

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Meckel diverticulum (MD), which is caused by an obliteration defect of the omphalomesenteric duct (vitelline duct or yolk sac), is one of the most common congenital anomalies of the small intestine [1]. It was first described by Johann Friedrich Meckel in 1808 and is also termed omphalomesenteric duct fistula, cyst, or sinus [23]. Although it is found incidentally during abdominal surgery for other pathologies, it can be associated with several complications, including congenital hernia, intestinal bleeding, bowel obstruction due to intussusception or fibrous band, and panperitonitis due to MD perforation [4567].
Conventional surgical treatment of MD has involved exploratory laparotomy with simple diverticulectomy, wedge resection, or small bowel resection and anastomosis [89]. With recent advances in laparoscopic techniques, minimally invasive surgery (MIS) has been applied for the treatment (i.e., resection) of MD in several studies [45671011121314151617181920]. These studies revealed that laparoscopic resection of MD is safe and feasible. However, most of the previous studies were case reports or retrospective, single-institution studies. Furthermore, few studies have compared the outcomes between laparoscopic and open surgery. Therefore, we cannot reach a definitive conclusion that MIS is better than open surgery.
Therefore, the aims of this study were to compare the outcomes between MIS and open surgery for MD and to evaluate the safety and feasibility of MIS procedures. We also compared the clinical outcomes between 2 MIS procedures for treating MD, namely laparoscopic only diverticulectomy (LOD) and laparoscopic-assisted diverticulectomy (LAD).
Go to : 
METHODS
We performed a retrospective, multicenter study of patients who underwent diverticulectomy for MD at 6 Hallym University-affiliated hospitals between January 2008 and December 2017. Due to the retrospective nature of the study, informed consent was waived by the Institutional Review Board of Dongtan Sacred Heart Hospital who approved the study (2019-01-004).
The patients were divided into 2 groups according to whether they underwent open surgery or MIS. MIS included cases of open conversion for patients with severe adhesion and inflammation. Patients who underwent MIS were subdivided into 2 groups according to whether they underwent LOD or LAD. LOD was defined as a procedure in which diverticulectomy was performed entirely intracorporeally. LAD was defined as a procedure involving intracorporeal exploration followed by extracorporeal resection of the diverticulum with extension of the umbilical site. LAD also included the cases of open conversion. The decision of surgery type for MD was based on the surgeon's discretion and the patient's clinical status.
Patient characteristics, operative variables, and postoperative outcomes were retrieved from their medical records. Patient demographic and clinical variables included age, sex, body temperature, body mass index (BMI), WBC count, neutrophil ratio, and serum CRP concentration. Perioperative variables included operation time, presence of small bowel resection or simple diverticulectomy, incidence of incidental Meckel diverticulectomy, and surgical approach (open vs. MIS and open vs. LOD vs. LAD). To consider the surgeons' experience in gastrointestinal (GI) surgery, we divided the surgeons' specialties into 2 groups: GI part (upper and lower GI surgery) vs. others (hepatobiliary, vascular, endocrinological, and pediatric surgery).
Postoperative outcomes included time to flatus, time to soft food intake, length of postoperative hospital stay, the rate of postoperative complications, and postoperative readmission and reoperation rates. Complications were defined as any conditions associated with additional procedures, readmission, reoperation, and prolonged hospitalization.
Laparoscopic techniques
For MIS, patients were placed in the supine position under general anesthesia. The first 10-mm port was placed in the supraumbilical area to insert a camera at 30° using the Hasson open technique. For children, a 5-mm port was used for the umbilical port. Two additional 5-mm ports were placed in the left upper and lower areas. One 5-mm port was enlarged to a 12-mm port for a laparoscopic stapler, such as an Endo-GIA Ultra (Covidien, North Haven, CT, USA), Enchelon Flex Endopath Staplers (Ethicon, Cincinnati, OH, USA), Enchelon Flex Powered Endopath (Ethicon), or iDrive Ultra Powered Stapling System (Medtronic, Minneapolis, MN, USA).
