces the load to the medial compartment.
However, in spite of these effects that the use of the brace can cause long term muscle of the femoral region by leading to decreased activity of the muscles is recognized as a potential problem. Yet studies on the varying degree of changes of activity as related to specific muscles at the time of exercise are actually incomplete. In this study we observed the activity of the muscles around knee joints while the off-loading knee brace was worn or not worn in squatting as well as slow and fast walking exercises. As a result of the study, after wearing the brace, in squatting and fast walking conditions the activity of the VMO significantly decreased, but, during slow walking no change of the activity of the VMO was observed. On the basis of these results, we determined that in specific exercises such as squatting and fast walking, the off-loading knee brace has a significant impact on the activation of the VMO among the muscles of the femoral region.
The quadriceps muscle of the thigh is in charge of functions such as extension of the knee joints, maintenance of the stability of knee joints, absorption of shock, proprioceptive sense and so on. In degenerative arthritis of the knee the weakening of the thigh quadriceps muscle commonly occurs and is one of the symptoms that patients report early on and is said to reflect that the level of pain experience is better detected in comparison to radiologic detection of degenerative changes.22 According to Slemenda et al.,23 in the patients with degenerative arthritis of the knee, even though there is no pain in the knee joints and no muscular atrophy, the weakening of the quadriceps muscle of the thigh can be observed. Also the degree of degenerative progress of the arthritis of the knee and the pain could be predicted by the degree of weakening of the thigh quadriceps muscle. These results prove that the weakening of the thigh quadriceps muscle can occur before the damage of joints by degenerative changes. In addition, the functional disorder of the quadriceps muscle of the thigh causes the weakening of muscular strength, decrease of voluntary activities, increase of fatigue, decrease of the minuteness of the proprioceptive sense, decrease of the neuromuscular protective mechanism, instability of functional joints, instability of posture and so on.22 Finally, the progress of degenerative arthritis of the knee causes a decrease in general daily living activities, the decrease of cardiopulmonary functional capacity and the deterioration of quality of life.
The role of the VMO among the thigh quadriceps muscle is mainly reported in the studies on the patellofemoral pain syndrome, where the weakening of the VMO causes the malalignment of the patella and abnormal lateral displacement.24 In addition, another study reported that the VMO is not a muscle that simply has the function of extension of knee joints but rather it shows a tendency of being activated in the case of movements that destabilize the knee joints.25 Based on these findings, this study investigated scenarios that included squatting, and within this the physical load concentrated to the knee joints and considerable stress comes to be given to the quadriceps muscle of the thigh. During squatting, the excessive load concentrated to the knee joints caused lateral tilting of the patella due to the normal Q-angle, and after wearing the brace, an external valgus moment occurred to the knee joints and the Q-angle comes to decrease.5,14 In addition, it is interpreted that the decreased Q-angle reduces the lateral tilting of the patella and thereby decreases the activity of the VMO. Therefore it is thought that at the time of squatting if one wears the brace, the external valgus moment occurs, the lateral tilting of the patella decreases, and thus the activity of the VMO decreases significantly. Moreover, in view of the decrease of VMO activity in both the extension period and the flexion period of the knee joints in squatting, the valgus moment maintained continuously during the squatting supported by a brace.
According to Perry and Burnfield26 in men who are 20 to 59 years old, the average of slow walking and the average of fast walking were measured as 37 m/min and 99 m/min respectively, and the speed of functional walking was measured as 40 through 100 m/min. When the speed of walking increases to that of running, compared with walking, the pattern of the activity of the quadriceps muscle of the thigh is similar, except the VMO and the VL are the most activated. Among those, the activity of the VMO is the highest, and the activity increases up to 3 times. The activity of the VMO and the VL increases since these muscles play a role in stabilizing the patella to the trochlear groove, and if there is no activation of the quadriceps muscle of the thigh, the knee joints will not be able to withstand the load and will buckle. This study distinguished the low speed as 3 km/h (50 m/min) and the high speed as 6 km/h (100 m/min). We intended to examine the impact of the off-loading knee brace on the activation of the quadriceps muscle of thigh and the BF following the walking speed.
We observed that in the case of fast walking, after using the brace the activity of the VMO increased significantly, but in the case of slow walking, the change of the activity of the VMO was not significant. This result demonstrates that the external moment by the brace primarily functions effectively during fast walking. As the walking speed increases normally the activity of the VMO increases to reduce lateral tilting of the patella,26 and it is thought that while wearing the brace, the external moment occurs and stabilizes the patella to the trochlear groove and thereby the activation of the VMO decreases significantly.5,14 In addition, before and after wearing the brace during the slow walking, the change of the VMO activity was decreased the slow walking could maintain the knee joints more stable than the fast walking.
