

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In recent years the life expectancy of patients with a spinal cord injury (SCI) has tended to increase as mortality due to complications of their injuries has decreased.1-3 Cures for disease not only increase life expectancy, but also increase interest in quality of life. The complications of injuries restrict engagement in various activities so that patients have difficulties in adapting to society.4 However, it is possible to boost social adaptation and improve life satisfaction by participation in leisure activities as well as by training and suitable employment.5
Leisure activities are an import source of pleasure to patients if they can choose what to do according to their circumstances and preferences. Leisure time means free time and excludes time spent on essential activities such as paid employment, chores, eating, sleeping, and going to school.6 Leisure activities not only put high emphasis on restful pursuits such as reading, watching TV, stamp collecting or watching performances, but also on more physical activities such as sports like football, mountain climbing, traveling, fishing or jogging. Leisure time physical activity (LTPA) is physical activity which people choose to do during their free time, and in case of patients with SCI it includes walking or wheeling and certain sports played in a gym.7
In the able-bodied population, considerable epidemiologic evidence indicates that greater LTPA is associated with lower risks of morbidity and all-cause mortality.8,9 Likewise, in people with SCI, accumulating data suggest that LTPA is associated with better fitness and health.10-13 However, very little is known about LTPA participation in the SCI population.12,14,15 Research into the total daily physical activities of chronic SCI patients indicates that the level of activity in most patients is low.14,16 However, these reports did not distinguish between general physical activity and LTPA. Neverthless, LTPA is now considered important for the health of chronic SCI patients.17-19 The purpose of this study is to assess the relationships between the type, extent and intensity of leisure activities and the general and injury-related characteristics and satisfaction levels of SCI patients.
MATERIALS AND METHODS
Subjects
The study involved a questionnaire survey of 79 chronic SCI patients attending spinal cord injury clubs in the Busan Kyeongnam area of Korea. All participants had provided formal consent, and the survey was conducted during June to December, 2010.
Method
1) Demographic and injury-related characteristics. The questionnaire (see Appendix 1 for complete questionnaire) contained items about age, gender, highest level of education completed, marital status, injury severity, date of injury, employment status before/after injury, income sources and medical payment status, and leisure activities before/after injury.
2) Leisure activities after SCI. For the investigation of current leisure activities, participants recalled all activities requiring physical exertion that were recently performed. To facilitate their recall of physical activities, participants were asked to report their recent average hours awake during the day. They were also asked to estimate their recent average daily hours of leisure time and how many hours of their leisure time involved some physical activity. Information about the type of physical and non-physical leisure activity in which they had recently engaged was obtained using checklists. The list of physical leisure activities contained sports activities (e.g. wheeling, lawn ball, curling), stretching exercise, resistance exercise, standing exercise, aerobic exercise, craftsmanship, and other similar activities. The list of non-physical leisure activities contained enjoying movies, reading, using computers and internet, concert watching, shopping, driving, listening to music, and other similar activities. The participants were also to rate the intensity of engagement in the physical activities and their levels of satisfaction with both the physical and non-physical activities. All ratings were made on scales from 0 to 10, with higher scores indicating greater intensity or satisfaction. The participants were asked to provide reasons for their satisfaction or dissatisfaction and, for dissatisfaction with physical leisure activities, they were given a checklist of likely reasons (pain, spasticity, poor bladder and bowel management, decreased vital capacity and other reasons). Checklists were also used for participants to indicate reasons for limitations on their engagement in physical and non-physical leisure activities (lack of money, accessibility, lack of time, absence of caregiver, poor health and other reasons). Finally, they were asked about their sources of information regarding leisure activities, and again a checklist was supplied (friends & co-workers, doctor, internet, family, SCI patients' gathering and other sources).
3) Statistical analysis. All analyses were performed using SPSS version 12.0 for Windows. Pearson's correlation coefficient was used for the relationships between age, years post-injury and LTPA time. The relationships between gender, marital status and employment status after SCI were analyzed using Student's t-tests. One-way ANOVAs were performed to investigate differences in levels of education completed, degree of injury, income sources and medical payment status. A p-value less than 0.05 was considered statistically significant.