In patients who underwent LOD, after systemic inspection of the peritoneal cavity, MD was resected using a laparoscopic stapler and the specimen was placed in a LapBag (Sejong Medical, Paju, Korea). The bag was retrieved through the umbilical port. For LAD, the supraumbilical incision was extended by about 3–4 cm to exteriorize the MD for simple diverticulectomy or small bowel resection and anastomosis using a hand-sewn method or surgical staples. The bowel was then reinserted to the abdomen and the incisions and ports were closed with interrupted sutures. The type of surgery was selected by the surgeon according to the patient's clinical status.
The primary endpoint of this was to evaluate postoperative recovery, including time to flatus, time to soft food intake, and the length of postoperative hospital stay according to the type of surgery. The secondary endpoints were the rate of postoperative complications and potential risk factors for postoperative complications.
Statistical analysis
The data were analyzed using IBM SPSS Statistics software package, ver. 24.0 (IBM Corp., New York, NY, USA). Continuous variables are presented as the mean and standard deviation and were compared using the Mann-Whitney U-test. Categorical variables are presented as the number and percent of patients and were analyzed using chi-square tests or Fisher exact test. Multivariable logistic regression was performed to identify independent predictors of complications. A P-value of <0.05 was considered statistically significant.
Go to :
RESULTS
Over 10 years between January 2008 and December 2017, 64 patients with MD underwent diverticulectomy, of which 21 (32.8%) underwent open surgery and 43 (67.2%) underwent MIS. Table 1 lists the patients' characteristics according to the type of surgery. The mean age of patients in the open surgery and MIS groups was 28.2 and 30.5 years, respectively (P = 0.338). There were no significant differences in BMI, WBC count, neutrophil ratio, or CRP concentrations between the 2 groups. The most common preoperative symptom was abdominal pain (64.0%) in both groups, followed by bleeding (20.3%), vomiting (7.8%), and umbilical discharge (6.2%). In the open surgery group, the most common preoperative diagnosis was mechanical obstruction (47.6%), followed by MD and panperitonitis. In the MIS group, the most common preoperative diagnosis was MD (41.9%), followed by acute appendicitis, mechanical obstruction, and panperitonitis.
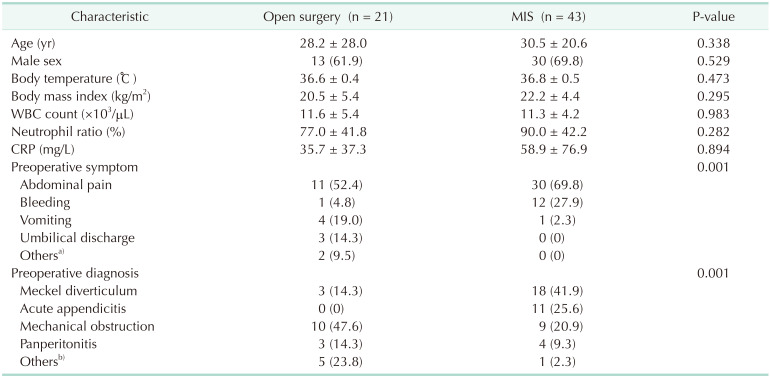
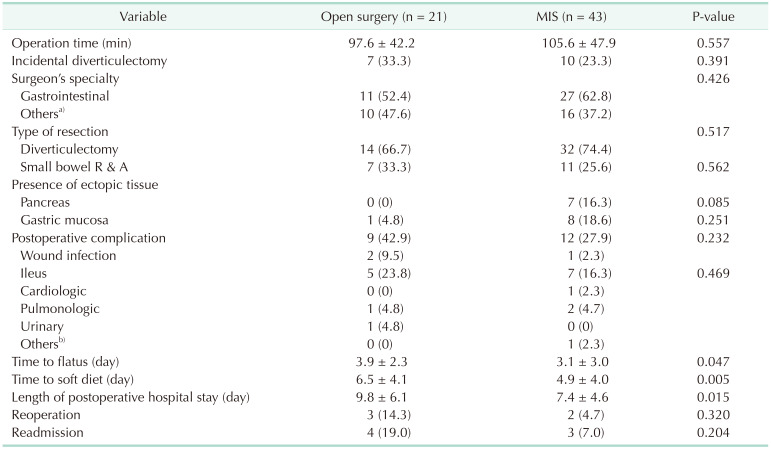
Table 2 presents the perioperative outcomes of open surgery and MIS. The mean operation time in the open surgery and MIS groups was 97.6 and 105.6 minutes, respectively (P = 0.557). The rates of incidental diverticulectomy and type of surgery were similar in both groups. The surgeons' specialties did not differ between the 2 groups (P = 0.426). The time to flatus (3.1 vs. 3.9 days, P = 0.047), time to soft food intake (4.9 vs. 6.5 days, P = 0.005), and length of hospital stay (7.4 vs. 9.8 days, P = 0.015) were significantly shorter in the MIS group than in the open surgery group. The rates of reoperation and readmission were similar in both groups (P = 0.320 and P = 0.204, respectively). Postoperative complications occurred in 9 patients in the open surgery group and in 12 patients in the MIS group, resulting in similar rates in both groups (42.9% vs. 27.9%, P = 0.232). The most common complication was ileus, which occurred in 5 patients (23.8%) in the open surgery group and in 7 patients (16.3%) in the MIS group. Of 5 patients with ileus in the open surgery group, 1 patient was readmitted and underwent reoperation. The other 4 patients were treated conservatively. Of 7 patients with ileus in the MIS group, 2 patients underwent reoperation during initial admission, 1 patient was readmitted, and 4 patients were treated conservatively. Two patients (1 in each group) were readmitted due to surgical site infection and were treated conservatively. In the MIS group, 1 patient were readmitted due to hematochezia and treated conservatively. In the open surgery group, 2 patients were readmitted and underwent reoperation due to a remnant omphalomesentric duct cyst and incisional hernia, respectively.
The MIS group was subdivided into 2 groups (LAD and LOD) and the perioperative outcomes according to the type of surgery are listed in Table 3. In type of surgery, small bowel resection and anastomosis was performed in 11 patients (45.8%) in the LAD group and 7 patients (33.3%) in the open surgery group, and was not performed in the LOD group (P = 0.003). There were no significant differences in the complication, reoperation, and readmission rates among the 3 groups. Among the 3 groups, LOD was associated with shortest recovery times, including the time to flatus (P = 0.011), time to soft food intake (P = 0.002), and the length of hospital stay (P = 0.012) compared with the other groups. When we compared LAD and LOD directly, the time to flatus (3.0 vs. 3.3 days, P = 0.019) and time to soft food intake (4.4 vs. 5.3 days, P = 0.035) were shorter in the LOD group than in the LAD group. The length of postoperative hospital stay was similar between the LOD and LAD groups (6.5 vs. 8.1 days, P = 0.114).
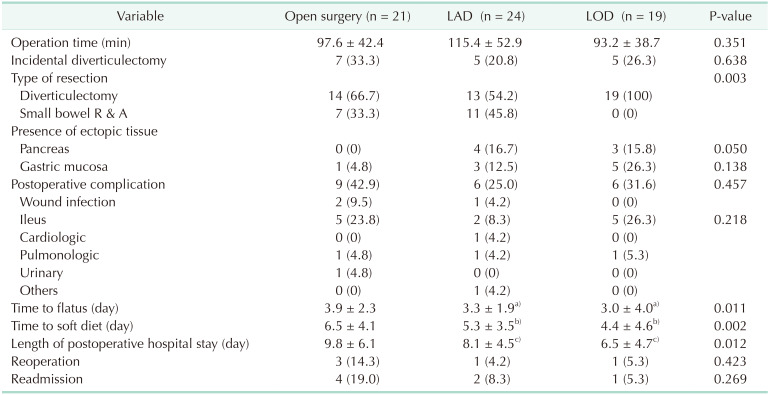
Table 3
Perioperative outcome according to the type of surgery in Meckel diverticulum
Values are presented as mean ± standard deviation or the number of patients (%) unless otherwise stated.
LAD, laparoscopic-assisted diverticulectomy; LOD, laparoscopic only diverticuelctomy; R & A, resection and anastomosis.
a)The time to flatus was shorter in the LOD group than in the LAD group (P = 0.019). b)The time to soft food intake was shorter in the LOD group than in the LAD group (P = 0.035). c)The length of hospital stay was similar between the LOD and LAD groups (P = 0.114).
![]()
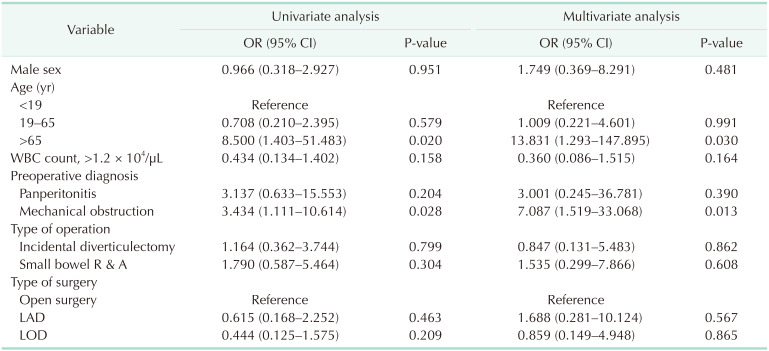
In univariate analysis, old age (>65 years, P = 0.020) and preoperative diagnosis of mechanical obstruction (P = 0.028) were associated with postoperative complications. Multivariable analysis also showed that old age (>65 years, P = 0.030) and preoperative diagnosis of mechanical obstruction (P = 0.013) were independent predictors of postoperative complications. The minimal invasiveness of surgery (open, LOD, and LAD) was not associated with postoperative complications (Table 4).
Go to :
DISCUSSION
MD, which is caused by an obliteration defect of the omphalomesenteric duct, was first described in 1808 by Johann Friedrich Meckel [23]. It is one of the most common congenital anomalies of the intestinal tract, with an incidence ranging from 0.3% to 2.7% [1213].
Correct preoperative diagnosis of MD is challenging because its clinical presentations are not specific [12]. Furthermore, conventional imaging studies, including CT, ultrasonography, and barium series do not have high accuracy [21]. Although CT and ultrasonography are frequently performed as initial imaging studies in patients with abdominal pain, they are limited for detecting MD because they cannot distinguish between distended bowel loop and MD, which is a movable and tubular structure. Moreover, it is difficult to detect MD in patients with intussusception or intestinal obstruction caused by MD [22].
The best noninvasive diagnostic technique for MD involves radionuclide scans and measuring technetium-99m (99mTc)-pertechnetate uptake by the ectopic gastric mucosa. Previous studies revealed that this scan has a sensitivity of 66.6%–87.5% [2324]. However, a false-negative diagnosis may occur in patients with insufficient gastric mucosa to bind 99mTc and in patients who experience a rapid “wash out” effect caused by a fast intestinal transit time [25].
Since Attwood et al. [26] first reported laparoscopic treatment of MD in 1992, several studies have confirmed the possibility of laparoscopic treatment [45671011121314151617181920]. However, most of these studies were case reports or retrospective, single-institution studies. Although several studies used national data or big data, including the National Surgical Quality Improvement Program-Pediatric database, or the Pediatric Health Information System database on MD, these studies did not include valuable information on clinical outcomes, indication for surgery, type of resection, or pathologic results [927].
With recent developments in laparoscopic instruments and accumulating experience of performing laparoscopic surgery, laparoscopy has extended from being a valuable diagnostic tool in patients with unclear clinical findings to an effective therapeutic procedure that can be performed without further delay [13]. Indeed, several studies have reported that patients who underwent laparoscopic surgery have a shorter hospital stay than patients who underwent open surgery [916]. However, these studies did not specifically compare recovery between the 2 approaches [916]. The present study showed that MIS was associated with shorter hospital stay as well as shorter times to flatus and soft food intake.
Laparoscopic diverticulectomy for MD can be performed by intracorporeal or extracorporeal methods. The first technique is performed entirely intracorporeally using 3 laparoscopic trocars. Laparoscopic diverticulectomy has been performed with application of an endo-loop [1926] or laparoscopic staples for simple diverticulectomy or wedge resection [111217181920]. Laparoscopic staples enabled safer and quicker resection of MD without intraperitoneal contamination [121820]. However, one of the major concerns of LOD is the possibility of leaving heterotopic mucosal tissue due to insufficient resection [10]. Echenique et al. [28] reported that stapled excision cannot be technically performed in patients with a very short or broad diverticulum. In addition, although it is possible to perform segmental resection and side-to-side anastomosis of MD intracorporeally, this approach required a longer operation time compared with laparoscopic-assisted surgery even when it performed by skilled laparoscopic surgeons [1016]. Moreover, endo-staplers are expensive.
LAD is also known as a laparoscopic-assisted procedure [1113151617], transumbilical laparoscopic-assisted Meckel diverticulectomy [10] or laparoscopic-assisted transumbilical Meckel diverticulectomy [14]. In LAD, the MD is retrieved through an extended umbilical port. Simple diverticulectomy or small bowel resection and anastomosis of the MD are performed using hand-sewn methods or staplers [101113141517]. This procedure has several advantages. In particular, extracorporeal resection and anastomosis can be performed easily and safely without the risk of intraperitoneal contamination [10]. This technique allows the surgeon to assess the presence of remnant heterotropic mucosa by palpation of MD [14]. This technique does not require expensive laparoscopic staplers [215].
In the present study, small bowel resection and anastomosis were performed in the LAD group but not in the LOD group. This suggests that LAD could be one of options in patients with MD requiring skillful procedures. The subanalyses in this study showed that the recovery time was longer in the LAD group than in the LOD group. However, although there were statistically significant differences in the time to flatus of 0.3 days and soft food intake of 0.9 days, these differences are unlikely to be clinically significant. Meanwhile, there were no differences in the length of hospital stay or the complication rate between LOD and LAD. Accordingly, LAD may combine the advantages of both surgical techniques, namely minimal invasiveness of laparoscopic surgery and direct palpation of conventional surgery.
The postoperative complication rate following diverticulectomy for MD ranged from 8.3% to 18% in prior studies [14272930]. Cullen et al. [30] reported an overall complication rate of 20%, which comprised an early complication rate of 12% and a late complication of 7%. Although the complication rate of 32.8% in the present study seems to be higher than the rate reported in previous studies, the rate of surgery-related complications, such as wound infection and ileus, was 23.4%, similar to the prior study. The most common complication after diverticulectomy for MD is adhesive intestinal obstruction, which ranged from 5% to 7% in prior studies [1429]. Sai Prasad et al. [14] reported that adhesion may be caused by secondary changes in the ischemic bowel after resolution of the obstruction. In the present study, the most common complication after diverticulectomy was adhesive intestinal obstruction, which occurred in 18.7% of patients. Two patients were readmitted and 3 patients underwent reoperation. However, the rate of this complication did not differ between the types of surgery. The multivariable analysis in the present study showed that the type of surgery was not a risk factor for complications, but 2 clinical factors, namely older age and preoperative diagnosis, were risk factors for complications.
There are several limitations to the present study. The main limitation is that this study was performed retrospectively, introducing the possibility of selection bias. Although we analyzed the medical records of patients treated at 6 hospitals, the number of patients may be too small to reach a definitive conclusion. