

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recently, the incidence of burns injuries is decreasing as industrial accidents are decreasing. Therefore, only a few special burn centers treat most of the burn patients and burn rehabilitation is recognized as a specialized treatment program. Initial treatment serves to prevent dehydration and secondary injury through wound disinfection and surgical treatment of skin grafting. The rehabilitation treatment after the acute phase aims to minimize the deformity of joints and to thereby preserve the functional state and to let the patient be able to return to work and home. Most joint lesions by burns occur secondarily to skin damage, and thus special skin management with exercise treatment is thoroughly needed.
The most common body parts in which burns occur are hands and arms, and one of the main complications of hand burns are finger joint contracture.1 Joint motion disorder is mostly found in the finger joints of burn patients, with the next most common being shoulder joints, elbow joints and knee joints in order. Among fingers, metacarpophalangeal joint is most commonly found affected at 29.4%.2,3 In particular, the flexion limit of metacarpophalangeal joints obstructs the motion to hold objects and thereby has a big impact on long term functional prognosis, and thus the treatment for this makes the main contribution for the enhancement of quality of life. Previous studies have investigated the use of a brace appliance, dressing fixing, joint motion range exercise, compression garment, and surgical correction in order to prevent and treat the post-hand burn contracture.4-9 Post-burn contracture causes not only scars, but also the transformation in the direction of pulling by muscles and is not easily corrected; and thus, it is important for its progress. With regard to this connection, this study examined the efficacy of modifying the Dynamic metacarpophalangeal joint flexion orthoses (Sammon Preston Roylan, Chicago, USA), which is used for correction in the cases of secondary joint contracture due to burns, and skin grafting, and but as yet, there have been no reports on its effect of treating hands.10
MATERIALS AND METHODS
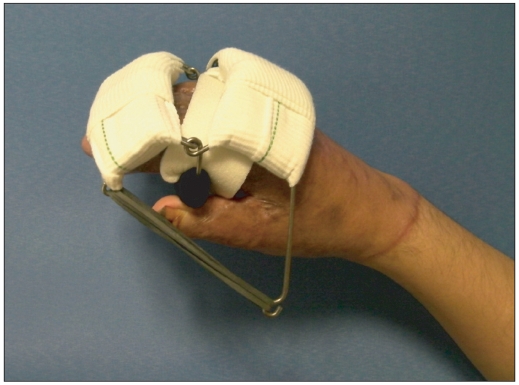
A prospective study was conducted on 42 patients, who completed acute treatment in special burn centers for hand burns and were transferred to the rehabilitation medicine department within 6 months from the injury, between March 2009 until December 2010.11,12 The study excluded patients that had fourth-degree burns with musculoskeletal diseases (fractures, amputation, rheumatoid arthritis and degenerative joint disease) in the injured hand or nervous diseases (peripheral nerve disorder, cervical radiculopathy), or injury in skin full-thickness and muscles and bone tissues The age at time of injury, gender, and the type and range of burn were examined. Patients that were within 6 months of their injury and in which the flexion motion range of metacarpophalangeal joint needed to conduct everyday living activities was limited to less than 61 degrees13 were randomly classified into and the orthotic group. Each group had 21 patients respectively. The orthoses used for this study did not obstruct the movements of proximal interphalangeal joint or the wrist and applied continuous extension in the direction of flexion of the second through fifth metacarpophalageal joints. The orthotic on the back of the hand was modified so that it would fit the average hand size of Koreans and the quality of material was adjusted to suit the state of patients'. The iron structure supporting both sides of the hand was made to be able to properly withstand pulling forces, and at the end, there is a ring, and a rubber band with improved elasticity toward the shape of a burn patient's hands and provides tension, with the dynamic correction force of joints being controlled by a change in the number of bands. The patients wore the Dynamic metacarpophalangeal joint flexion orthoses modified into this shape for 3 hours each day, one hour at a time, for a time periods of 8 weeks (Fig. 1). Both the control group and the orthotic group conducted the rest rehabilitation treatment equally, in addition to the application of orthoses.
We compared the joint motion range, the grip strength, the quality of life and the state of health, and the functions of hands before and after wearing modified Dynamic metacarpophalangeal joint flexion orthoses for 8 weeks. The joint motion range and the grip strength were measured respectively by using the goniometer and the squeeze dynamometer in order to evaluate the changes of flexion limit of metacarpophalangeal joint. In order to examine patient quality of life and the state of health,14,15 we implemented the Korean version of the Burn Specific Health Scale-Brief (BSHS-B-K). The Korean version of Michigan Hand Outcomes Questionnaire (MHQ-K),16 Jebsen Hand Function Test17 and Functional Independence Measure (FIM)18 were implemented in order to evaluate hand function level in the patients. The SPSS version 12.0 programs was used for the statistical analysis, and the significance level was set at less than 0.05. The Mann-Whitney U test was used in the statistical analysis.
