

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Cholecystectomy is currently considered the main therapy choice for patients with benign gallbladder disease, although there are no international guidelines on patient selection. This procedure is performed frequently, with more than 800 ,000 cholecystectomies annually in the United States, and associated major global health burden [12].
Development of diagnostic imaging modalities such as CT, MRI, and ultrasonography and their widespread application have led to an increase in diagnosis of benign gallbladder diseases. Although CT is not the first choice imaging modality for suspected gallbladder disease, as ultrasonography is preferred, it is frequently performed in clinical practice because of the short scan time, ease of access, availability, and usefulness for evaluating alternative diagnoses, especially in emergency settings with right upper quadrant pain/discomfort. However, CT has limited ability to detect small stones or polyps in the gallbladder/bile duct and stones that have a similar density to bile. Development of post-processing for CT allows maximal intensity projection, which provides excellent visualization of vascular anatomy to the gallbladder and can provide valuable preoperative information for the surgeon. In cases of biliary obstruction, the multiplanar reformation or minimal intensity projection techniques have demonstrated excellent performance for visualizing the longitudinal extent of bile duct dilatation. However, this modality does not provide sufficient anatomic detail of the bile ducts, particularly non-dilated ducts [34]. In comparison, magnetic resonance cholangiopancreatography (MRCP) is a highly sensitive modality for detecting choledocholithiasis as well as cholelithiasis. Moreover, MRCP can provide both high-quality cross-sectional and projection images of the bile duct and show the anatomy of the intra- and extrahepatic bile ducts even when they are not dilated. Therefore, MRCP may reduce the treatment missing for choledocholithiasis and risk of bile duct injury [567]. This advantage may be associated with the significant increase in preoperative MRCP in patients with planned cholecystectomy. However, the benefits of preoperative MRCP have been controversial. Even though there have been some reports to evaluate the value of MRCP, most of them investigated the predictive value of MRCP to detect asymptomatic choledocholithiasis [6891011]. Only a few studies have been conducted focusing on the influence of preoperative MRCP on the postoperative outcomes in patients who underwent laparoscopic cholecystectomy [810]. Moreover, numbers of enrolled patients in these studies were relatively small.
The purpose of this study was to determine whether preoperative MRCP impacts patient outcomes and management, and which patients should be considered for MRCP preoperatively, those that were scheduled for laparoscopic cholecystectomy for benign gallbladder disease.
METHODS
Study population
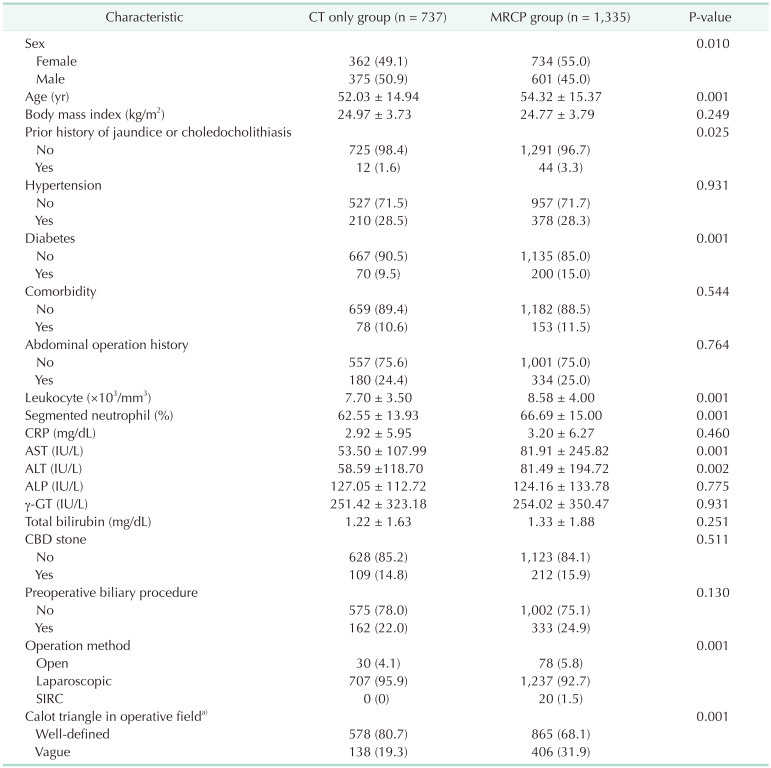
