

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
For patients with locally advanced rectal cancer, neoadjuvant chemoradiotherapy (nCRT) followed by radical surgery is the standard treatment. Although nCRT has been shown to increase the control of local disease while reducing toxicity associated with treatment, it has not been shown to improve overall survival (OS) [12]. As distant recurrence occurs in roughly 30% of patients [2345], adjuvant chemotherapy has been used to stop or destroy circulating tumor cells and micro-metastases in order to decrease distant recurrence. Although adjuvant chemotherapy is recommended for patients who undergo nCRT and radical surgery, the use of adjuvant chemotherapy for patients with rectal cancer following nCRT and radical surgery has not demonstrated a clear benefit, especially for patients that respond well to nCRT, such as ypT0–2N0 [456]. Some studies have suggested that adjuvant chemotherapy should be used selectively, as patients treated with nCRT and radical surgery that achieve stage ypT0–2N0 already have a favorable oncologic outcome, so they may not benefit from adjuvant chemotherapy following nCRT and surgery [789].
Although there is one previous meta-analysis about adjuvant chemotherapy following nCRT and radical surgery for rectal cancer [10], it did not focus on patients with ypT0–2N0 rectal cancer. Since there were no random trials with a subgroup of ypT0–2 patients excluding N positive, no previous random trial on this subject can be a part of a meta-analysis that focuses solely on ypT0–2N0 patients. Consequently, the hypothesis that adjuvant chemotherapy is beneficial for ypT0–2N0 rectal cancer patients needs stronger evidence for confirmation. Therefore, we performed a meta-analysis to assess the oncologic efficacy of adjuvant chemotherapy for patients with ypT0–2N0 rectal cancer who were treated with nCRT and radical surgery.
METHODS
This meta-analysis followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [11]. Multiple comprehensive databases were searched for studies that assessed the oncologic effects of adjuvant chemotherapy compared with observation for patients with ypT0–2N0 rectal cancer after nCRT and radical resection surgery. The study protocol used Cochrane Review Methods [12]. This study was approved exempt from Institutional Review Board of Jeonbuk National University Hospital (No. CUH202001021-HE001).
Data and literature sources
Studies were identified from PubMed (January 1, 1976 to December 13, 2018), Embase (January 1, 1985 to December 13, 2018), and the Cochrane Central Register of Controlled Trials (CENTRAL; January 1, 1987 to December 13, 2018). There were no restrictions regarding the year of publication, and articles in any language were permitted for review. The search terms were “rectal cancer,” “neoadjuvant chemoradiotherapy,” “adjuvant chemotherapy,” “recurrence,” “prognosis,” and “survival.” After the preliminary electronic search, further articles were searched for manually to retrieve additional studies. Finally, all articles were assessed individually for inclusion.
Study selection and data extraction
Article titles and abstracts were screened and full texts were independently reviewed by 2 reviewers according to the selection criteria. Any differences in judgment regarding inclusion were resolved through discussion between the reviewers.
The included studies assessed survival outcomes, including OS, disease-free survival (DFS), cancer-specific survival (CSS), local recurrence, and distant recurrence, for patients with ypT0–2N0 rectal cancer after nCRT and radical surgery. Studies were excluded if they: (1) assessed patients with stage IV or recurrent rectal cancer; (2) assessed patients who received neoadjuvant radiotherapy alone without chemotherapy; (3) examined rectal cancer patients who did not receive total mesorectal excision after completion of nCRT; (4) examined rectal cancer patients who had observation after completion of nCRT; (5) had no extractable data and authors were unavailable to provide additional information (e.g., only an abstract was available); or (6) were case series with fewer than 10 patients.
All eligible studies were reviewed and all relevant data were extracted by the 2 reviewers independently using a data extraction form designed before the review. The variables recorded were: (1) standard publication information, including year of publication, name of the first author, and number of patients; (2) clinical and demographic characteristics of all patients; and (3) outcomes (5-year OS, DFS, CSS, local recurrence, and distant recurrence).
