

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Low back pain is a common disease, and it is observed at least once in 70-85% of the population during their lifetime. Low back pain is important due to progress in treating chronic pain, which decreases productivity and the financial burden globally.1-5
Several psychiatric disorders commonly accompany chronic low back pain, and the rate of depressive symptoms is 30-60% among patients.6-8 According to previous studies, a group of patients with chronic low back pain accompanied by depressive symptoms show significantly higher subjective pain, but no difference was found in the functional states or organic lesions when organic lesions, a subjective pain measure, and functioning and treatment progression were compared with a group of patients with general chronic low back pain. Improvements are minimal after rehabilitation.9 The degree of depressive symptoms at the initiation of treatment and during the treatment period are the biggest independent factor for pain intensity in patients.10 Accordingly, depressive symptoms as well as organic lesions in patients with chronic low back pain are very important for patient management. Therefore, factors associated with depressive symptoms need to be understood to consider treatment for chronic low back pain. However, socioeconomic and demographic approaches are rare in studies about depressive symptoms accompanying patients with chronic low back pain in Korea. Additionally, the subjects were limited in previous studies, so the results may have been biased in specific areas. Therefore, it is difficult to represent the general population in Korea.9,11,12
The aim of this study was to investigate depressive symptoms accompanied by chronic low back pain and their related factors using data from questions of the fourth Korea National Health and Nutrition Examination Survey (KNHANES IV) 2009, performed to sample households selected to represent the entire nation of Korea in 2009.
Go to : 
MATERIALS AND METHODS
Subjects
In the health survey of the third year (2009) of KNHANES IV, a patient with chronic low back pain was defined as "ill more than 3 months during the past year" for the items about low back pain among the 7,893 in the sample population over 19 years old. In total, 1,426 (18.1%) subjects were finally selected.
Methods
The depressive symptom group was defined as those who answered "yes" to: "Have you felt sorrow or despair that has affected your daily life more than 2 weeks continuously during the past year?" Age was limited to those over 20 years old. Four groups were investigated, and their marital status was confirmed. Education level was divided into "less than elementary school", "less than middle school", "less than high school", and "more than university". Family income was classified into quartiles. Medical security was divided into "employee health insurance subscribers", "local health insurance subscribers", and "medical-aid beneficiaries". Smoking status was classified into "smoking", "not-smoking currently", and "not applicable". Drinking frequency was classified into "less than once per month", "1-4 times per month", and "more than twice per week". Perceived health was divided into "very good, good, average, bad, very bad" and, one group included "very good, good, average" and the other included "bad, very bad". For items about activities of daily living (ADL), only "I am not disrupted from daily activity." was defined as independent. Chronic diseases included stroke, hypertension, diabetes, ischemic heart disease, liver cirrhosis, arthritis, asthma, and chronic renal failure. The cancer group included patients who had at least one cancer among stomach, liver, lung, cervical, breast, colon, and other cancers. Each disease was defined as "yes" for "Did a doctor diagnose the disease?" so errors decreased due to the subjective judgment. Body mass index (BMI) was classified into underweight (<18.5), normal weight (18.5-24.9), and obese (>25).
Data analysis
SPSS 15.0 version was used for the statistical analysis (SPSS Inc., Chicago, USA). A p-value less than 0.05 was considered significant. A cross-tabulation was used for the distributive analysis of each factor between the depressive symptom group and the general group. Distribution differences were examined with the chi-square test. Significant factors in the univariate analysis were used as variables to identify factors related to depressive symptoms in a multiple logistic regression. Model 1 was analyzed before correction of variables and Model 2 was analyzed after correction.
