

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The discovery of minimally invasive surgical techniques has played an important role in the development of surgical treatment for gastric cancer. It is currently preferred over open surgery in early gastric cancer because of its low complication rate and enhanced surgical view [1]. Research concerning laparoscopic surgery has compared the oncological effects of surgical techniques through a series of randomized control trials and has found that minimally invasive surgery is not inferior to open surgery [23]. With the increasing survival rate of patients with gastric cancer, function preservation has become another key factor in gastric cancer surgery. Comparative trials of partial gastrectomy, including pylorus-preserving gastrectomy (PPG) or proximal gastrectomy (PG), are underway regarding long-term surgical outcomes [45]. Studies on surgical resection margin and safety have continuously been carried out [6]. In an atmosphere that emphasizes patient satisfaction, quality of life (QOL) after surgery has become a topic of increasing focus.
Systemic indicators have been developed to evaluate QOL after surgery. The commonly used QOL evaluation tools for gastric cancer include the quality-of-life questionnaire (QLQ)-C30 and QLQ-STO22 developed by the European Organization for Research and Treatment of Cancer (EORTC), which has good reliability and validity [7]. The Korean version of the EORTC QLQ-C30 was validated in 2004 and has been widely used in postoperative patient surveys [8]. Various comparative studies have been conducted using these indicators for QOL [9].
Laparoscopic gastrectomy requires a high degree of experience in lymph node dissection. It takes a long time to train a skilled laparoscopic surgeon. Robotic surgery, a modification of conventional laparoscopic surgery, is an emerging solution for this difficult laparoscopic training [10]. Robotic surgery requires a relatively short training period with a systemic assistant, and provides benefits such as an easy surgical view, free joint movement, and handshake correction [11]. Currently, the number of robotic surgeries is increasing worldwide. Although they emphasize the advantages of robotic surgery, many studies have reported limitations regarding single-institute and retrospective data collection. In a recent, multicenter prospective trial study comparing robotic gastrectomy with laparoscopic gastrectomy, no significant difference in outcomes was found between these two operations regarding operative bleeding, open conversion rate, and hospital stay [12]. We further analyzed the QOL in this study using the same data set as that of this multicenter prospective trial.
METHODS
Patients and treatment
A prospective multicenter study was conducted on patients who underwent laparoscopic or robotic gastrectomy at 11 hospitals in Korea between May 2011 and December 2012. The type of operation (extent of gastrectomy) was determined by the patient after a comprehensive understanding of the location of the tumor, clinical stage, and operative procedure. Investigators generally followed the international gastric cancer guideline of the Japanese Gastric Cancer Association [13]. This study was performed by surgeons who participated in the Korean Laparoendoscopic Gastrointestinal Surgery Study Group, and the laparoscopic or robotic procedures were accordingly standardized in the multicenter. The robotic procedure was performed using the da Vinci Surgical System (Intuitive Surgical, Sunnyvale, CA, USA). The adjuvant chemotherapy regimen (capecitabine plus oxaliplatin or S-1) was recommended for patients with pathological stage II or III disease in both the groups [1415]. We collected clinical information such as age, sex, weight, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status classification, tumor location, pathological stage, operation type, and approach of the anastomosis, accordingly for each subject. Pathological evaluation and staging were determined according to the 7th American Joint Committee on Cancer staging system.