RESULTS
Measurement of active motion range of joints and grip strength
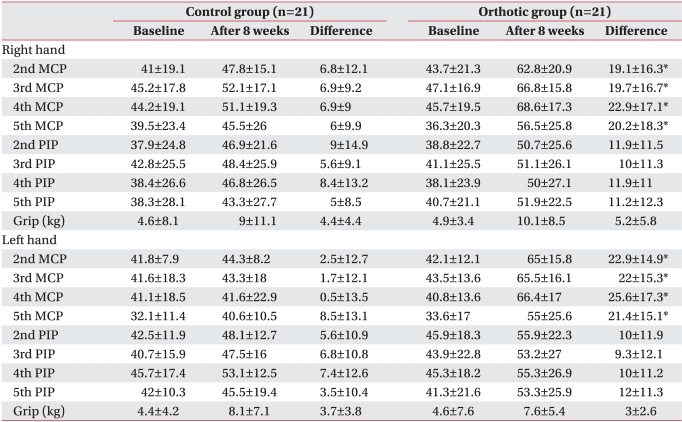
There was no significant difference in the active motion range and grip strength of the metacarpophalangeal and proximal interphalangeal joints about the flexion limit correction effect of orthoses, (p>0.05). The active joint motion range of metacarpophalangeal and proximal interphalangeal flexion of both side of the orthotic group increased after 8 weeks compared with the control group, and there was a statistically significant difference only in metacarpophalangeal joint (p<0.05), and proximal interphalangeal joint did not show a significant difference (p>0.05). In addition, there was no significant difference in the grip strength of both hands between the two groups after 8 weeks (p>0.05) (Table 1).
Evaluation of the quality of life, the state of health and the hand function
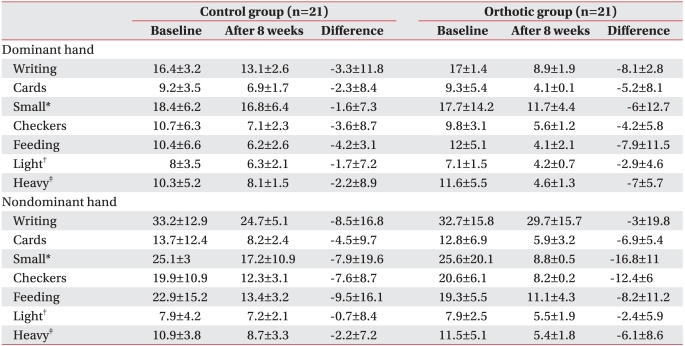
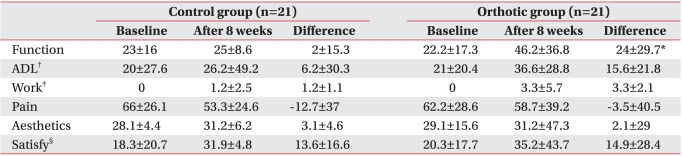
The score of the Korean version of Burn Specific Health Scale-Brief that reflects the quality of life and the state of health and the Functional Independence Measure related to the everyday living movements was not statistically significantly different between the 2 groups (p>0.05) (Table 2). The time used for conducting each test in the Jebsen Hand Function Test was the same as Table 3, and there was also no difference between the 2 groups (p>0.05). The scores on the hand function items of the Korean version of Michigan Hand Outcomes Questionnaire were 23 and 22 in the control group and the orthotic group, respectively, and increased to 25 and 46, respectively after 8 weeks; there was a significant difference between the 2 groups (p<0.05) (Table 4).
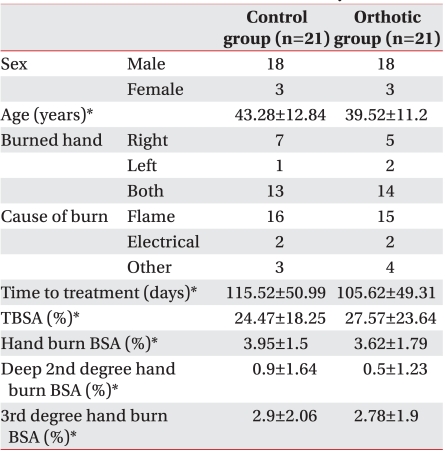
Age and gender distribution and clinical aspects
Twenty-one patients received rehabilitative medical and hospital treatment within 6 months after burn injury, in part by wearing the modified Dynamic metacarpophalangeal joint flexion orthoses; another 21 patients were classified as the control group. The average patient-subject age was 41.4±12.06 years old; and 36 patients were male and 6 patients were female. There was no significant difference between the 2 groups in gender, age, left and right distribution of hand burns, the type of burn, the time that passed since the burns until the treatment, the entire burn range and the hand burn range and depth (Table 5).