Go to :
RESULTS
Socioeconomic and demographic features of the study subjects
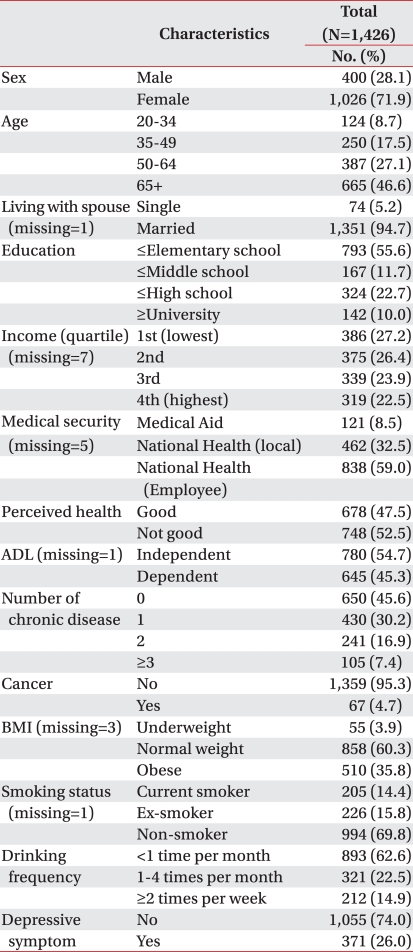
The depressive symptom group included 371 subjects (26.0%) among 1,426 patients with low back pain (Table 1). The test group was comprised of 400 males (28.1%) and 1,026 females (71.9%). In total, 124 subjects (8.7%) were 20-34 years old, 250 (17.5%) were 35-49 years, 387 (27.1%) were 50-64 years, and 665 (46.6%) were over 65 years. A total of 1,351 subjects (94.7%) were married. A total of 793 subjects (55.6%) had less than an elementary school education. For family income, 386 subjects (27.2%) were in the first quartile, 375 (26.4%) were in the second quartile, 339 (23.9%) were in the third quartile, and 319 (22.5%) were in the fourth quartile. There were 838 (59.0%) employee health-insurance subscribers 462 (32.5%) local health-insurance subscribers, and 121 (8.5%) medical-aid beneficiaries. For perceived health, 748 subjects (52.5) were "not good" and 780 subjects (54.7%) were independent with their ADL. A total of 650 subjects (45.6%) showed no accompanying disease, 430 (30.2%) showed one, 241 (16.9%) showed two, and 105 (7.4%) showed more than three diseases. The cancer group contained 67 subjects (4.7%). In total, 510 subjects (35.8%) were obese, 858 (60.3%) were normal weight, and 55 (3.9%) were underweight. For smoking status, 205 subjects (14.4%) were current smokers, 226 (15.8%) quit smoking, and 994 (69.7%) were non-smokers. For drinking frequency, 893 subjects (62.6%) drank less than once per month, 321 (22.5%) drank 1-4 times per month, and 212 (14.9%) drank more than twice per week.
Comparison of characteristics according to depressive symptoms
Depressive symptoms were significantly higher in females (p<0.001) (Table 2). Depressive symptoms were higher as education level (p=0.003) and family income (p=0.001) decreased, and higher in medical-aid beneficiaries (p<0.001) than in health insurance subscribers. Depressive symptoms were significantly higher in the "not good" group of perceived health (p<0.001) and in the ADL "dependent" group (p<0.001). Cancer (p=0.010), stroke (p=0.042), myocardial infarction or angina pectoris (p=0.009), and arthritis (p=0.007) showed significant results for relevance to accompanying chronic diseases, and more depressive symptoms were observed as the number of chronic diseases increased (p=0.018). The underweight group tended to show more depressive symptoms than the normal or overweight groups, but it was not statistically significant. Depressive symptoms were significant higher in the ex-smoker and non-smoker groups than those in the current smoker group (p=0.006). Depressive symptoms were significantly higher in the groups who drank alcohol "less than once per month" and "1 to 4 times per month" than those who drank "more than twice per week" (p=0.026).