This retrospective study was approved by the Institutional Review Board of Kangbuk Samsung Hospital (KBSMC 2019-10-027-001), and informed consent was waived. From January 2014 to June 2017, data from a total of 2,353 consecutive patients who underwent cholecystectomy for benign gallbladder disease that was coded as a diagnosis of gallstones, gallbladder polyps, cholesterolosis, adenomyomatosis, acute, chronic, or other cholecystitis at our hospital were collected. Of these patients, 281 patients were excluded because (1) other surgery was performed simultaneously (n = 276) or (2) either CT or MRCP was not performed preoperatively (n = 5). A total of 2,072 patients were included in the study. Patients were grouped according to preoperative imaging modalities; CT only group (n = 737) and MRCP group (n = 1,335), which included both CT and MRCP (n = 1,292) or MRCP only (n = 43). Patients were aged 15–99 years (mean age, 53.5 ± 15.3 years) and consisted of 1,096 female patients and 976 male patients. Patient medical records were reviewed for demographic and clinical variables.
Outcomes
The main outcome measure in the 2 groups was complications, including intraoperative or postoperative compl icat ions that occurred within 30 days af ter cholecystectomy. Complications were defined as any adverse events attributable to cholecystectomy based on medical records and imaging findings, if available. Intraoperative bleeding was defined as >100 mL of bleeding. Secondary outcomes were hospital stay for the operation period, readmission within 30 days after cholecystectomy, and events that changed patient management due to addition of MRCP. Events that could change patient management were considered as detecting unexpected common bile duct (CBD) stones not identified by CT; subsequent biliary procedure such as percutaneous transhepatic cholangiography (PTC) or endoscopic retrograde cholangiopancreatography (ERCP), and identifying aberrant bile duct or cystic duct anomalies that could cause bile duct injury. Such bile duct or cystic anomalies were defined as follows: (1) aberrant or accessory intrahepatic bile duct draining into the cystic duct or gallbladder (ducts of Luschka); (2) aberrant drainage of the cystic duct to the right hepatic or left hepatic duct, which can be mistaken for the cystic duct at the point of insertion into either the main hepatic duct or CBD; (3) long (anterior or posterior spiral course, 5 cm or more) cystic duct with medial insertion and parallel course for at least 2 cm [1213], where the duct was surrounded by a common fibrous sheath (if this variation is not recognized, the extrahepatic bile duct can be mistaken for the cystic duct and can result in inadvertent section or ligation of the extrahepatic bile duct and postoperative complication); and (4) absence of or a short/effaced cystic duct (length, <5 mm) due to congenital anomaly, impacted stone, or Mirizzi syndrome, which may result in tenting of the common hepatic duct or CBD and inadvertent clamping of these ducts when attempting to visualize the cystic duct by placing traction on the gallbladder. The MRCP findings mentioned above were retrospectively reviewed by 2 experienced abdominal radiologists (KAK and MSK; 6 and 19 years of experience, respectively) by consensus with blinding to outcomes.