Study design
Since the patients who chose robotic surgery group were fewer in number, we registered one laparoscopic surgical subject after recruiting one robotic surgical subject with the same surgeon, sex, and extent of gastric resection. The inclusion criteria were as follows: (1) a documented diagnosis of gastric adenocarcinoma, (2) minimally invasive gastric cancer surgery, and (3) no preoperative evidence of serosal invasion or extraperigastric lymph node metastasis during the preoperative examination. Exclusion criteria were as follows: (1) mental incompetency, (2) illiteracy, (3) pregnancy, or (4) aged younger than 20 years. A paper survey was given at 11 centers. The Korean version of the EORTC QLQ-C30 and EORTC QLQ-STO22 was used for the survey. The QOL questionnaire was collected at the time of preoperative admission, postoperative 1st outpatient department (OPD) visit (usually 2 weeks after discharge), followed by 3-month, 1-year, and 3-year OPD visits respectively, postsurgery. Patients who responded to 1 preoperative questionnaire and similarly gave their responses to at least one among the several questionnaires administered postoperatively were selected as the initial data set. We compared the data after dividing it into several types of characteristics as follows: device (robotic or laparoscopic), operation type (distal gastrectomy [DG], total gastrectomy [TG], or PPG), pathological stage (stage I or stage II–III), and sex (male or female). Each comparison used data set after propensity score matching.
Propensity score matching
In the comparative data set, biased components were extracted by logistic regression analysis. Propensity score matching (PSM) was applied to the initial data set by PSM tool in IBM SPSS Statistics ver. 25.0 (IBM Corp., Armonk, NY, USA) with biased components (confounders). Nearest-neighbor matching and 1:1 matching were used in the software as an option. Exceptionally, comparison by operation type did not adjust the bias according to the location of the tumor. The cases of PPG and PG were excluded from the initial data set during comparison of DG and TG. Similarly, for comparison of DG and PPG, the cases of TG and PG were excluded from the initial data set. Each comparison was performed using the respective logistic regression and PSM.
Outcomes
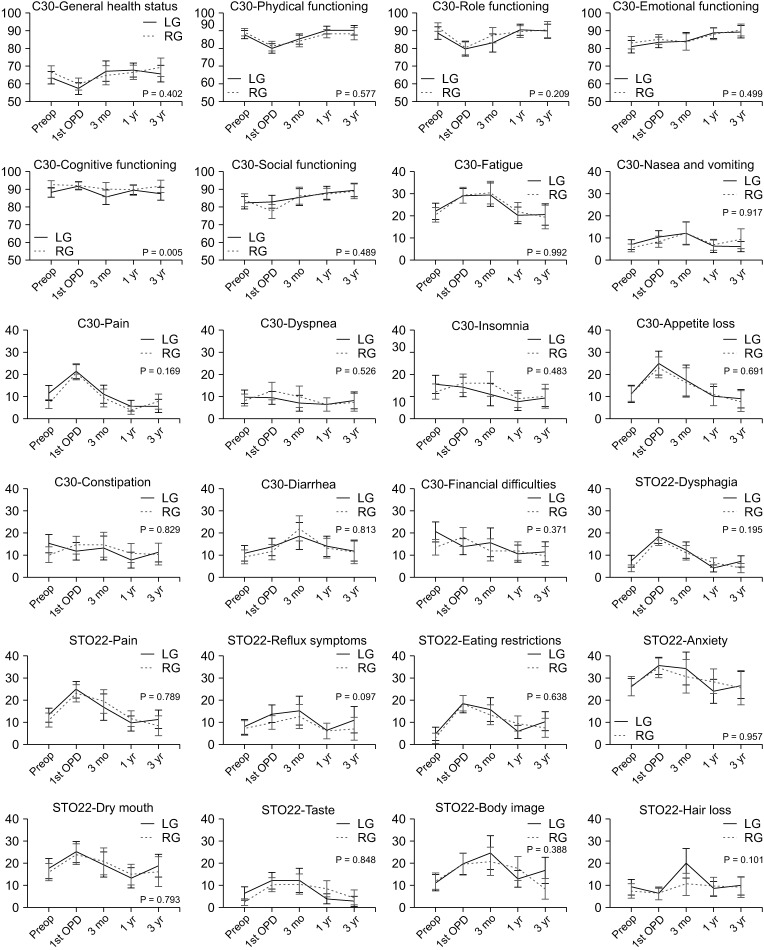
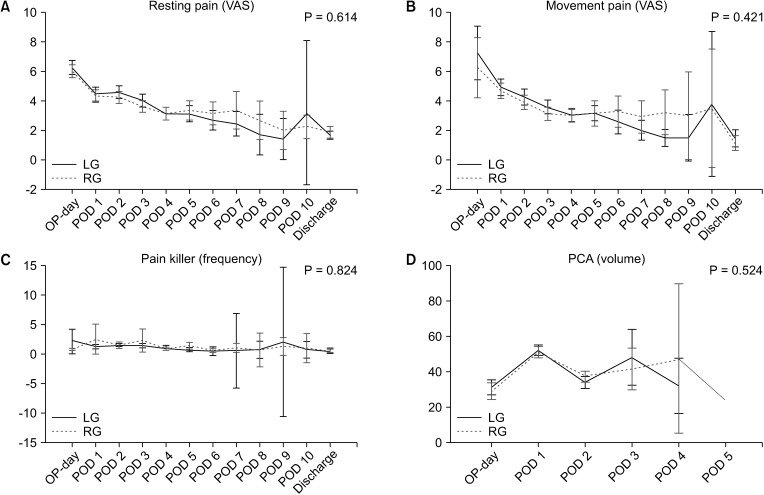