RESULTS
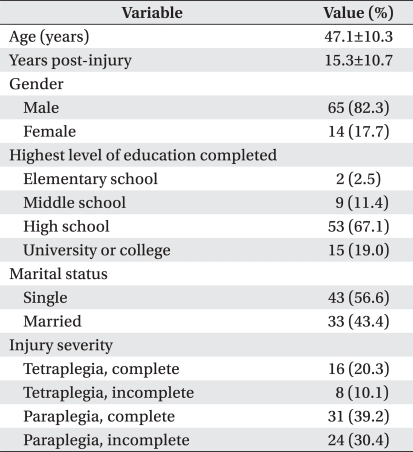
The mean age of the participants was 47.1 years, and the mean time since spinal cord injury was 15.3 years. There were more men (n=65, 82.3%) than women (n=14, 17.7%). Most (n=64, 81.0%) had reached high school level of education, and slightly more were single (n=43, 56.6%) rather than married. In terms of the degree of injury, most (n=54, 69.6%) had some degree of paraplegia rather than tetraplegia (n=24, 30.4%). Amongst the paraplegia patients, complete injury (n=31, 39.2%) was slightly more common than incomplete paraplegia (n=24, 30.4%). This was in contrast to the tetraplegia patients, in whom complete injury was twice as common as the incomplete degree of severity (n=16 vs n=8) (Table 1).
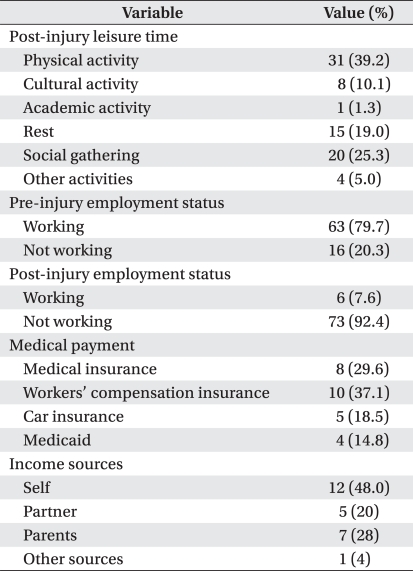
Many of the survey respondents had been unable to remain in the workforce. Whereas 63 people (79.7%) reported having a job prior to their injury, only six (7.6%) were currently employed. However, while few (n=25) provided information about their present source of income, almost half of these (n=12) saw themselves as being their source of income. For their current payment of medical expenses, workers' compensation insurance was the most frequent (37.1%) form of cover. Looking at the different types of leisure activities, in which the participants had recently participated, the number involved in physical activities was found to be 31 (39.2%), in cultural and academic 9 (11.4%) and in the use of free time for resting it was 15 (19.0%) (Table 2).
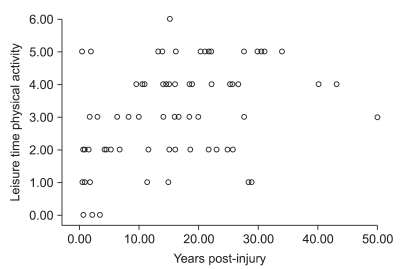
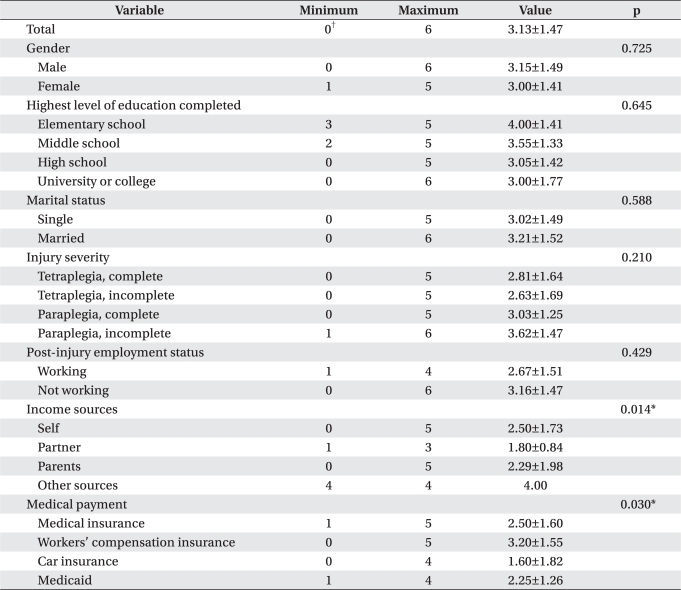
The mean time of being awake during the day was 16.27±2.92 hours, and the mean daily time invested in leisure activities was 6.05±3.38 hours. The mean daily time invested in LTPA was 3.13±1.47 hours. The mean daily time spent in wheeling, when this was the only physical leisure activity selected, was found to be 2.86±1.21 hours. Three people (3.8%) reported engaging in no physical activity during their leisure time. There were no significant differences in LPTA time according to gender, educational history, marital status, degree of injury, or present employment. However, the amount of LPTA time was positively correlated with the length of time since the injury (Fig. 1), and the relationships with income source and type of cover for medical expenses were statistically significant (p<0.014 and p<0.030, respectively) with the highest LPTA hours being associated with self as income source and the workers compensation scheme (Table 3).