DISCUSSION
Various complications occur after hand burn, which can result in limitations in everyday movements and in functional disorders. Examples include claw hand deformity, web space contracture, dorsal contracture of the hand, thumb-in palm deformity, abduction deformity of the little finger, extensor tendon adhesion, boutonniere deformity, the pressure and cut of the median nerve and the ulna nerve, and heterotopic ossification of elbow; these cause a serious problem in the psychological and social aspects of burn patients.4
Serious disorders remain in in the hands in particular due to their functional and anatomical structure. The back of the hand has a supporting structure that stably maintains the tendon of extensor muscles at the metacarpophalangeal joint at the time of flexion and extension. This is a dorsal hood made of three supporting structures, and the extensor tendon is supported by the sagittal band at the metacarpophalangeal joint, and at a lower part, the metacarpophalangeal joint and the proximal interphalangeal joint are supported by the transverse band and the oblique band.5-8 When you see the intertendinous connections after removing the skin and thin layer of hands, you can observe that the stability of the metacarpophalangeal joint space is maintained in the second finger through the fifth finger. As the metacarpophalangeal joint is extended and the proximal interphalangeal joint gets flexion due to hand burns, these ligament structures of the hands are damaged and the surrounding supporting tissues loosen and thus contracture occurs and an unstable deformity state is caused in the metacarpophalangeal joint and finger joint due to the contracture of skin.9-11 At this time, if the metacarpophalangeal joint gets flexion, the orthotic is extended and naturally the proximal interphalangeal joint is straightened, and pressure is given to the anterior capsule of carpometacarpal joint of the metacarpophalangeal joint that obstructs extension and thus the base of the proximal interphalangeal joint faces upwards. As the functional axis of the joint moves, the physiological arm moment is decreased at the point where the flexor tendon has lost the active flexion ability, and thus the joint rotates maximally and the joint space opens without gliding. By this principle, the joint contracture is improved by properly maintaining the extensor tendon and being increased of the motion range.13,19,20
The Dynamic metacarpophalangeal joint flexion orthoses is used to assist the functions of the injured hands and to prevent or correct the joint deformities. In addition, it is used as a conservative treatment for sprain, fracture, and nerve damage. It can prevent the clawing by the extension function of extrinsic muscles by promoting the active proximal interphalangeal joint extension through passive metacarpophalangeal flexion, particularly in the patients with paralysis of the intrinsic muscles.21,22 In addition, the common standards for the ideal time of wearing orthoses of burn patients has not been established as yet, and thus the wearing schedule depended on the patient's subjective feelings of comfortable state to prevent soft tissue ischemia and pressure ulcer (alternating schedule).20,23
In the results of this study, the metacarpophalangeal joint motion range was enhanced significantly by using the modified existing orthoses, and this became a chance to provide sufficient grounds to prevent joint deformity. Subjective measures could be checked by using in the Korean version of Michigan Hand Outcomes Questionnaire. However, the orthotic group did not have a big difference from the control group in the Functional Independence Measure and the Jebsen Hand Function Test and the grip strength. It is considered that the orthoses almost did not have an effect on the thumb or the rest of the fingers' proximal and distal interphalangeal joints. Also, because of the first web space was not wide enough to produce proper muscular strength, we could not observe significant difference in the grip, hold and transfer function.24 In addition, the grip strength is also influenced by the posture of elbows and wrists,25 and thus evaluation of grip strength has limitations as a predictor of the entire hand function in post-burn joint contractures.
The study of the hand stability orthoses for the prevention of the hand contracture as a result of brain lesions is presented by Park et al26 has seen that there was no distinct effect in subacute period patients and thus the prevention of deformity through early wearing is still uncertain. However, according to Pizzi et al.,27 it was judged proper because spasticity and joint exercise range were enhanced in the stroke patients who have been 4 months or longer after the disease occurred. The effects of orthoses on the hand deformity of central disease remains controversial, particularly when this condition is accompanied by weakening of muscular strength and muscle tone and the long-term results of treatment.
The importance of orthoses for hand burn is emphasized than for central diseases because in hand burn, as skin is stabilized, the joint disorder has the personality to be fixed. The patients' tendency to clench fists after burn injury eventually worsens the tendon contracture and the deformity of finger joints. Therefore, it is important to apply proper orthoses in order to prevent deformity by maintaining the length of tendon in the hand burn patients. Hence, it is thought to be that the additional studies are needed to verify the relationship between the efficacy of orthoses and the functional evaluation scale for various hand diseases, and to develop the orthoses which can correct the thumb as well as the other fingers to improve grip function.
CONCLUSION
As a result of letting the hand burn patients wear the modified Dynamic metacarpophalangeal joint flexion orthoses, the joint motion range of the metacarpophalangeal joint was enhanced and hand functions improved. In view of these results, the modified Dynamic metacarpophalangeal joint flexion orthoses will be clinically useful for the flexion of the metacarpophalangeal joint and for improving hand function.

 XML Download
XML Download