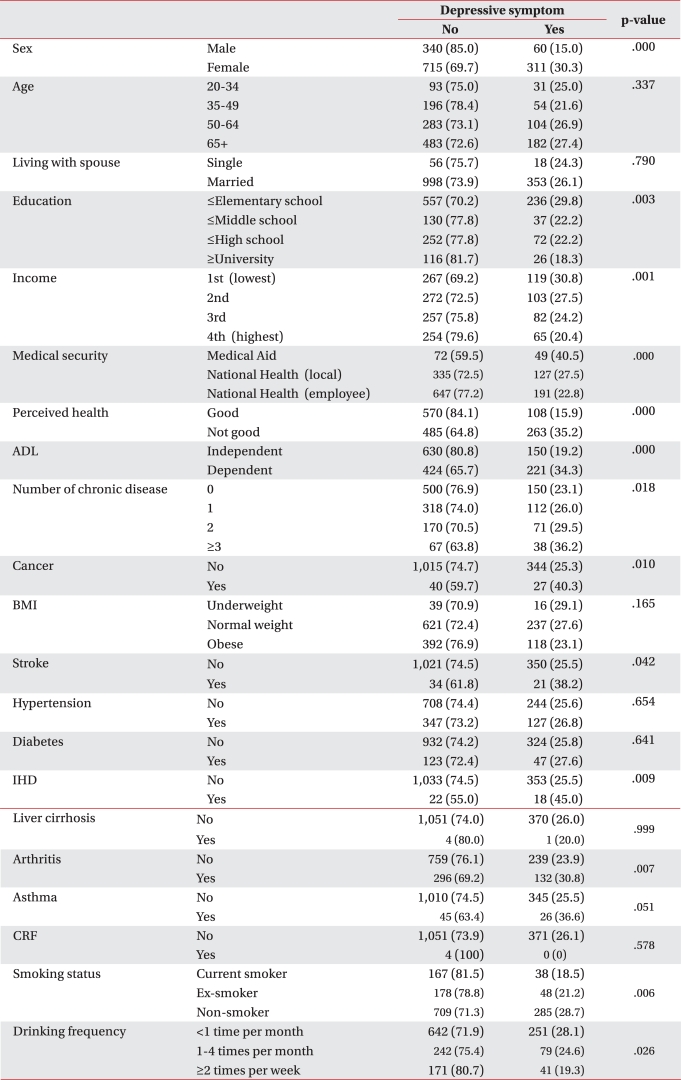
Table 2
Sociodemographic and Medical Factors Influencing Depressive Symptom in Patients with Chronic Low Back Pain
ADL: Activities of daily living, BMI: Body mass index, IHD: Ischemic heart disease, CRF: Chronic renal failure, Chronic diseases: Stroke, hypertension, diabetes, ischemic heart disease, liver cirrhosis, arthritis, asthma, and chronic renal failure, Cancer: Stomach, liver, lung, cervical, breast, colon, and other cancers
![]()
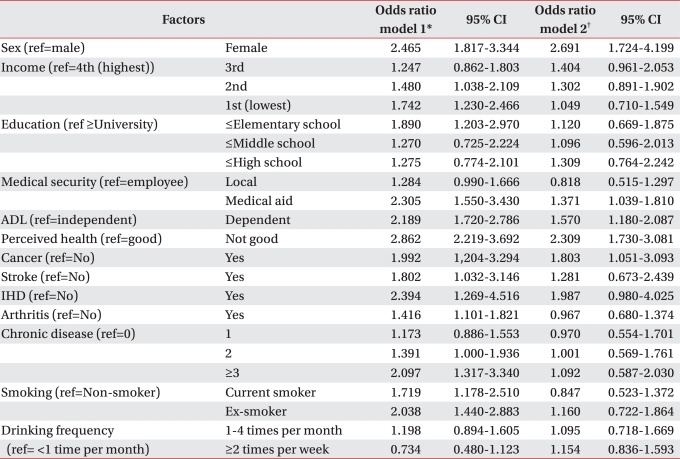
Predictable factors for depressive symptoms
In the Model 1 analysis, females showed more depressive symptoms than males (OR, 2.465; 95% CI, 1.817-3.344), and the second (OR, 1.480; 95% CI, 1.038-2.109) and first quartile (OR,1.742; 95% CI, 1.230-2.466) showed more depressive symptoms than the fourth quartile of family income. More depressive symptoms were shown for subjects with "less than an elementary school" education (OR, 1.890; 95% CI, 1.203-2.970) than those with "more than university", and medical aid beneficiaries (OR, 2.305; 95% CI, 1.550-3.430) showed more depressive symptoms than those of employee health insurance subscribers (Table 3). The dependent group in ADL (OR, 2.189; 95% CI, 1.720-2.786) showed more depressive symptoms than those of the independent group. "Not good" in perceived health (OR, 2.862; 95% CI, 2.219-3.692) resulted in more depressive symptoms than those of the "good" group. Depressive symptoms were significantly higher for patients with cancer (OR, 1.992; 95% CI, 1.204-3.294), stroke (OR, 1.802; 95% CI, 1.032-3.146), myocardial infarction or angina pectoris (OR, 2.394;, 95% CI, 1.269-4.516), and arthritis (OR, 1.416; 95% CI, 1.101-1.821). The group with more than three accompanying chronic diseases (OR, 2.097; 95% CI, 1.317-3.340), and past (OR, 2.038; 95% CI, 1.440-2.883) and present (OR, 1.719; 95% CI, 1.178-2.510) smokers had more depressive symptoms than the non-smoker group. However females (OR, 2.691; 95% CI, 1.724-4.199), medical-aid beneficiaries (OR,1.371; 95% CI, 1.039-1.810), the ADL dependent group (OR, 1.570; 95% CI, 1.180-2.087), 'not good:' for perceived health (OR, 2.309; 95% CI, 1.730-3.081) and the cancer group (OR, 1.803; 95% CI, 1.051-3.093) were the only statistically significant variables in the multivariate regression after the correction.
Go to :
DISCUSSION
Socioeconomic and demographic factors related to depressive symptoms in patients with chronic low back pain were studied based on the KNHANES IV (2009). Gender, medical security, ADL, perceived health and accompanied cancers were related to depressive symptoms after correcting for other variables.