Assessment of methodological quality
The methodological quality of the studies included in the meta-analysis was assessed using the Newcastle-Ottawa quality assessment scale (NOS), which attributes a maximum of 9 points to each study and categorizes a study with a score of 6 or more as “high quality” [13]. The quality of the included studies was analyzed using 3 metrics: study group comparability, patient selection, and outcome assessment.
Statistical analysis
Odds ratio (OR), variance, and 95% confidence interval (CI) were determined in the meta-analysis. Heterogeneity, including its presence and extent, were assessed using the Q test and I2 index, respectively; a P-value less than 0.1 was considered statistically significant [14]. The DerSimonian-Laird random effects model was used to pool data in light of cross-study heterogeneity [15]. When sufficient data were available, subgroup analyses were performed. For this analysis, patients treated with nCRT and radical surgery were separately categorized as patients with ypT0N0 rectal cancer and patients with ypT1–2N0 rectal cancer. Sensitivity analyses were also performed to assess the robustness of the meta-analysis findings [1617]. Sensitivity analysis of the data was determined with the trim-and-fill method and an alternative effects size, and were performed to exclude any studies with large outlying effects. Assessment of publication bias was done using the Egger weighted linear regression test, along with visual inspection of funnel plots showing outcomes [1819]. Data analyses were performed using Review Manager software (ver. 5.3; Cochrane Collaboration) and Comprehensive Meta-Analysis software (ver. 3; Biostat, Englewood, NJ, USA).
RESULTS
Description of studies
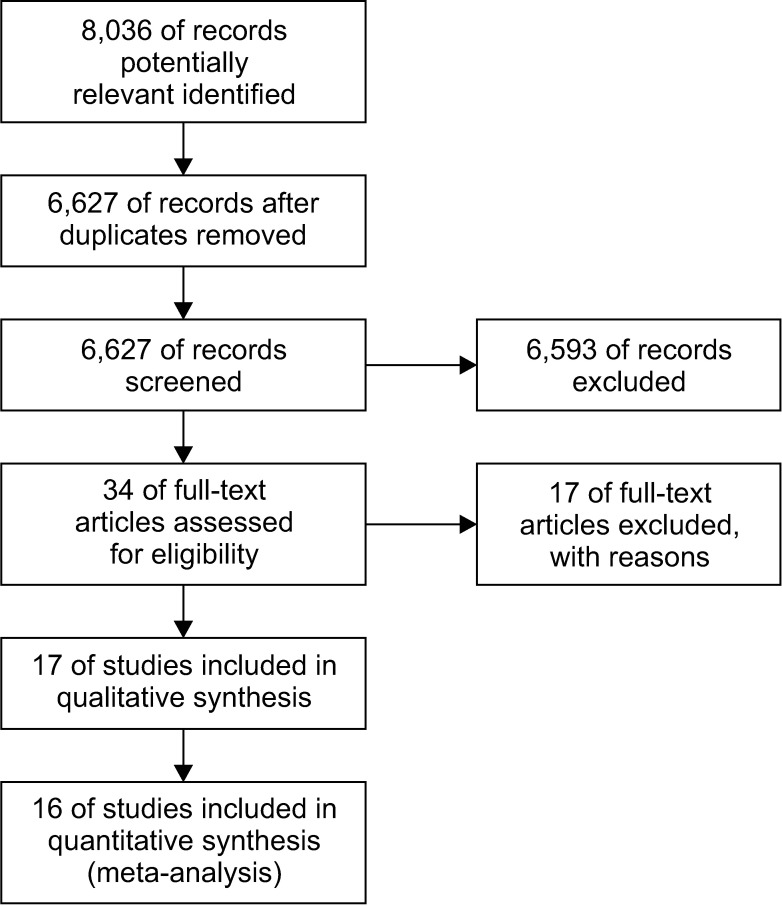
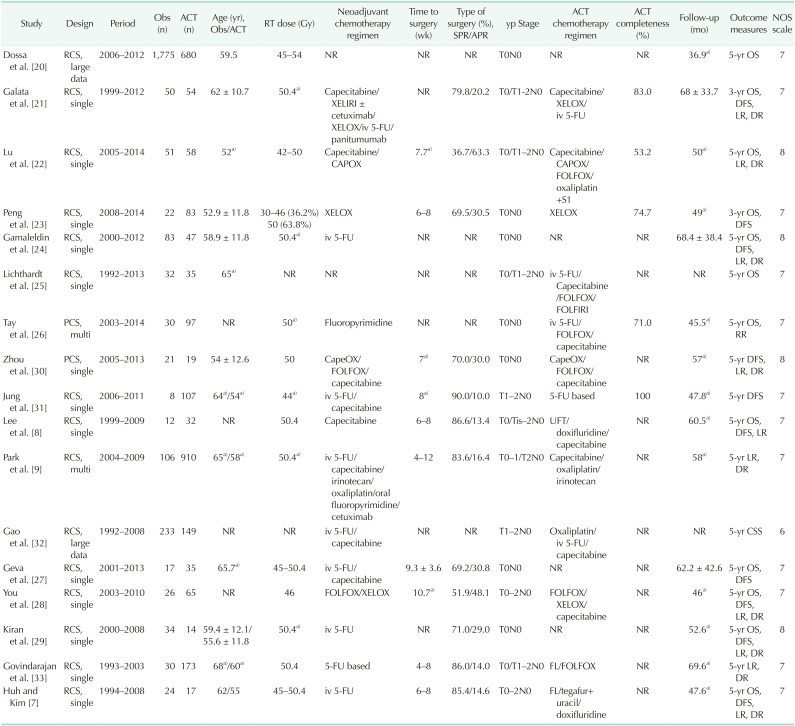
