

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Liver cirrhosis (LC) is a pathological condition where long-term fibrous scarring of the liver owing to persistent inflammation caused by hepatitis virus infection or alcohol consumption leads to the loss of liver function [1]. A deepening pathophysiological understanding of LC and advances in treatment methods, such as liver transplantation, have led to longer life expectancies in patients with LC; however, no notable improvements in postoperative morbidity and mortality rates have been observed [23]. The reported morbidity rates of patients with LC are 30.1%–43% after nonhepatic abdominal surgery, while the reported mortality rates range between 11.1% and 35.8% [456].
Colorectal cancer (CRC) is the fourth most common cancer worldwide accounting for 6.1% of newly diagnosed cancers annually, and is the third leading cause of cancer-related deaths with a mortality rate of 5.8% [7]. Its incidence is rapidly increasing in South Korea owing to the rising popularity of Western diets in recent years [8]. A previous study found evidence of an increased risk of CRC in patients with LC [9]; the management of such patients requires a thorough understanding of the 2 diseases. While CRC and LC have been investigated separately in previous studies, the prognoses and postoperative outcomes of patients with CRC complicated with LC remain understudied. Among patients with CRC, we previously reported a significantly lower 5-year survival rate in those who also had LC (46.7%) than in those who did not (76.2%). We also derived a modified model that includes the serum sodium score that can serve as a prognostic predictor for patients who have both CRC and LC [4]. However, our previous study had a limited sample size; therefore, we performed this study to compare oncological and surgical outcomes between patients with CRC who had LC and those who did not using a nationwide cohort. Furthermore, we examined the respective effects of CRC and LC on the patients' prognoses and surgical outcomes by comparing them to members of the general public who were either healthy or have only LC.
METHODS
This study was approved by the Institutional Review Board of Dongnam Institute of Radiological and Medical Sciences (No. D-1807-007-002). It was also approved by the National Health Insurance Service (NHIS) Research Committee (NHIS-2018-1-378), and data customized by NHIS researchers were provided.
Data source and study design
We performed a nationwide retrospective study using health insurance claim data provided by the NHIS (Republic of Korea), which covers approximately 97% of all medical care and is considered representative of the South Korean population [10]. We included patients who were diagnosed with CRC and underwent resection between 2008 and 2013; there were 105,754 such patients identified. CRC was diagnosed per the Korean Classification of Diseases (KCD) codes, and resection was confirmed according to surgical codes. Patients diagnosed with any other type of cancer within 2 years before the surgery were excluded (n = 39,162). Patients with CRC who underwent resection were also excluded if (1) we were unable to identify their basic demographic characteristics (n = 1,206), (2) the location of CRC was unclear (n = 6,826), or (3) they were younger than 19 years of age at the time of diagnosis (n = 22). Of the remaining 58,538 patients, 453 developed LC within 2 years before surgery; LC was confirmed using the KCD codes. Each patient with both CRC and LC was matched with 2 patients with CRC but without LC according to sex, age (5-year intervals), and year of surgery. Furthermore, CRC patients with and without LC were matched patients without CRC but with LC and patients without CRC and LC, respectively. Upon matching, sex, age (5-year intervals) and the same year were matched, and then patients were randomly extracted at this ratio of 1:2. Therefore, CRC patients with LC, CRC patients without LC, patients without CRC but with LC, and patients without CRC and LC were matched at a ratio of 1:2:2:4. As a result, 453 patients with CRC and LC (the CRC-LC group), 906 with CRC but without LC (CRC group), 906 subjects with LC alone (LC group), and 1,812 healthy patients (control group) were analyzed.