Generally, the interrelationship between gender and depressive symptoms are well known. The prevalence rate in suspected patients with depression who scored more than 16 points on the Center for Epidemiological Studies-Depression Scale in Korea was 23.1% in males and 27.4% in females. In severe cases of depression (>25 points), the prevalence rate was 6.8% in males and 10.4% in females.13 According to the type of medical security, depressive symptoms were significantly higher in medical-aid beneficiaries than those in employee health insurance subscribers. In medical-aid beneficiaries, low level of education, single patients who lived alone, and low monthly average family income were considered in previous studies and selection standards were referred, so there might be indirect effects.14 Depressive symptoms increased in the low-ability ADL group compared to those in the high-ability group, which was similar to a previous study.15 Depressive symptoms increased as perceived health became poorer, and the reason is associated with studies about health-related quality of life and depressive symptoms.16 The correlation between accompanied cancers and depressive symptoms has been revealed in many studies. In particular, patients with pancreatic cancer, oropharyngeal cancer, and breast cancer show more depressive symptoms and the prevalence rates are 20-25%.17-20
Many studies have reported the relationship between depressive symptoms and chronic diseases. In this study, stroke, myocardial infarction or angina pectoris, and arthritis were significantly different in the univariate analysis. In previous studies of stroke, depressive symptoms were different by location of the lesion, and more depressive symptoms were observed when the lesion was located on the left side.21,22 In previous studies about myocardial infarction or angina pectoris, many patients showed depressive symptoms and high morbidity rates, and the male result was similar to that of females, so our results agreed with those of previous studies.23,24 In addition, depression and severity of depression symptoms influences a decrease in arthritis symptoms.25,26 In the univariate analysis, depressive symptoms increased as the number of chronic diseases increased. Thus, by contracting more chronic diseases, related physical symptoms would increase and functional disorders would occur, which would increase medical expenses. Therefore, increasing depressive symptoms were expected.27
In the univariate analysis results about smoking and depressive symptoms, the past and present smoker groups showed fewer depressive symptoms than those in the non-smoker group. According to previous studies, depressive symptoms increase remarkably when a smoker group was forbidden to smoke. However, smoking has generally been reported to increase depressive symptoms, so it is difficult to say that smoking has a positive effect on depressive symptoms.28-31 The group who drank alcohol "less than once per month" showed more depressive symptoms than those who drank "more than twice per week" and this result was also different from previous studies.32,33 This difference might have been caused by the plurality of females who showed less smoking and drinking rates among participants in this study.
The first limitation of this study is that it was cross-sectional, so it was difficult to interpret chronic low back pain and depressive symptoms as a simple cause and effect relationship. In general, chronic low back pain occurred first and then depressive symptoms followed but several factors related to depressive symptoms could also cause depressive symptoms, so previous studies have indicated careful interpretation of these types of data.34 Questions about the intensity of low back pain were not used for patients with chronic low back pain, so depressive symptoms and the differences with ADL were not compared. In addition, a single question was provided to measure the degree of depression instead of established selection tools, so accuracy could be limited. However, the one question of "Do you often feel sad or depressed?" showed a sensitivity of 86%, a specificity of 78%, and positive predictive and negative predictive values of 82% in previous studies, so the error was thought to be small.35 A self-writing method was used for the health survey, so accuracy could be limited. However, the survey was performed at a mobile clinic center with an investigator, so it was different with other methods without an observer.
Despite these limitations, this study included every family in Korea so the results are representative, because it was not limited to specific hospitals or local areas. Relatively more patients with chronic low back pain were investigated compared to previous studies. Additionally, psychosocial risk factors as well as organic disturbances could be evaluated through socioeconomic and demographic approaches regarding factors related to patients with chronic low back pain and depressive symptoms. Therefore, this study suggests various ways to approach patients with low back pain.
Go to :
CONCLUSION
Low back pain is observed at least once in most people's lives and has a significant effect on society as well as each patient because it is chronic. In particular, psychological factors as well as organic disturbances act in a complex manner for a prognosis. Therefore, a diagnosis of depressive symptoms in patients with chronic low back pain and an analysis of related factors are essential for comprehensive rehabilitation.
Socioeconomic and demographic factors related to depressive symptoms were studied by KNHANES in patients who reported chronic low back pain more than 3 months during the past year. This result suggests preliminary data to grasp factors influencing depressive symptoms. Thus, more effects are expected when managing chronic low back pain by combining organic disturbance, which causes pain, and the emotional aspects during treatment.
Go to :
 XML Download
XML Download