The predefined search strategy and manual searching identified 8,036 potentially relevant articles. We excluded 1,409 articles because they were duplicates, and 6,593 articles because their titles and abstracts did not fulfill the selection criteria. After full text review of the remaining 34 articles, we excluded 17 articles because of the exclusion criteria of this study. Therefore, we included 17 nonrandomized studies for qualitative analysis and 16 nonrandomized studies that examined 4,747 patients for the meta-analysis (Fig. 1). Twelve studies evaluated OS [7820212223242526272829], 10 studies evaluated DFS [782123242728293031], one study evaluated CSS [32], 10 studies evaluated local recurrence [78921222428293033], and 8 studies evaluated distant recurrence [79212224283033]. Eight studies examined patients with ypT0–2N0 rectal cancer [79212225282933]; among these, 5 studies separately analyzed patients with ypT0N0 and ypT1–2N0 rectal cancer [821222533]. Seven studies examined patients with ypT0N0 rectal cancer alone [20232426272930], and 2 studies examined patients with ypT1–2N0 rectal cancer alone [3132]. Evaluation of methodological quality showed all studies scored high (≥6) on the NOS. Table 1 summarizes the characteristics of included studies.
Oncologic outcomes of adjuvant chemotherapy in patients with ypT0–2N0
Analysis of oncologic effects of adjuvant chemotherapy in patients with ypT0–2N0 indicated that 12 studies (3,454 patients) reported data on OS; patients who received adjuvant chemotherapy had better survival than patients who were not (OR, 1.71; 95% CI, 1.03–2.85; I2 = 32%) (Fig. 2A). Ten studies (851 patients) reported data on DFS; there were no significant survival differences between the observation and adjuvant chemotherapy groups (OR, 1.52; 95% CI, 0.90–2.55; I2 = 11%) (Fig. 2B). Ten studies (1,907 patients) reported data on local recurrence; there were no significant survival differences between the observation and adjuvant chemotherapy groups (OR, 1.88; 95% CI, 0.97–3.62; I2 = 0%) (Fig. 2C). Eight studies (1,734 patients) reported data on distant recurrence; there were no significant survival differences between the observation and adjuvant chemotherapy groups (OR, 1.49; 95% CI, 0.96–2.32; I2 = 0%) (Fig. 2C). On the other hand, there was only one study that reported data on CSS; therefore, we could not perform a metaanalysis on this outcome metric.