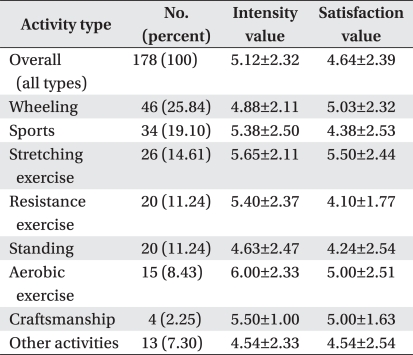
Wheeling, sports activities and stretching exercises were the commonest forms of LPTA. In general, the physical activities were performed at moderate levels of intensity (overall mean=5.12±2.32); aerobic exercises were associated with the highest levels of intensity, but otherwise there was little difference between the different types of LPTA. The mean intensity level for wheeling was 4.14±2.79, but the intensity level was higher when wheeling was the only kind of physical exercise (mean=5.27±2.40).
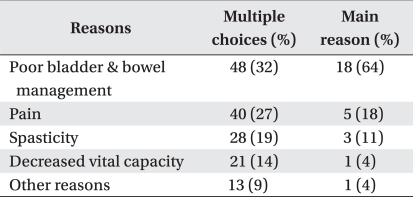
The mean overall level of satisfaction with the exercises was 4.64±2.39 points. Again, there was little difference between the exercises, but the highest satisfaction was when doing stretching exercises (Table 4). The mean satisfaction with wheeling when it was the only form of exercise was 4.71±2.98. When wheeling was excluded, the overall mean satisfaction with the other exercises was found to be 5.06±2.46. When participants were allowed to choose more than one reason, poor bladder and bowel management was the commonest reason given for dissatisfaction (n=48, 32%). The next most common reasons were pain (n=40, 27%) and spasticity (n=28, 19%). When participants were asked to select a single main reason for dissatisfaction, the rank order of frequency of reasons selected remained unchanged with the majority choosing problems related to bladder and bowel management (n=18, 64%) (Table 5).
Using a computer and the internet was the commonest type of non-physical leisure activity (n=40, 24%). The frequencies of engaging in the other forms of non-physical leisure activities were: enjoying movies, 26 people (15%); listening to music, 25 people (15%); driving, 18 people (11%); reading, 16 (10%); shopping, 14 (8%); and concert watching, 12 people (7%). The number who mentioned 'other' activities was 17 (10%). Mean satisfaction with non-physical activities was 4.71±2.50, which was similar to the mean level found for physical activities.
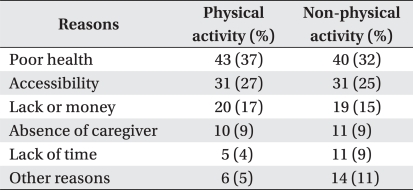
For both physical and non-physical activities, poor health and accessibility were commonest reasons given for having insufficient leisure activities (Table 6).
Information about leisure activities was mostly obtained from the SCI patients' gatherings with 34% reporting this source, and 25% received the information from friends or co-workers, but only 11% said that it came from doctors. Other sources of information were the internet (11%) and family members (6%). Additional sources were mentioned by 13%.
DISCUSSION
The purpose of this study was to investigate relationship between the general and injury characteristics of chronic SCI patients and their physical leisure time, and to examine the nature of their actual physical activities and in what other ways they spend their free time. Although no big differences were found from the findings of previous studies in terms of age, gender distribution, marital status, degree of injury,20 and years post-injury, the educational level of the present sample of SCI patients was higher than that found in overseas studies with 81.0% completing high school compared only 34.7% in those other studies.20,21 However, while in other countries the proportion in employment after injury has ranged 43-48%, in this study only 7.6% had paid work, and this is a big difference.22,23 On the other hand, in the present study 37.1% reported having workers' compensation insurance. This is a far greater figure when compared with the data of Rosenberg and others,24 which showed only 13.1% were earning benefits from workers' compensation insurance. The relevant point here is that a high number of jobless patients may be related to a high number of cases of gaining benefits from workers' compensation insurance.