Variable definitions
We considered the effects of basic demographic characteristics,
location of CRC, stage of CRC, and surgical method on survival. For basic demographic characteristics, we considered age, sex, and socioeconomic status (SES); the latter was based on the level of insurance premium, which ranged from 0 to 20 (the higher the insurance premium level, the higher the SES). As the survival rates of patients with CRC differ depending on the tumor's location (i.e., the left versus right colon), C185, C186, C187, C19, and C20 codes were classified as left-sided CRCs while C180, C181, C182, C183, and C184 were classified as right-sided. As with all types of cancer, the tumor stage (which is a significant predictor of survival) was determined by whether chemotherapy or radiotherapy were administered; if codes denoting chemotherapy or radiotherapy administration were noted in the patient's medical records 1 year before and after the surgery date, the patient was classified as having advanced-stage CRC. Incisional hernia and ileus were confirmed via KCD and surgical codes. We also considered the surgical method as a covariate; there were 2 types of surgical CRC resection: laparoscopic and open. Lastly, the Charlson comorbidity index (CCI) was included as a covariate, and was calculated by using the CCI calculation algorithm in the analytical manual published by the Health Insurance Review & Assessment Service [11].
Statistical analysis
The t-test and chi-square test were performed to determine any differences in the means of continuous and categorical variables, respectively, between patients with and without LC. Kaplan-Meier survival curves were plotted for patients with and without LC according to the covariates. The effect of LC on the survival of patients with CRC was tested using a Cox proportional hazards model. For this analysis, the history of CRC and LC, CRC stage, location of CRC, SES, CCI, and surgical method were used as covariates. Sex, age, and year of surgery were not considered covariates because they were used to match patients with and without LC. All statistical analyses were performed using the R statistical software ver. 3.5 (R Foundation for Statistical Computing, Vienna, Austria), and figures were plotted using the Rex software [1213]. P-values of <0.05 were considered statistically significant.
RESULTS
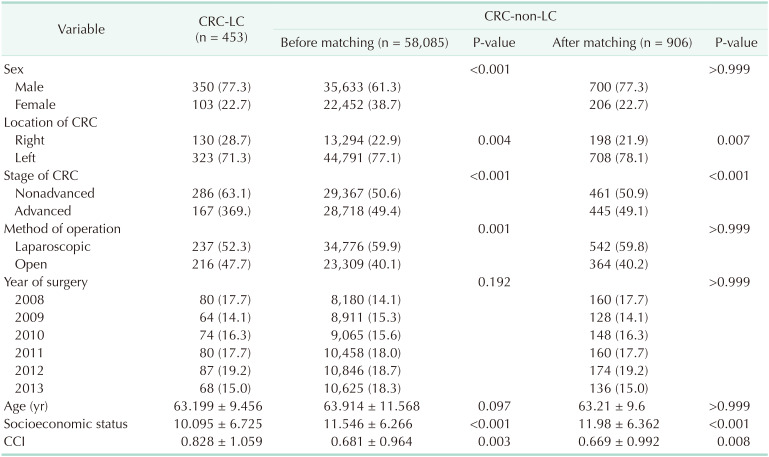
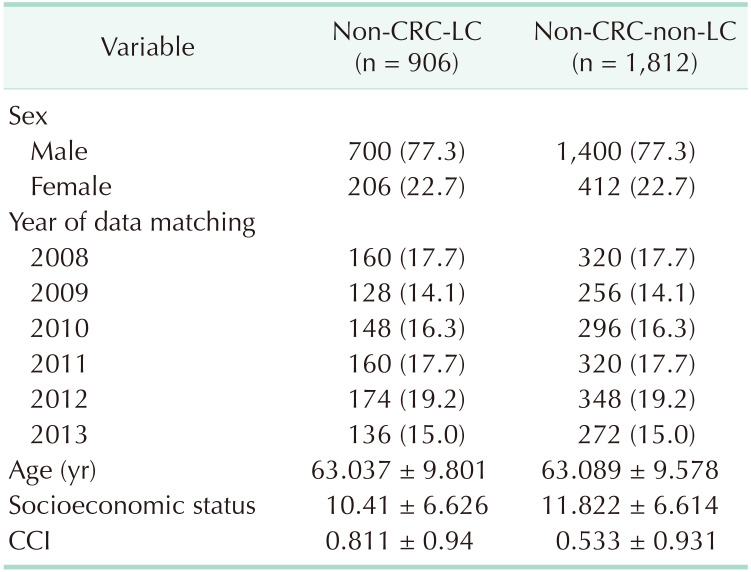
There were 453 patients in the CRC-LC group and 58,085 in the CRC group who underwent surgery for CRC; the characteristics of these patients before and after matching are summarized in Table 1. Compared to the CRC group, the CRC-LC group had a higher percentage of nonadvanced, right-sided CRC and lower SES. Table 2 shows the comparisons of 906 LC-group patient and 1,812 healthy controls.
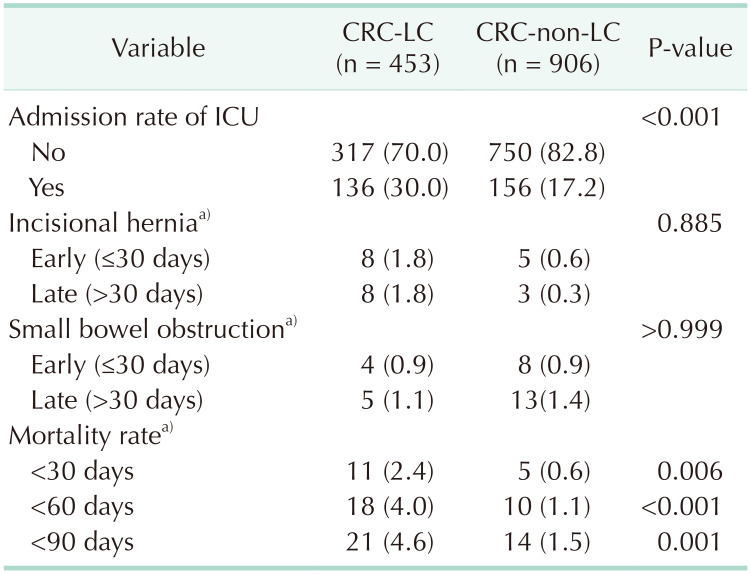
Patients in the CRC-LC group had a higher frequency of intensive care unit (ICU) admission than did those in the CRC group. There were no differences between the 2 groups in the incidences of early (≤30 days) and late (>30 days) postoperative small bowel obstruction and incisional hernia. However, their mortality rates were significantly different, as the 30-day (2.4% vs. 0.6%, P = 0.0058), 60-day (4.0% vs. 1.1%, P < 0.001), and 90-day (4.6% vs. 1.5%, P = 0.0013) mortality rates were all significantly higher in the CRC-LC group than in the CRC group (Table 3).
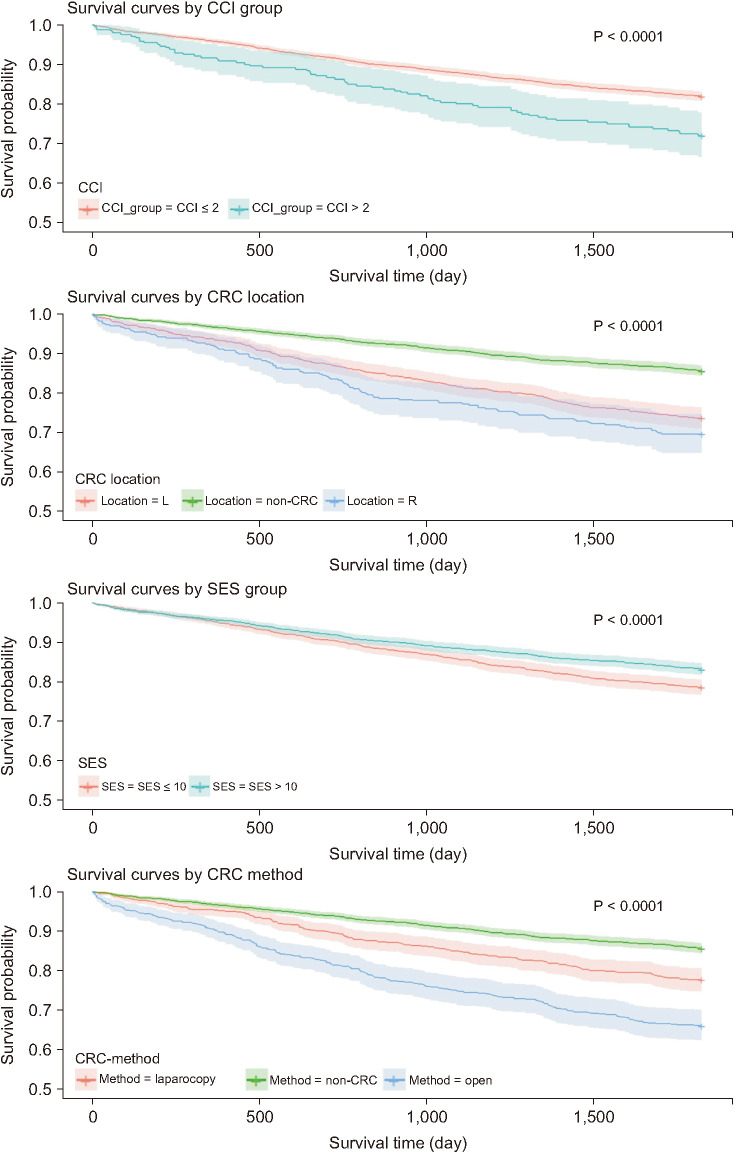
Patients presenting with underlying LC had a significantly lower survival rate than those without LC. The CRC-LC group had the lowest survival rate (with statistical significance), followed (in order) by the LC, CRC, and control groups. The survival rate of patients with CRC (i.e., the CRC-LC and CRC groups) was significantly lower than that of patients without CRC (the LC and control groups). When patients with CRC were divided into the nonadvanced and advanced disease groups, the control group showed the highest survival rate, followed by the nonadvanced CRC, advanced CRC, LC, nonadvanced CRC-LC, and advanced CRC-LC groups (Fig. 1). In terms of other investigated covariates, a higher CCI, right-sided CRC, SES ≤10, and open surgery were associated with a significantly lower survival rate (Fig. 2).
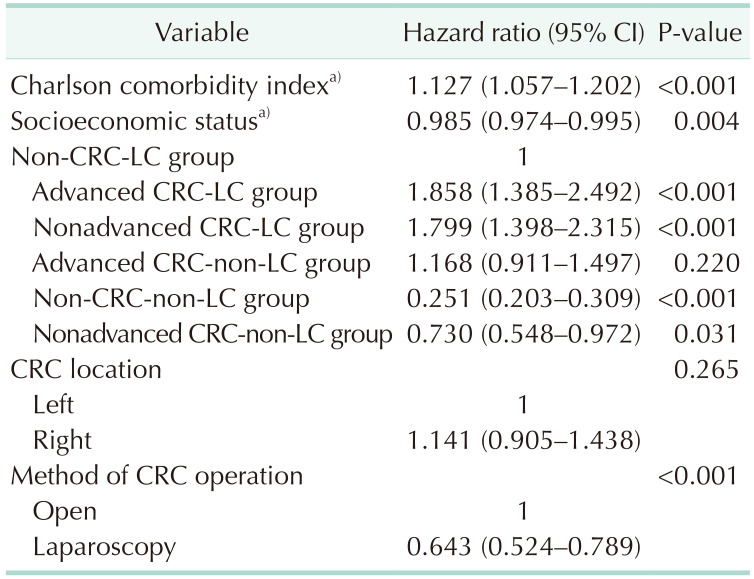
Of the factors influencing the 5-year survival rate, a higher CCI and higher SES were associated with significantly higher and lower risks of death, respectively; the risk was significantly lower in patients who underwent laparoscopic surgery. Patients in both the advanced and nonadvanced CRC-LC groups had significantly higher hazard ratios (HRs) than did those in the LC group; however, the control and nonadvanced CRC groups had lower HRs than the LC group (Table 4).
DISCUSSION
This study examined the survival rates of healthy subjects, patients with LC alone, patients with CRC alone, and patients with both LC and CRC. Furthermore, the CRC patients' surgical and oncological outcomes were investigated based on the presence or absence of LC. Our findings suggest that LC determines the prognosis of patients with CRC regardless of the tumor's stage (i.e., advanced or nonadvanced). Additionally, the prognoses of patients without LC could depend on the stage of CRC. Given the paucity of research on the prognoses and postoperative outcomes of CRC patients with LC, this study had the advantage of investigating a national cohort.
The significantly high proportion of nonadvanced CRC in the CRC-LC group can be attributed to higher chances of discovering CRC in patients who have underlying LC. It is recommended that patients with LC seek routine screening for early detection of primary liver cancer [1415]; a periodic health screening program is available in South Korea for the general public [16]. A previous study found that the postoperative ICU admission rate in the CRC-LC group was 14.5%, which was significantly higher than the rate of 4.1% observed in the CRC group [4]. Our study showed the same trend, although the rates in both groups were higher (30.0% vs. 17.2%). This difference may be owing to the selection bias in single-institution studies and variations in ICU admission criteria.
Treating patients with both CRC and LC involves longer hospital stays and (consequently) higher medical costs [17]. Such patients also require continuous outpatient follow-up and necessary procedures more frequently than do patients with CRC patients who have no LC. As such, we observed that a higher SES (which was a prognostic factor in this study) was associated with a lower HR. The CCI has also previously been found to be a significant prognostic factor in patients with CRC [181920]. Likewise, the HR was significantly higher in patients with increasing CCIs.
Our multivariate analysis aimed at identifying factors that influence survival rates showed a significantly elevated HR when CRC occurred in patients with LC. There was a significant difference between the advanced CRC-LC group (HR, 1.858) and the nonadvanced-CRC-LC group (HR, 1.799); that both groups had HRs >1 indicated that CRC in patients with underlying LC was associated with a worsened prognosis regardless of CRC stage. Furthermore, the HR of the control group was 0.251 when using the LC group as a reference, which is consistent with data from previous studies that showed worsened prognoses in patients with CRC who had underlying LC than in those who do not. The nonadvanced CRC group had no survival advantages over the advanced CRC group, but did have a significantly lower HR (0.730) than that of the LC group. This indicates that LC has a greater influence on survival than CRC stage, and that the absence of LC in patients with CRC is associated with a significantly better prognosis.
This study also revealed significant differences in survival rates based on surgical methods and other prognostic factors. Laparoscopic surgery is currently performed for T4a and T4b cancers, and positive results are shown accordingly. However, the authors think that in the period of this study (2008–2013), open surgery was performed for T4a and T4b advanced CRC patients relatively and the prognostic factor was analyzed. Previous studies found that 7.3% and 12.7% of CRC patients with and without LC underwent laparoscopy, respectively [4]. Likewise, laparoscopy was significantly less frequent in our CRC-LC group (52.3%) than in our CRC group (59.9%). This difference is possibly attributable to a higher likelihood of poor prognosis in patients undergoing open surgery.
This study had some limitations. First, the nationwide data contain no information on recurrence or cancer stage. Some previous studies found that LC in patients with CRC influences the location of recurrence [2122]; however, we could not confirm this in our study. Patients with advanced and nonadvanced CRC in our study were examined separately based on the administration of cancer treatment. Moreover, 74%–78% of patients with CRC underwent postoperative cancer treatment, the administration of which is an indicator of cancer stage; as such, we modified the study design based on this indication [23]. Furthermore, the severity of LC was not investigated and we could not examine the differences in survival rates based on the commonly used Child-Pugh classification or the ‘model for end-stage liver disease’ score. In the future, we believe it is necessary to conduct research involving liver function.
In conclusion, patients with CRC who had underlying LC had a lower survival rate than did those without LC, although there were no differences in the incidences of postoperative complications. LC was associated with a significantly lower survival rate regardless of the CRC disease stage. Given the high postoperative mortality of patients with LC, caution is advised when planning and performing surgery; importantly, liver function (among other factors) should be taken into consideration. We also recommend careful postoperative management for patients with both CRC and underlying LC.

 XML Download
XML Download