Sensitivity analyses using predefined methods indicated that the results of these meta-analyses were robust except for data on OS. Excluding one study with a large outlying effect [20], OS between the observation and adjuvant chemotherapy groups was not significantly different (OR, 1.48; 95% CI, 0.80–2.75; I2 = 27%).
Subgroup analysis of ypT0N0 rectal cancer patients
The oncologic effects of adjuvant chemotherapy were determined in 2 subgroups, according to the final pathologic stage. They were separately determined in patients with ypT0N0 and ypT1–2N0 rectal cancer who were treated with nCRT and radical surgery.
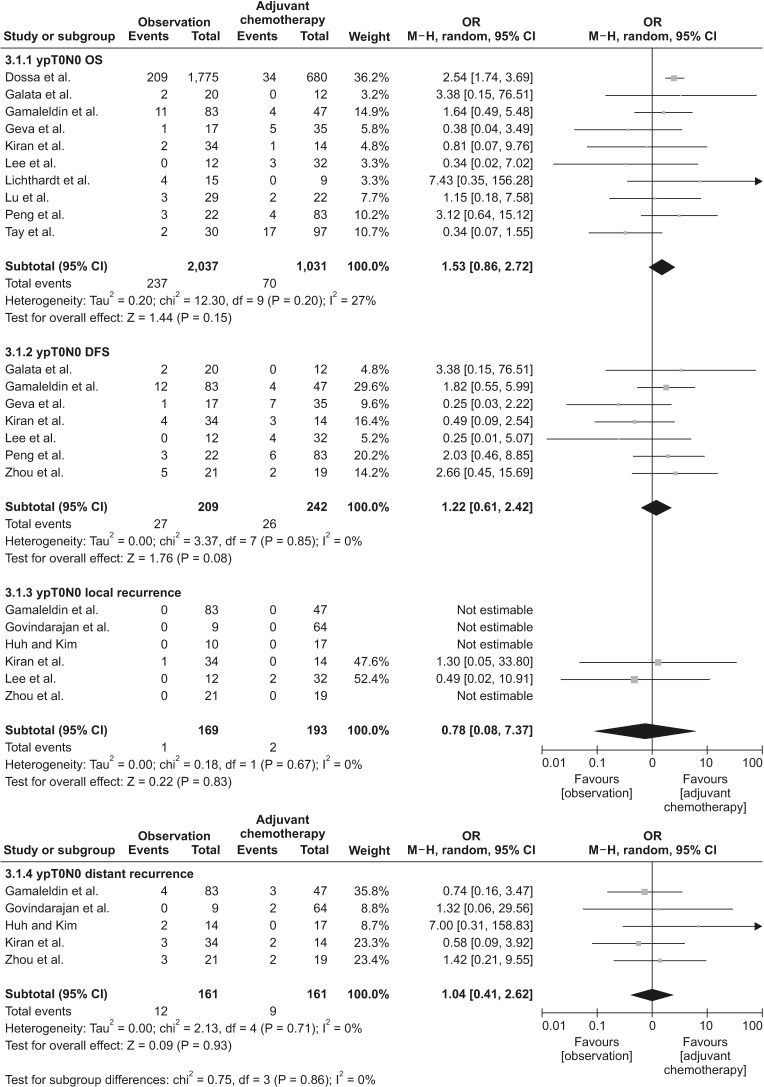
The first subgroup consisted of patients with ypT0N0 rectal cancer. The results show that adjuvant chemotherapy had no significant effect on OS (OR, 1.53; 95% CI, 0.86–2.72; I2 = 27%), DFS (OR, 1.22; 95% CI, 0.61–2.42; I2 = 5%), local recurrence (OR, 0.78; 95% CI, 0.08–7.37; I2 = 0%), and distant recurrence (OR, 1.04; 95% CI, 0.41–2.62; I2 = 0%) (Fig. 3).