Physical activities accounted for 39.2% of the activities done during leisure time after injury, which was similar to 36%, previously found in other studies.25 Since 19.0% used their leisure for having a rest, it is thought there are many, who spend time relaxing due to the complications after injury.
Most of the participants engaged in physical activities during their leisure time, and only 3.8% were found to have no physical activity at all. This result is very different from the equivalent finding of 50% reported by Martin Ginis et al.20 Furthermore, the mean daily time spent on LTPA was 3.13±1.47 hours which is considerably higher than the comparable figure of 27.14±49.35 minutes found by Martin Ginis et al.20 Similarly, an average of 49±31 minutes was reported by Buchholz et al.14 and 40.4±50.11 minutes by van den Berg-Emons et al.16 Since the present study was conducted on relatively active patients, who were regularly participating in gatherings at social clubs for patients with SCI, the subjects are thought to have been more generally active. Additionally, many of the respondents in this survey reported wheeling as a physical leisure activity. It is hard to differentiate between the use of a wheelchair as a leisure activity and its use for general mobility purposes. If SCI patients saw the general use of a wheelchair as a leisure activity, then this may explain the low number of SCI patients who reported no physical leisure activity in the present study. Where wheeling was the only physical activity, the mean daily hours of physical activity were 2.86±1.21, which is quite a long time. However, where the patients also spent time on other exercises, the overall mean daily hours were 3.13±1.47 hours. This suggests the high possibility that the investment of leisure time in activities other than wheeling may have relatively small.
Other studies have reported that hours of participation in LTPA are correlated with patient characteristics such gender, age, years post-injury, and the degree of injury.12,16,20 For example, it was found out that men are more active than women, and that younger patients are even more physically active. The suggestion has been women are less active because they have less knowledge of physical activities and more fear of outside activities than men.26,27 Similarly, in case of older patients, physical aging and health problems were said to be impediments to the adoption and maintenance of physical exercise activities.28 In the present study, although the difference was not statistically significant, men appeared to spend more hours engaged in physical activities than women (3.15±1.49 hours vs 3.00±1.41 hours). One of the statistically significant relationships between characteristics related to injury and hours of LTPA was that physical activity appeared to increase as the years post-injury increased. This finding was completely opposite to that reported by Martin Ginis et al.,20 which showed that the activities decreased over time after injury. The explanation for these contradictory findings may be that, in other countries, patients become employed after a certain time post-injury and have increased activities related to their work, whereas the participants in this current survey had experienced long periods of unemployment and thus had more hours to invest in leisure activities.
In other studies, a relationship was found between severity of injury and leisure time physical activity with patients, who had incomplete spinal injuries, engaging in more hours of activity than those with complete injuries,14,16,20 but this relationship was not statistically significant in the current survey.
In this research, cases where patients themselves were the main source of income reported daily leisure physical activity hours (mean=2.50±1.73) which were higher than in the cases where patients relied on their spouses or parents. With respect to the types of cover for the payment of medical expenses, cases receiving compensation from workers' compensation insurance showed a higher degree of daily physical leisure activity (mean=3.20±1.55 hours).
The top three most practised LTPAs in this research were wheeling, sports such as lawn ball, and stretching exercises. These physical activities were also reported as commonly practised by patients with SCI in previous studies; for example, Martin Ginis et al.29 found that aerobic exercise, weight training, and wheeling were the exercises most likely to be performed, and in the research by Carpenter et al.25 commonly practised physical activities were deep breathing and muscle relaxation (49%), patients engaged in weight training (45%), swimming (28%), wheeling (19%), and sports activities (18%). The reason why all these studies showed similar results is probably because these particular exercises are easier for patients with SCI to access than other exercises.29 However, the reason wheeling was found to be the most frequently practised exercise in the present survey, unlike the findings of the other researches, is the possibility that patients included as a leisure activity their general use of a wheelchair for daily living purposes.
Most of the leisure time physical activities were implemented at a moderate level of intensity, and by setting the most intensive level of activity as 10 points, the overall physical activities were engaged at an intensity which averaged 5.12±2.32 points. The average intensity of physical activity found in this research was similar to findings of Martin Ginis et al.,29 who reported that in their study most of the physical activities were implemented at mild or moderate level of intensity. Studies have shown that implementing physical activities at a moderate degree of intensity helps increase physical ability in patients with SCI,30 and the results of the present research can be a good guide when offering physical exercises to SCI patients in the future.