Moreover, we were able to see that during fast walking, after using the brace, the activity of the VMO significantly decreased not only in the stance phase but also in the swing phase. In general, during normal walking, the activity of the vastus muscle group begins from the terminal swing and reaches its peak at the loading response of the stance phase and after the mid stance decreases slowly, coming to a stop. Particularly during the terminal swing, the activation of the vastus muscle group has activated for the maximum extension of knee joints and the preparation for the sudden weight load that occurs in the initial stance phase.27 However, according to Toumi el al.25, activity was measured by distinguishing the VMO and the VL among the vastus muscle groups showing these similar patterns of activation. It was reported that the VMO activity was significantly increased comparing with VL activity in the movement in which could give more load to the knee joints before the landing. In view of the synthesis of these contents and the results of this study, it is thought that in the case of fast walking, the instability of knee joints can be caused not only in the initial and mid stance phase in which weight load occurs, but also in the late swing phase without weight load. But after wearing the brace, the knee joints are stabilized, and the activation of the VMO significantly decreased in both the stance phase and the swing phase. Up until now, the existing studies analyzed the size of the external moment that occurs at the time of use of the off-loading brace by using the 3-D gait analysis system with the patients of degenerative arthritis of the knee as the subject,15,16 or mainly checked the changes in pain following the load decrease of the medial side knee joints by measuring the widening of the space in the medial compartment of knee joints using fluoroscopy.12,28 However, this study analyzed the changes of the activity of the muscles around the femoral region after using the off-loading knee brace with normal people as the subject, and it is thought that in the state where the knee joint load is large and unstable, the brace significantly decreased the activation of the VMO. According to Landry et al.29, contrary to the prediction that the walking speed would be slower in patients with moderate degenerative arthritis of the knee, the actual walking speed is not significantly different from that of normal people. Therefore, when we hypothesize that the impact of the brace on muscle activation around the femoral region would be similar in healthy people and in patients with degenerative arthritis of the knee, if a patient with degenerative arthritis of the knee comes to use the off-loading knee brace in daily life and long term, the weakening of the VMO or the relative weakening of the quadriceps muscle of the thigh can be caused due to the continuous decrease of the activation of the VMO. In addition, this decrease of muscular strength of the VMO could cause the imbalance between VMO and VL and finally lead to lateral tilting of the patella and cause or further promote diseases such as the patellofemoral pain syndrome. At the time of long-term use of the off-loading knee brace, the program of selective strengthening of muscular strength of the VMO is needed. From now on, it is needed to develop a knee brace that can promote the VMO activity by using functional electrical stimulation, especially during fast walking or squatting.
There are several limitations of this study, the first being that the number of subjects who participated in the study was small, and second, only walking on a treadmill and squatting among the daily living activities were measured. Third, the results of this study were obtained from normal healthy subjects based on the supposition that the activation of femoral region muscles would be similar in normal people compared with patients suffering from degenerative arthritis of the knee, and it is hard to apply this result to the patients of degenerative arthritis of the knee directly. Fourth, the degree of activation of the femoral region muscles at the time of short-term wearing of the off-loading knee brace can be different from that of long-term wearing of the brace. Therefore, future studies should be conducted with more subjects as well as by adding daily living movements such as walking on the stairs or walking on a slope. In addition, in order to draw a generalized conclusion, subsequent studies would need to be conducted on whether the changes of the activity of the femoral region muscles of patients with degenerative arthritis of the knee after wearing the brace are different from those of normal people, and whether there is a difference in the strength and activity of the muscles of the femoral region following the period of wearing the off-loading knee brace with patients. Moreover, it is thought that the quantitative analysis of the impact of the walking speed on the activation of the muscles of the femoral region after wearing the brace should be supplemented through subsequent studies through enhancing the reliability of studies by testing not only the normal group but also additional control groups such as a population of the elderly in the changes of the femoral region muscle activity during long-term wearing of the off-loading knee brace.
Go to :
CONCLUSION
As a result of this study, the activity of the VMO significantly decreased in squatting or fast-speed exercise after wearing the off-loading knee brace in normal people compared to without the brace, and it is thought that this is a result of the external moment of the brace which effectively stabilized the patella in the movement in which the knee joints become relatively unstable. In view of these results, in patients with degenerative arthritis of the knee, the clinical effects of the use of the brace can be useful in the short term, but for long-term use, weakening of the VMO is predicted, and therefore the program of selective muscular strength strengthening for the VMO should be emphasized. In order to prevent VMO weakness, it may require a development of newly functional electrical-stimulated knee brace.
Go to :
 XML Download
XML Download