Covariates
Patient characteristics were sex; age; body mass index; prior history of jaundice or choledocholithiasis; hypertension; diabetes; comorbidities [1415]; past history of abdominal surgery; laboratory findings of leukocyte count, segmented neutrophils, CRP, AST, ALT, ALP, γ-GT, and total bilirubin; presence of CBD stone; preoperative biliary procedures including percutaneous transhepatic gallbladder drainage, percutaneous transhepatic biliary drainage, ERCP with stone retrieval, endoscopic sphincterotomy, endoscopic nasobiliary drainage, and endoscopic biliary drainage; surgical method (open vs. laparoscopic vs. single-incision robotic cholecystectomy); and status of Calot triangle in the operative field (well-defined vs. vague). Presence of CBD stones was determined based on ERCP, endoscopic ultrasonography (EUS), or PTC as standards of references. The status was determined based on CT/MRCP with clinical findings if ERCP, EUS, or PTC was not available. Data were collected from patient medical records by 2 radiologists (KAK and MSK).
Statistical analyses
The study sample was divided into 2 groups (CT only group and MRCP group), and the impacts on patient outcomes were assessed. Categorical variables were summarized as number (percentage) of patients, and continuous variables were summarized as mean ± standard deviation. Variables were compared between 2 groups using the chi-square or Fisher exact test (categorical variables) or analysis of covariance (ANCOVA).
Regression was performed to assess independent variables for detecting unexpected choledocholithiasis or changing the patient management by adding MRCP. Backward elimination logistic regression procedures were performed using the variables that were significant in univariate analysis. Statistical analyses were performed using PASW Statistics ver. 18.0 (IBM Corp., Armonk, NY, USA), and a P-value less than 0.05 was considered statistically significant.
RESULTS
Characteristics
Of 2,072 patients, 1,809 (87.3%) had gallstones with or without polyps, and the remaining 263 did not have gallstones; 168 patients with gallbladder polyps (8.1%), 89 cases of cholecystitis (4.3%), and 6 cases of adenomyomatosis (0.3%).
MRCP was preferred in female patients (P = 0.010), older age (P = 0.001), prior history of jaundice or choledocholithiasis (P = 0.025), or diabetes (P = 0.001) compared with the CT only group. The MRCP group showed significantly higher levels of leukocyte count (P = 0.001), segmented neutrophils (P = 0.001), AST (P = 0.001), and ALT (P = 0.002) and had a greater tendency for vague Calot triangle in the operative field (P = 0.001) or conversion to open cholecystectomy (P = 0.001). Patient characteristics between the 2 groups are summarized in Table 1.
Outcomes
Complications
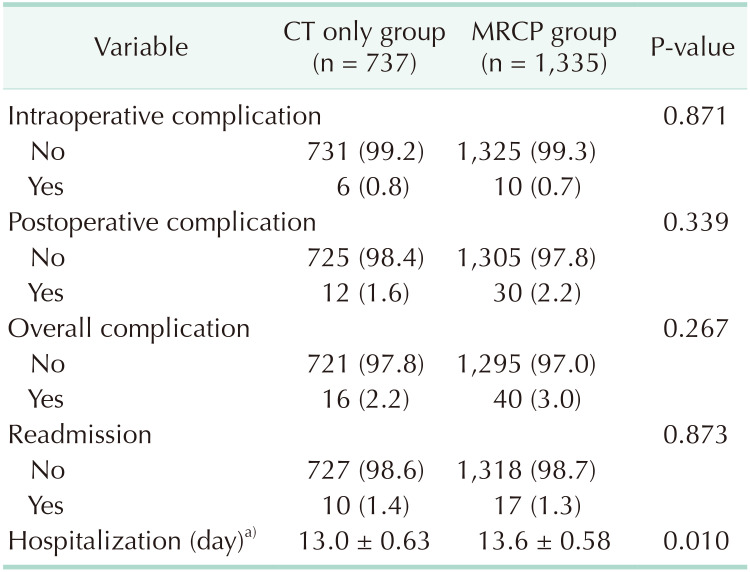
There were no significant differences in rate of intraoperative or postoperative complications between the 2 groups (Table 2). In the MRCP group, there were overall complications in 40 patients. The intraoperative complications (n = 10) comprised bleeding (n = 7) due to adhesion or inflammation, bile duct and duodenal injuries (n = 1) due to adhesion, bile duct injury (n = 1) due to technical error, and small bowel perforation (n = 1) due to severe adhesion during trocar manipulation. The postoperative complications (n = 30) were bile leak in 20 patients, with 1 case of simultaneous duodenal ulcer perforation, remnant cystic duct or CBD stones in 6 cases, fever in 2, intraabdominal abscess due to spilled biliary stone in 1, and active bleeding at the operative bed in 1 case treated with embolization.
Overall complications developed in 16 patients in the CT only group. Intraoperative complications (n = 5) were bleeding (n = 5) due to adhesion or inflammation, with 1 case of duodenal perforation. There were postoperative complications in 12 patients with associated fever (n = 2), bile leak (n = 1), pneumonia (n = 2), bile duct stricture (n = 1), infection at the laparoscopic port (n = 1), remnant stone (n = 2), wound infection (n = 1), pancreatitis (n = 1), and complicated fluid collection at the operative bed (n = 1).
Readmission and hospitalization
There were no significant differences in readmission rates between the 2 groups. The hospital stay was about 0.6 days longer in the MRCP group (Table 2).
Factors associated with detection of unexpected CBD stones or subsequent biliary procedure in relation to addition of MRCP
Addition of MRCP allowed detection of CBD stones that were not initially seen on CT in 84 (6.5%) of the total 1,292 patients that underwent both CT and MRCP. Seventy-four (88.1%) of the 84 patients in whom unexpected CBD stones were detected subsequently underwent biliary procedures. We recommend the subsequent ERCP for stone extraction to all patients diagnosed with CBD stones on MRCP. However, the remaining 10 patients didn't undergo biliary procedure for the following reasons: (1) seven patients had small CBD stones exclusively without features of cholangitis and their spontaneous excretion was expected, therefore, followed by MRCP without intervention; (2) endoscopic cannulation of the bile duct was not possible due to altered anatomy as result of previous surgery (n = 1) or comorbidity (n = 2; schizophrenia and asthma).
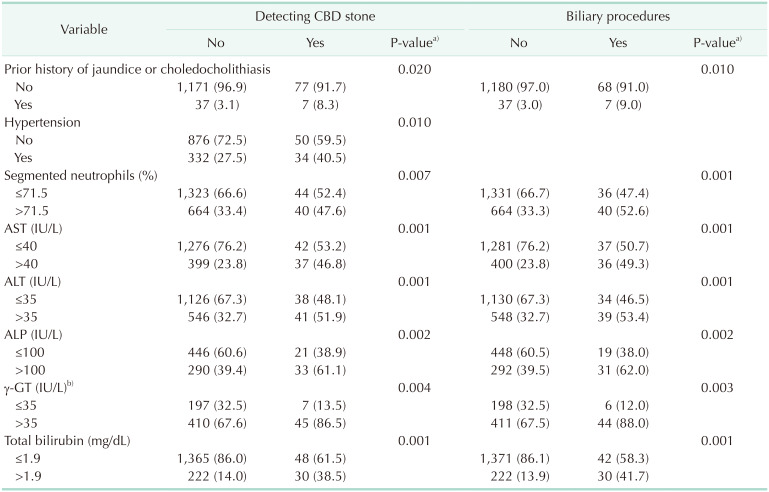
In univariate analysis, prior history of jaundice or choledocholithiasis (P = 0.020), hypertension (P = 0.010), elevated segmented neutrophil count (P = 0.007), AST (P = 0.001), ALT (P = 0.001), ALP (P = 0.002), γ-GT (P = 0.004), and total bilirubin (P = 0.001) were significant factors; elevated γ-GT (adjusted odds ratio [OR], 2.89; 95% confidence interval [CI], 1.12–7.48; P = 0.029) was the only independent factor in detecting unexpected CBD stones in multivariate analysis (Table 3). In univariate analysis for subsequent biliary procedures after addition of MRCP, the significant variables were prior history for jaundice or choledocholithiasis (P = 0.010) and elevated segmented neutrophil count (P = 0.001), AST (P = 0.001), ALT (P = 0.001), ALP (P = 0.002), γ-GT (P = 0.003), and total bilirubin (P = 0.001). Elevated γ-GT (adjusted OR, 3.34; 95% CI, 1.23–9.05; P = 0.018) was the only independent factor in multivariate analysis (Table 3).