Subgroup analysis of ypT1–2N0 rectal cancer patients
A second subgroup consisted of patients with ypT1–2N0 rectal cancer. The results show that adjuvant chemotherapy had no significant effect on OS (OR, 2.15; 95% CI, 0.59–7.80; I2 = 26%), DFS (OR, 1.66; 95% CI, 0.35–7.85; I2 = 44%), local recurrence (OR, 2.56; 95% CI, 0.72–9.13; I2 = 0%), and distant recurrence (OR, 1.15; 95% CI, 0.23–5.87; I2 = 0%) (Fig. 4).
Publication bias
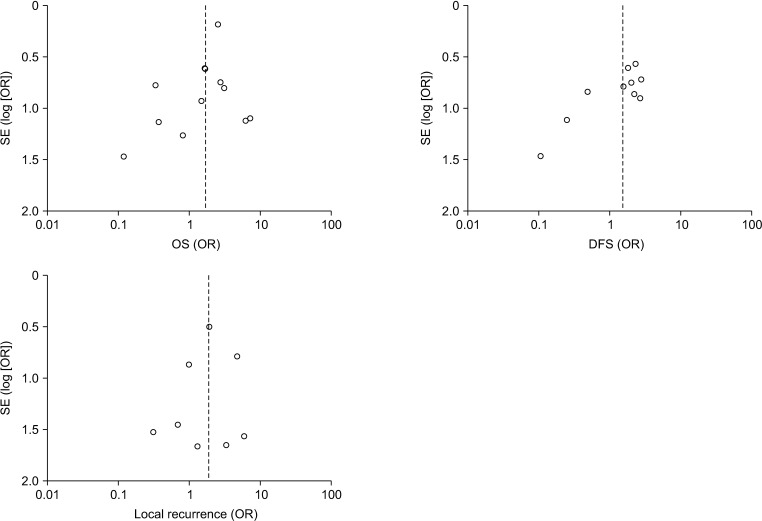
Publication bias was analyzed using the Egger weighted linear regression test, which assesses the asymmetry of funnel plots, and visual inspection of funnel plots (Fig. 5). The funnel plot for analysis of OS (P = 0.075) and DFS (P = 0.007) in patients with ypT0–2N0 was found to be asymmetrical, indicating the presence of publication bias. However, the funnel plots for analysis of local recurrence (P = 0.31) in patients with ypT0–2N0 indicated no publication bias.
DISCUSSION
For patients with locally advanced rectal cancer who were treated with nCRT, transabdominal resection can be performed. According to the guidelines of National Comprehensive Cancer Networ, adjuvant chemotherapy is recommended to improve survival rates in these patients, regardless of their pathologic stage after surgery. The treatment strategy to use adjuvant chemotherapy has been guided by studies on colon cancer [343536], and has also been guided by the thesis that tumor downstaging after nCRT may suggest a favorable tumor biology that can be correlated with further responsivity to additional chemotherapy. The theory further suggests that patients with a proven responsivity to treatment may benefit from adjuvant chemotherapy insofar as potentially eliminating residual micrometastatic disease [3738]. Further, a recent meta-analysis demonstrated improved OS with adjuvant chemotherapy in patients with a downstaged tumor following nCRT and radical surgery [10].
However, in clinical practice, patients' compliance with adjuvant chemotherapy is poor, with only about half to two-thirds of patients continuing with it [3940]. Further, adjuvant chemotherapy after local treatment is usually not well tolerated and often cannot be completed by older patients and those with comorbidities. In addition, patients with a positive response to nCRT are expected to have improved outcomes, and adjuvant chemotherapy may not be needed for them [929]. Some studies showed that patients with ypT3–4 or ypN+ rectal cancer that were treated with nCRT and radical surgery had worse oncological outcomes where adjuvant chemotherapy was required; whereas patients with a positive response to nCRT, such as ypT0–2N0 rectal cancer, were expected to have improved survival outcomes and may not need adjuvant chemotherapy [929]. Therefore, the hypothesis that adjuvant chemotherapy is beneficial for ypT0–2 rectal cancer patients needs better evidence for confirmation. However, the only previous meta-analysis on this topic did not focus on patients with ypT0–2N0 rectal cancer, so we performed the present meta-analysis. To our knowledge, the present study is the first meta-analysis evaluating the effect of adjuvant chemotherapy in patients with ypT0–2N0 rectal cancer after nCRT and radical surgery.