The primary outcome of this study was QOL after gastrectomy for gastric cancer. QLQ–C30 consists of 30 questions, which assess 15 scales; general health status, physical functioning, role functioning, emotional functioning, cognitive functioning, social functioning, fatigue, nausea/vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties. QLQ-STO22 consists of 22 questions, which assess 9 scales: body image, dysphagia, pain, reflux symptoms, eating restrictions, anxiety, dry mouth, taste, and hair loss. The secondary outcomes of this study were pain and long-term complications. Pain was assessed using the visual analog scale (VAS, 0–10) and therapeutic regimen for pain killer. The pain scale and the volume usage of patient-controlled analgesia (PCA) were checked on the operation day, postoperative day (POD) 1 to POD 10, and discharge day. Intestinal obstruction, stenosis, reflux, malabsorption, dumping, and delayed emptying, which appeared after 1 month of surgery, were monitored as long-term complications. Student t-test, chi-square test, and mixed analysis of variance (ANOVA) were used for comparative statistical analyses. All statistical analyses were performed at a significance level of 5% using IBM SPSS statistics.
Ethical standards
The study protocol was approved by the Institutional Review Boards of all participating institutions (No. H-1710-050-891, Seoul National University Hospital). This multicenter prospective study was approved by the responsible committee on human experimentation of the respective medical center and all procedures followed the Helsinki Declaration of 1964 and later versions of the same guideline. All patients signed an informed consent form before the study.
RESULTS
Demographics and propensity score matching
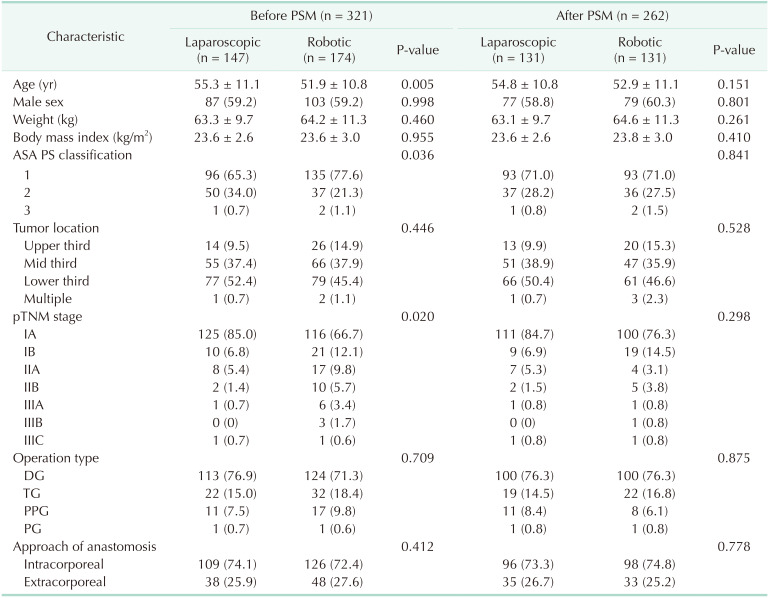
In the multicenter project, 434 patients (robotic 223 and laparoscopic 211) were enrolled from 11 centers. During the 5 surveys, 337, 302, 157, 220, and 165 patients answered at the time of preoperative admission, postoperative 1st OPD visit, and 3 months, 1 year, and 3 years later, respectively (Fig. 1). Among them, 321 patients responded to both the pre- and postoperative surveys: 72 patients answered at 1 preoperative and 4 postoperative surveys; 95 patients answered at 1 preoperative and 3 postoperative surveys; 117 patients answered at 1 preoperative and 2 postoperative surveys; 37 patients answered 1 preoperative and 1 postoperative survey. We compared these 321 patients accordingly on the basis of the following groups: (1) robotic vs. laparoscopic, (2) TG vs. DG, (3) PPG vs. DG, (4) stage I vs. stage II–III, and (5) male vs. female. Comparing the 147 patients in the laparoscopic group and the 174 patients of the robotic group, there was a significant difference in age, ASA