Identifying bile duct or cystic duct anomalies that can potentially cause bile duct injury
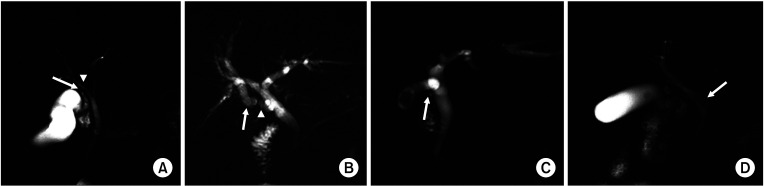
Bile duct anomalies that can cause injury in MRCP were identified in 41 patients (3.2%, Fig. 1): 30 with aberrant drainage of the cystic duct to the right hepatic or left hepatic duct, 4 with aberrant or accessory intrahepatic ducts that drained into the cystic duct or gallbladder, 4 with absent or short cystic ducts (length, <5 mm), and 3 with long (anterior or posterior spiral course) medial insertion and parallel course for at least 2 cm. For 7 patients in the MRCP group, bile duct anatomy could not be evaluated due to poor image quality such as severe motion artifact, severe inflammation, or extensive cysts that occupied the entire abdominal cavity due to polycystic kidney disease and interfered with visualization.
DISCUSSION
Our study showed no statistical difference in patient outcomes between CT only group and MRCP group in benign gallbladder disease (Table 2). However, the MRCP group may have been more susceptible to complications and bile duct injury due to factors such as older age, higher frequency of diabetes, higher levels of the inflammatory markers, AST and ALT, higher rate of conversion, and higher rate of vague Calot triangle in the operative field compared to the CT only group (Table 1). It is well known that various factors such as patient demographics, inherent disease, and surgeon experience contribute to development or possibility of complications after cholecystectomy [16171819]. Based on subanalysis (Supplementary Table 1), other factors of male sex, older age, hypertension, comorbidities, inflammatory markers, and vague Calot triangle in the operation field significantly affected the development of complications, as in prior studies [16171819]. Hence, there is a limit of statistical evaluation to determine if there is difference in clinical outcomes between 2 groups.
With regard to hospitalization, in our study, mean length of hospital stay was longer (13 days) than reported in prior study (1.3–6.3 days) [2021]. The reason for this disparate result could be different characteristics of the study population. Our study included patients with acute cholecystitis that needs to be treated with biliary intervention which may increase the length of stay, whereas previous study included only patients underwent cholecystectomy.
Diagnostic accuracy of MRCP for detecting CBD stones has been clearly demonstrated and is comparable to that of ERCP and intraoperative cholangiography; in addition, the sensitivity and specificity are greater than 90% [222324]. Detection and elimination of CBD stones before operation is important because residual CBD stones can induce postoperative complication such as early biliary leakage, jaundice, cholangitis, and pancreatitis [25]. According to the new guidelines on CBD stone management based on a systematic literature review by the European Society of Gastrointestinal Endoscopy, stone extraction is recommended in all patients with CBD stones, regardless of size or symptoms [25]. It means that additional detection of CBD stones subsequently changes patient management. In our study, silent CBD stones were detected in 6.5% of cases with added MRCP and 88% of our patients with detected CBD stones underwent biliary procedures for stone removal. Detection rate of silent CBD stones in our study (6.5%) was slightly lower than that of previous studies (8%–18%) [2021]. This discrepancy could be attributable to different study cohort. We included benign gallbladder diseases including polyps, adenomyomatosis, and acalculous cholecystitis as well as gallstones, whereas previous studies included patients that underwent cholecystectomy due to symptomatic gallstones.
Since the introduction of laparoscopic cholecystectomy, the change of surgical treatment from open to laparoscopic cholecystectomy has resulted in an increased incidence of iatrogenic bile duct injury, reported at more than 2–6 times the previous rate, and an increase from 0.1%–0.5% up to 3% compared to open cholecystectomy [26]. Any major bile duct injury may result in significant morbidity, increased mortality, and financial burden on the patient [27]. Therefore, prevention of bile duct injury is critical, and it is very important for surgeons to preoperatively understand bile duct anatomy. At the beginning of this study, in our institute, MRCP was performed only when the results of ultrasonography or CT were equivocal for diagnosing choledocholithiasis, or cholangitis was suspected based on the laboratory finding. However, since last 2 years, preoperative MRCP has been performed in most patients undergoing cholecystectomy to prevent bile duct injury as well as to detect silent stones. MRCP can play a major role in identifying potentially risky variants of bile duct anatomy, which were reported at 3.2% in our study.
Routine performance of MRCP prior to laparoscopic cholecystectomy has been controversial due to the associated financial considerations. Prior research has demonstrated that routine use of preoperative MRCP was not cost-effective for diagnosing and managing gallstone disease with asymptomatic choledocholithiasis [28]. However, we believe that MRCP is necessary under specific conditions and can play a significant role in the diagnosis and subsequent treatment of patients, which can have positive effects on patient outcomes. Based on our results, elevated γ-GT was the only independent factor for additional detection of CBD stones (adjusted OR, 2.89; P = 0.029) and subsequently undergoing biliary procedures (adjusted OR, 3.34; P = 0.018) when additional MRCP was performed. In our study, total bilirubin and ALP were significant factors in univariate analysis, but they were eliminated in multivariate analysis.
According to the American Society for Gastrointestinal Endoscopy criteria, derangements of liver function tests other than bilirubin are one of the moderate predictors for assessing the likelihood of choledocholithiasis [29]. However, to the best of our knowledge, none of the studies have been conducted to find clinical predictors for silent CBD stones not identified by CT. Therefore, further comprehensive studies would be needed to identify factors to select candidates who undergo preoperative MRCP in order to detect silent CBD stones.
The strength of our study is the largest comparative study to investigate the impact of preoperative MRCP on the outcomes and management of patients scheduled for laparoscopic cholecystectomy. Nevertheless, there are several limitations of this study. We performed a single-institution, retrospective review, which always presents challenges for data interpretation and can be subject to selection bias. Moreover, different environments for availability or qualification of equipment and presence of a skilled practitioner complicate generalization of our results to other institutions. The enrolled patients in our study had varied entities associated with benign gallbladder disease; therefore, there could also be differences in the rate of complications, readmission, and hospitalization between the group with stones and the group without stones. However, the majority of our enrolled patients (80%) had symptomatic gallstones. Moreover, preoperative MRCP in the non-stone group who are at a higher risk for operation or biliary obstruction such as older age, diabetes, past history of jaundice or choledocholithiasis, or abnormal laboratory markers was not uncommon at our institute, which is the reason we included various disease entities that underwent cholecystectomy. In this study, the detection rate for choledocholithiasis when MRCP was added could be over- or underestimated. A standard reference was difficult to determine because not all cases that additionally detected CBD stones underwent stone extraction. Identification of choledocholithiasis by ERCP can be limited, especially in regard to size and location of stones. In addition, there was a time interval between MRCP and ERCP, which could also have allowed some stone passage. Finally, to assess the significant variation of bile duct anatomy by MRCP, we could not identify all cases of aberrant bile ducts or cystic ducts in the operative fields or using intraoperative cholangiography as the standard of reference.
MRCP is valuable for identification of bile duct variation and CBD stones. Preoperative MRCP can be considered, particularly in patients with elevated γ-GT, for proper preoperative management and avoidance of complications.
 XML Download
XML Download