Our primary analysis of ypT0–2N0 rectal cancer patients indicated that adjuvant chemotherapy was associated with better OS, but there were no associations between adjuvant chemotherapy and DFS, local recurrence, and distant recurrence. However, the studies included in patients with ypT0–2N0 were heterogeneous in terms of groups of participants. To account for this affect, it was necessary to perform sensitivity analysis for confirmation of robustness in this meta-analysis. As a result, although there was a survival difference in the analysis of OS, adjuvant chemotherapy was not associated with better OS after excluding one study in a sensitivity analysis. In that case, the primary result for OS was modified by excluding a study that assessed a large number of patients with ypT0N0 disease only, as inclusion of such a large study with ypT0N0 patients would inaccurately distort the results [20]. Eventually, we found that subgroup analysis separating into ypT0N0 and ypT1–2N0 patients provided a more robust analysis.
Subgroup analyses, in terms of OS, DFS, and local and distant recurrence, determined no oncologic effects of adjuvant chemotherapy, both for patients with ypT0N0 and ypT1–2N0. Although patients with ypT0–2N0 rectal cancer are regarded as responding well to nCRT, there was a need to explore patients with ypT0N0 and ypT1–2N0 separately. There were 2 studies reporting ypT stage as a prognostic predictor [833] and another reporting ypN stage as an independent prognostic factor influencing oncological outcomes [41]. These studies may suggest that final TNM staging could help predict oncological outcomes [3842]. Tumor response to nCRT can range from no response to a complete pathological response (pCR), where no tumor is seen in the specimen subsequent to rectal resection. This response may also help predict overall prognosis, as patients with pCR (ypT0N0) appear to have improved survival prognosis in general [4344]. In addition, a study reported that dividing patients between ypT1–2N0 and ypT0N0 showed that response to nCRT in ypT1–2N0 patients treated with adjuvant chemotherapy had a significantly longer recurrence-free time [45]. Therefore, separating into 2 subgroups was more reasonable to determine oncologic effects of adjuvant chemotherapy.
According to the results of this meta-analysis, adjuvant chemotherapy may be an overtreatment for patients with ypT0N0 and ypT1–2N0 rectal cancer after nCRT and radical surgery, as it may lead to a lack of benefit regarding oncologic outcomes along with the adverse effects of the therapy itself. Such chemotherapy may delay recovery from the surgery and delay closure of ileostomy. Nevertheless, this meta-analysis has several limitations. First, it was based on an analysis of nonrandomized studies. Second, there could be a potential heterogeneity across the included studies, even though subgroup and sensitivity analyses were performed. For example, there were clinical differences regarding radiation dose and chemotherapeutic agents during nCRT. In addition, the regimen of adjuvant chemotherapy and duration of its use also varied among the included studies. Third, although 5-year survival rates and recurrence rates were outcome measures, there were differences in the median follow-up period among the included studies, which may affect oncologic outcomes.
In conclusion, based on this meta-analysis, patients with ypT0–2N0 rectal cancer after nCRT and radical surgery may not benefit from adjuvant chemotherapy with respect to long term oncologic outcomes, including OS, DFS, and local and distant recurrence. Therefore, routine use of adjuvant chemotherapy for those patients may be avoided but selective use of adjuvant chemotherapy is recommended. As this is a meta-analysis of non-randomly controlled studies, a random controlled trial would provide a higher degree of evidence to confirm this result.


 XML Download
XML Download