Satisfaction with exercises was found to be around the medium level of the overall range with a mean of 4.64±2.39 on the 10-point scale. When the patients were allowed to select more than one cause of dissatisfaction, the most frequently selected causes were poor bladder and bowel management (32%) and pain (27%). When they were asked to choose only one (ie the main) cause of dissatisfaction, the majority (64%) selected poor bladder and bowel management, and only 18% chose pain. This indicates that clearly the biggest source of dissatisfaction with physical leisure activity is poor bladder and bowel management. Carpenter et al.25 reported a similar result with 52% and 17% of their patients reporting that their degree of injury and pain (respectively) were factors, which limited their participation in physical and fitness activities.
Non-physical leisure activities included (in descending order of frequency) using a computer or the internet (24%), watching a movie or listening to music (15%), shopping (8%), and concert watching (7%). In general, these activities were easily done for the purpose of having a rest. In contrast, the research by Carpenter et al.25 revealed a great deal of active social participation, such as visiting or going out with family members or friends (71%), participating in social gatherings (37%), physical activities (36%), and volunteering (16%). There were relatively low frequencies of the use of computers and the internet (4%), reading (4%), and listening to music or performing (3%). These differences in the outcomes of the two studies may have been due to the Korean patients living in domestic situations which were not conducive to the enjoyment of outdoor activities and being considered as a burden on others. In the Carpenter et al.25 study, the SCI patients reported a mean happiness index score of 5.0±1.4 on a scale with scores ranging from 1 to 7, and a mean life satisfaction score of 18.6±7.6 on a scale with scores ranging from 5 to 35. High scores indicated high levels of happiness and satisfaction. Most of their patients therefore indicated that they were living happy and satisfying lives, even after injury. They also reported that their feelings of satisfaction and happiness became stronger as the hours of associating with family members or friends increased. This suggests that the reason why, in the present study, the mean satisfaction with non-physical leisure activities was only 4.71±2.50 on the 10-point scale was because there were many individual activities rather than activities of social participation. Another reason may be that the non-physical leisure activity options provided in the present questionnaire were primarily forced options and largely individual rather than social.
Although quality of life can be enhanced and physical or mental satisfaction can be found through leisure, there can be cases where participation is difficult due to impeding factors, even when participation is wanted. In the present study, the biggest impediment to leisure activity was found to be poor health, which could have arisen due to the secondary complications of SCI or some more general deterioration in health. Other factors, less frequently reported, included problems of access to leisure facilities and unaffordability. Carpenter et al.25 reported similar findings with their respondents mentioning the following impeding factors: poor health, including bladder and bowel difficulties (23%), physical limitations, including paralysis and poor balance (22%), accessibility and transport problems (21%), and lack of money or funding (10%). While health promotion provided in medical consultations and treatment by medical teams are important for encouraging patients to participate in leisure activities, attention to the social and occupational welfare issues confronting SCI patients is also needed.
This research study has several limitations. Firstly, the findings apply only to SCI patients in the Busan Kyeongnam area and cannot be generalized to all the country. Secondly, the subjects for this research were recruited from the chronic SCI patients attending spinal cord injury clubs. This group of patients is likely to represent the more socially active patients and those with a higher level of participation in leisure activities. This limits the degree to which the results can be generalized to all SCI patients. Finally, as mentioned earlier, the extent of wheeling as one of the physical leisure activities may have been inflated by inclusion of the times when the use of wheelchairs was really just a part of general daily activity. The possible consequence of this is that, although the overall levels of physical leisure activity seem higher than in other studies, they may actually be comparable.
CONCLUSION
As a result of examining the factors influencing actual conditions of leisure life or leisure life itself of chronic SCI patients in Busan and the Kyeongnam province, the overall number of hours invested in leisure and physical leisure activities were found to higher than those reported in studies conducted in other countries. The possibility that the activity rate was found to be relatively higher due to the use of wheelchairs for general living purposes cannot be excluded. The intensities with which physical activities were used implemented were at an appropriate level, and the satisfaction ratings were in the middle range. Compared with studies elsewhere, the unemployment rate was high as was the proportion receiving payments from workers' compensation insurance. The hours of productive activity through employment seemed too low. From the perspective of the findings of this study, we should be encouraging the expansion of general social facilities to improve satisfaction levels and increase physical activity hours during leisure life, and we should be improving the economic circumstances of SCI patients by promoting the return to employment through vocational training.

 XML Download
XML Download