physical status classification, and pathologic TNM; the patients in the robotic group were young and had an advanced pathological stage (Table 1). We adjusted the 2 groups into 262 patients (robotic 131 vs. laparoscopic 131) by PSM. A total of 46.6% (robotic) and 50.4% (laparoscopic) of tumors located in the lower third of the stomach. A total of 76.3% (robotic) and 84.7% (laparoscopic) of patients were in stage IA. A total of 76.3% of operations required DG. Intracorporeal anastomosis was performed in 74.8% (robotic) and 73.3% (laparoscopic) of cases.
Similar QOL between robotic and laparoscopic approaches
Twenty-four scales composed of general health status, 5 of C30 functioning scales, 9 of C30 symptom scales, and 9 of STO22 symptom scales were checked to compare robotic and laparoscopic surgery. Only C30-cognitive functioning was significantly different between the 2 groups (P = 0.005) (Fig. 2). The robotic group had better preoperative QOL in cognitive functioning than the laparoscopic group (P = 0.010) and the scale did not change over time (P = 0.053). General health status, physical functioning, and role functioning decreased in the immediate postoperative period and then recovered. The emotional and social functioning increased after the operation. Symptom scales, except for 2 scales, were increased and recovered serially after surgery; dyspnea and constipation scales did not change over time (P = 0.086 and P = 0.263, respectively).
Long-term complications and pain scores
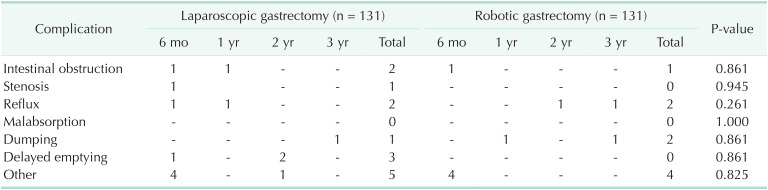
Considering 6 major complications (intestinal obstruction, stenosis, reflux, malabsorption, dumping, and delayed emptying), the incidence of any type of complication was as low as 9.2% (24/262) within 3 years after discharge (Table 2). Laparoscopic or robotic approaches did not show a significant difference in long-term complications. For example, the rate of delayed emptying was higher in the laparoscopic group (3/131 vs. 0/131, P = 0.861) without significance. Postoperative pain was compared using 4 indexes (the VAS of resting pain, the VAS of movement pain, the frequency of additional painkillers, and the volume usage of PCA). The score of resting pain and movement pain decreased daily from the highest score on the operation day; however, the usage of painkillers and PCA volume did not change significantly after the operation. There was no significant difference in the 4 pain indices between laparoscopic and robotic group (resting pain sore, P = 0.614; movement pain score, P = 0.421; pain killer, P = 0.824; PCA usage, P = 0.524) (Fig. 3).
Better quality of life of men, distal gastrectomy, and stage II–III across several parameters
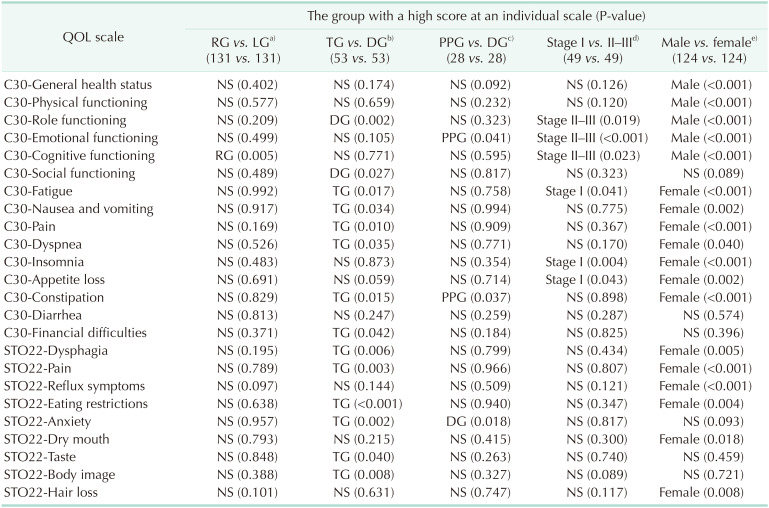
We compared TG and DG, PPG and DG, stage I and stage II–III, and male and female rather than a robotic and laparoscopic surgery from the initial data set (321 cases). A comparison between TG and DG was adjusted by PSM with 2 confounders, weight and the approach of the anastomosis. A comparison between PPG and DG was adjusted with weight and the approach of the anastomosis. A comparison between stage I and stage II–III was matched without a confounder. A comparison between male and female was matched with BMI as a confounder. DG showed better scores using 2 of C30 functioning scales, 6 of C30 symptom scales, and 6 of STO22 symptom scales than TG. DG was better in constipation but worse in emotional functioning and anxiety than PPG. Male patients showed better scores in general health status, 4 of C30 functioning scales, 7 of C30 symptom scales, and 6 of STO22 symptom scales than female patients. Stage II–III showed better scores at the 3 of C30 functioning scales and 3 of C30 symptom scales (Table 3).
DISCUSSION
Robotic surgery is a procedure with greater use of technology. Recently, robotic surgery has attracted the attention of people with respect to big data and artificial intelligence. However, robotic surgery is more expensive than conventional laparoscopic surgery. Therefore, we need to determine the advantages that offset its high cost. Comparative studies have been conducted to analyze the oncological effect, complications, and surgical performance (e.g., the amount of bleeding, length of hospital stay, and operation time) of robotic surgery [16]. Until now, it does not appear to be superior to conventional laparoscopic surgery for gastric cancer [1217].
In this study, robotic surgery was different from laparoscopic surgery only in the C30 cognitive functioning scale. This resulted from the difference in preoperative baseline measurements. For budget issues, this study could not randomize the robotic and laparoscopic groups. The cognitive functioning scale may be related to the economic background of patients who chose robotic surgery. Comparing the change before and after surgery, there was no difference noticed in QOL including cognitive functioning between robotic and laparoscopic surgery. Since the technology applied to robotic surgery has been upgraded continuously, the benefit for gastric cancer might be discovered in the future.
It is difficult to define an overall indicator by integrating individual scales, and it is difficult to clarify the cause-and-effect relationship. Nevertheless, the value of this study is that we tried a prospective approach to control the variables associated with QOL. This is the only prospective study that verified the QOL of robotic surgery for gastric cancer. Similar prospective studies of QOL were performed to compare open surgery and laparoscopic surgery or to compare the type of anastomosis [18].
In this study, DG received a good score on 14 items when compared to TG. That is consistent with the results from previous studies comparing DG and TG [719202122]. In fact, patients who underwent TG complained about weight loss and frequent bowel movement. In this study, the scores of nausea/vomiting, constipation, dysphagia, and eating restrictions of TG patients were found to be poor. Referring to an article published in 2016, the QOL comparison of TG and DG in our study is similar to theirs by 18 scales of 24 [22]. This study was derived from an earlier study comparing robotic surgery and laparoscopic surgery. There are limits to the population for analyzing these other factors, though.
We found 3 articles comparing QOL with the stage of gastric cancer. In one article, there was no significant difference in the QOL between stage I/II and III/IV [23]. In another article, there was no difference between the patients who underwent adjuvant chemotherapy and those who did not undergo adjuvant chemotherapy [24]. Nevertheless, another study published in 2018 showed that the role functioning scale and reflux scale were good in the advanced stage (>stage II); that is similar to our analysis [25]. It seems that the experience of survival from cancer might change the threshold of an individual's satisfaction.
We found that female patients had poor scores on many indicators; physical functioning, fatigue, nausea/vomiting, insomnia, appetite loss, diarrhea, dysphagia, pain, eating restrictions, anxiety, taste, and hair loss. Referring to the previous study, the QOL of the general population seems to be sexually biased [26]. Referring to a well-designed study that compared QOL before and after coronary artery bypass surgery, they concluded that the baseline level of QOL and the change of QOL by surgery differed according to sex [2728]. Interestingly, an article about gastric surgery presented results similar to ours in terms of sex differences [25]. Therefore, our clinicians might keep in mind that the ratio of males and females affects the outcomes of the QOL study.
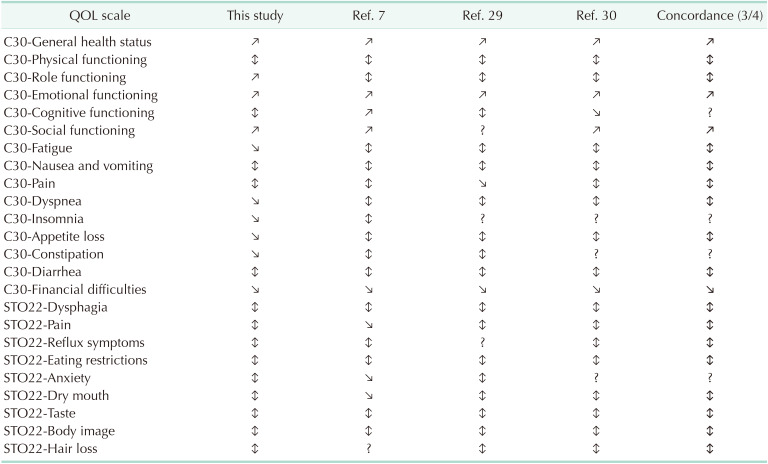
We examined the chronological changes of QOL for this study. We found 3 articles that described the chronological change of the QOL after gastrectomy; these studies were performed in Korea and Japan [72930]. We analyzed the line graph about QOL scales from these articles and arranged them in 3 categories as follows: (1) ‘recovery (↕)’ - functioning scale decreased and partially recovered, or symptom scale increased and partially recovered; (2) ‘increase (↗)’ - function scale finally increased over baseline; (3) ‘decrease (↘)’ - symptom scale finally decreased under the baseline (Table 4). We defined ‘concordance’ of a scale when 3 of 4 articles showed the same pattern of the scale. Therefore, C30-general health status, 4 of C30 functioning scales, 7 of C30 symptom scales, and 8 of STO22 symptom scales showed concordance among the 4 articles. The results demonstrate the reliability or reproducibility of the QOL study. Patients are afraid of changes before and after surgery. By predicting the chronological changes of the QOL profile, patients will be free from fear and find a solution easily to their problem.
In conclusion, robotic and laparoscopic approaches for gastric cancer surgery did not differ regarding QOL, except in the C30 cognitive functioning scale. Male (vs. female), DG (vs. TG), and stage II–III (vs. stage I) resulted in better QOL among the several parameters chosen for the study.

 XML Download
XML Download