

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer is the third most malignant cancer in the world and it is the second most common cancer after stomach cancer in Korea according to the National Cancer Registry in 2015 [12]. Therefore, diagnosis and management of colorectal cancer are very important. Precise staging should be a basic tool for evaluating cancer, and the American Joint Committee on Cancer (AJCC) guideline for TNM staging is most widely used in colorectal cancer as well as in many other cancers. This staging system can predict cancer prognosis and can be used as a guideline for determining postoperative management policy. Therefore, accurate staging is clinically important. TNM staging is based on pathologic examination, and the tumor is similarly evaluated using TNM staging in preoperative imaging. In general, the accuracy of imaging tests is lower than the accuracy of histologic examination, especially for N stage [345]. To increase the accuracy of evaluation, various tests are performed before surgery and evaluated comprehensively [678910]. Nevertheless, current examinations are limited since there are some differences between staging before and after surgery.
The postoperative stage is occasionally different from the stage predicted before surgery, which makes it difficult for the clinician to trust the diagnosis and define a treatment plan. In colon cancer, a preoperative suspected cT4 stage can often be diagnosed as pT3 after surgery. In these cases, preoperative clinical and imaging staging were very reliable, leading to challenges in determining which results to trust [111213]. Since there are concerns around whether pathologic T3 is understaged, there are also concerns around undertreatment. However, there are few studies on the accuracy of pathologic diagnosis, especially for T stage. Therefore, this study was planned to confirm the diagnostic accuracy of the postoperative pathologic results by comparing the survival of patients who were suspected of cT3 and cT4 before surgery and who were diagnosed with pT3 after surgery.
Go to : 
METHODS
We reviewed the data of patients who underwent surgical resection for colon cancer from September 2006 to September 2016, and who were diagnosed with pathologic T3 stage cancer with or without lymph node metastasis. Patients with preoperative clinical T3 or T4 stage cancer were selected. Clinical T4 was defined as free perforation, localized peritumoral abscess, and direct invasion of an adjacent organ [14]. Patients diagnosed with primary colon cancer with pathologically proven adenocarcinoma from the cecum to the sigmoid colon were included in this study. The exclusion criteria were as follows: patients with appendiceal or rectosigmoid colon cancer, patients with multiple colon cancers, patients with distant metastasis, or patients who had undergone neoadjuvant treatment. This study was approved by the Institutional Review Board (IRB) of Korea University Anam Hospital (IRB No. 2019AN0071), and all patients had provided informed consent.
All patients with colon cancer had been evaluated preoperatively by physical examination, total colonoscopy, abdominopelvic CT, chest CT, and routine laboratory, which included tests for tumor markers. In cases of postoperative stage 2 disease with risk factors or stage 3 disease, oxaliplatin-based adjuvant chemotherapy was performed for 8–12 cycles. In patients who had undergone chemotherapy, laboratory tests, which included CEA, and abdominopelvic CT were performed at 3–4 cycle intervals during chemotherapy. Other examinations such as chest CT, colonoscopy, and PET-CT were added when necessary. Radiation therapy was determined after a multidisciplinary team discussion for cases where there was suspicion of peritoneum or abdominal wall involvement, or if there was a high risk of recurrence in a locally limited area before or during surgery. After adjuvant treatment, follow-up examinations were carried out at 3-month intervals during the first 2 years postoperatively, at 6-month intervals until 5 years after surgery, and then annually if there was no evidence of recurrence.
Data for cT3 and cT4 groups were compared in terms of patient demographics, tumor characteristics, operative and postoperative outcomes, pathologic results, and oncologic outcomes. Descriptive results are presented as a mean with standard deviation or median with interquartile range for continuous outcomes and as frequency and percentage for categorical outcomes. Student t-tests were used to compare continuous variables, and the chi-square test or Fisher exact test was applied for categorical variables. Five-year overall survival (OS) and recurrence-free survival were analyzed using the Kaplan-Meier method. Comparison of survival between groups was performed by log-rank test. Univariate and multivariate analyses of clinicopathologic factors were performed by the Cox regression analysis in order to determine prognostic factors of survival. Statistical analysis was performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA). A P-value <0.05 was considered statistically significant.
Go to :
RESULTS
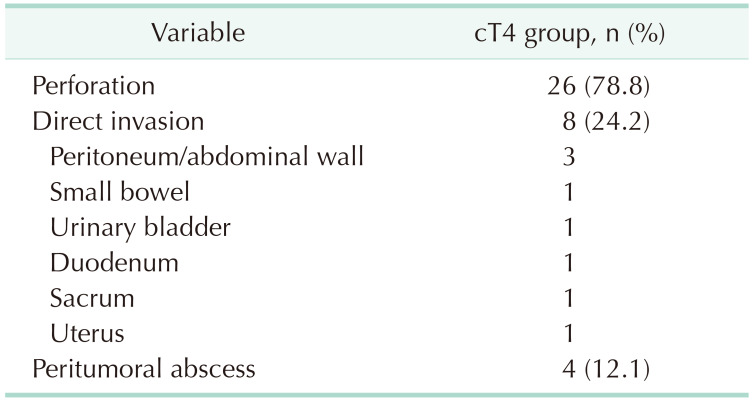
A total of 536 patients were included in the study. In the patient population, 503 had clinical T3 (93.8%), and 33 had clinical T4 (6.2%). Table 1 summarizes the reasons for the stage 4 diagnoses in the cT4 group. The most common finding was free perforation (26 patients, 78.8%), followed by direct invasion of adjacent organs (24.2%). The most commonly invaded organ was the peritoneum or abdominal wall, followed by the small bowel or urogenital organ. Four patients had suspected localized peritumoral abscess (12.1%).
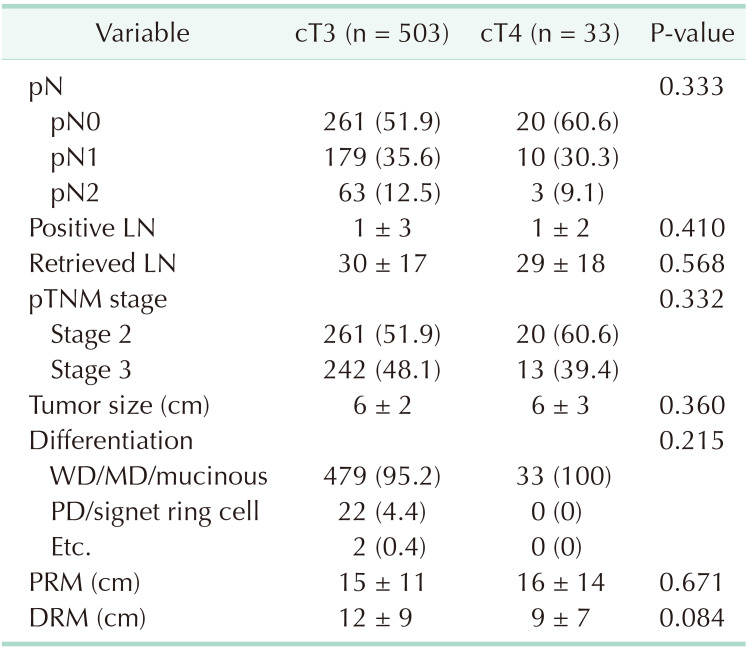
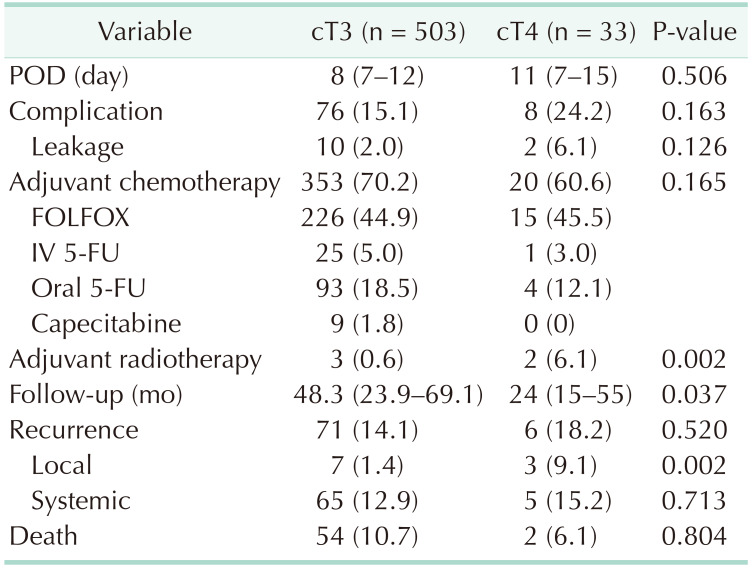
In the cT4 group, the proportion of sigmoid colon cancer was high (38.8% vs. 63.6%), whereas the proportion of right colon cancer was high in the cT3 group (43.3% vs. 15.2%, P < 0.001) (Table 2). In the cT4 group, the rate of emergency surgery was high (1.6% vs. 30.3%, P < 0.001), and the rate of open surgery was high (4.0% vs. 27.3%, P < 0.001). In terms of operative procedure, the cT3 group was more likely to undergo right colonic resection (50.3% vs. 24.2%), while the cT4 group was significantly more likely to undergo Hartmann's procedure (0.4% vs. 24.2%, P < 0.001). Estimated blood loss was also higher in the cT4 group (95 mL vs. 287 mL, P < 0.001). The rates of combined resection and operation time were higher in the cT4 group, but the results were not statistically significant (6.4% vs. 15.2%, P = 0.054; 182 minutes vs. 203 minutes, P = 0.079, respectively). There were no significant differences between the 2 groups in terms of pathologic results (Table 3). There were no differences in postoperative stay, complication, and adjuvant chemotherapy, but the rate of adjuvant radiotherapy in the cT4 group was high (0.6% vs. 6.1%, P = 0.002).
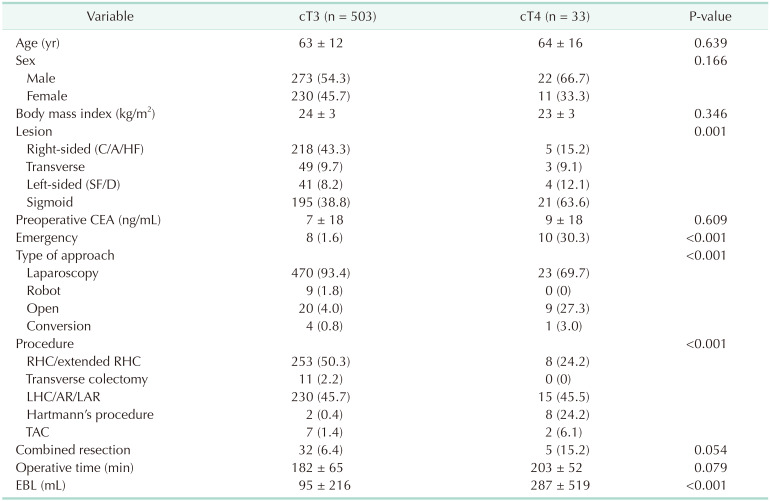
Table 2
Patient demographics and operative outcomes
Values are presented as mean ± standard deviation or number (%).
BMI, body mass index; C, cecal; A, ascending; HF, hepatic flexure; SF, splenic flexure; D, descending; RHC, right hemicolectomy; LHC, left hemicolectomy; AR, anterior resection; LAR, low anterior resection; TAC, total abdominal colectomy; EBL, estimated blood loss.
![]()
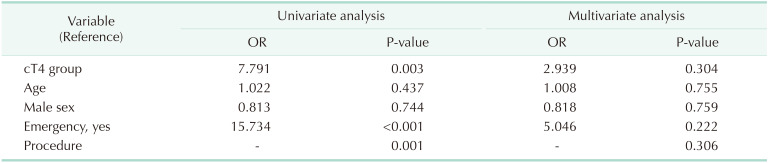
Median follow-up periods for the cT3 and cT4 groups were 48.3 months and 24 months, respectively, and the shorter follow-up period for the cT4 group was significant (P = 0.037). On the other hand, local recurrence was significantly higher in the cT4 group (9.1%) than in the cT3 group (1.4%) (P = 0.002) (Table 4). The 5-year OS was 87.7% in the cT3 group and 79.6% in the cT4 group; the difference was not statistically significant (P = 0.470). There was no difference in 5-year total disease-free survival (DFS) between the cT3 and the cT4 groups (82.7% vs 71.5%, P = 0.286). However, the 5-year local DFS was significantly worse in the cT4 group than in the cT3 group (98.6% vs. 84.0%, P < 0.001) (Fig. 1). When performing subgroup analysis according to stage, in stage 2, only 5-year local DFS varied between the 2 groups (99.6% vs. 88.1%, P < 0.001). On the other hand, in stage 3, no measures of survival differed between the 2 groups. In the univariate analysis, cT4, emergency surgery, and operative procedure were risk factors for local recurrence. However, multivariate analysis showed no statistically significant risk factors (P = 0.056) (Table 5).
 | Fig. 1Five-year overall (A), total disease-free (B), systemic disease-free (C), and local disease-free (D) survivals in the cT3 and cT4 groups.
|
Go to :
DISCUSSION
In our study, patients who had suspected cT4 before surgery but had been diagnosed with pT3 after surgery were more likely to have perforation, and local recurrence was significantly higher in these patients. This implies that preoperative cT4 patients have a worse prognosis. Therefore, the cT4 group should be treated more aggressively after surgery. However, according to our results there was no difference in adjuvant chemotherapy between the cT3 and cT4 groups. Following the National Comprehensive Cancer Network guidelines [15], we recommended adjuvant chemotherapy for either stage 2 cancer that is associated with preoperative obstruction or perforation or stage 3 disease; however, these principles were not always applicable.
This phenomenon seems to be due primarily to the influence of pathologic staging. Because there is high regard for pathologic staging as an errorless and immutable result, we are dependent on pathologic staging in determining a treatment plan. As compared to clinical staging, which is generally dependent on the preoperative imaging tests, postoperative pathologic results are thought to be highly accurate and have been the standard for treatment plans. However, actual results may be inaccurate because the opinion of the pathologist is reflected in the postoperative pathologic results. In particular, gross examination is very important and requires a discussion between the surgeon and the pathologist with regard to the surgical specimen [16]. For example, in the case of a cancer with perforation, this can be diagnosed as T4 due to the identification of a nonconsecutive serosal lining through finding an accurate perforation site, otherwise a T4 diagnosis is difficult pathologically.
In our study, the proportion of patients with suspected cT4 due to perforation was relatively high. Perforation often cannot be detected during pathologic examination, and thus understaging as pT3 can occur in these patients. In these patients, clinical stage may have been more important in determining the postoperative treatment plan because the reliability of the clinical or imaging results was relatively very high [111213]. These patients are likely to have been treated with an adjuvant treatment based on the postoperative pT3. In addition, the condition of the patient after surgery may have influenced the adjuvant treatment. For this reason, there was no difference in adjuvant chemotherapy between the cT3 and cT4 groups.
Therefore, it should be noted that the diagnostic accuracy of pathologic results may also be inaccurate, and a discussion between the surgeon and pathologist would be needed for accurate oncological evaluation. Fortunately, the 8th edition of the AJCC guideline specifies the definition of pT4a [14]. Unlike the previous version, which defines T4 as simply “tumor penetration to the surface of the visceral peritoneum,” T4 is specifically defined in the 8th edition as “tumor invades through the visceral peritoneum (including gross perforation of the bowel through tumor and continuous invasion of tumor through areas of inflammation to the surface of the visceral peritoneum).” Although it remains controversial, it seems to reflect a willingness to diagnose more actively than before.
In our study, postoperative local recurrence of cT4 patients was similar to those of other studies [171819202122]. If the tumor invades the serosa, seeding tumor cells may remain in the peritoneal cavity. This is probably due to the presence of seeding tumor cells in the peritoneal cavity when the tumor invades the serosa. Considering these results, it is highly suggestive that a pT3 diagnosis after surgery is likely to be understaged. Therefore, if cT4 is clinically suspected before surgery, aggressive adjuvant treatment is required regardless of pathologic staging. If necessary, aggressive treatments, such as hyperthermic intraperitoneal chemotherapy or early postoperative intraperitoneal chemotherapy, may be considered. In cases of suspected abdominal wall or retroperitoneal invasion, intraoperative marking, and postoperative radiotherapy may be performed to reduce local recurrence.
A limitation of our study is that the analysis included various colon cancers. The colon has large differences in luminal diameter depending on whether it is right or left, and there are many differences in clinical features and surgical methods. Recently, there have been many studies by tumor sideness, in which there are differences in tumor biology between the midgut and hindgut [232425]. The basis for suspecting cT4 or the pattern of recurrence may be different between retroperitoneal colon (ascending or descending colon) and intraperitoneal colon (transverse or sigmoid colon). Therefore, a subgroup analysis can also be considered for accurate analysis of survival, especially local recurrence. Nevertheless, to our knowledge there have been no survival analyses according to preoperative staging in patients with pathologic T3 until this current study. Our study is important since it questions the accuracy of current pathologic examinations and confirms a correlation between clinical staging and oncologic outcome.
In conclusion, patients with colon cancer who were suspected of cT4 before surgery had a high local recurrence even after a T3 diagnosis on final postoperative pathology. Considering that the current pathologic exam has limitations in accurately diagnosing the T4 stage, the clinician should perform more aggressive adjuvant treatment in patients with colon cancer who have suspected preoperative T4 stage cancer. In addition, a discussion between the surgeon and the pathologist is needed for accurate T staging after surgery.
Go to :
 XML Download
XML Download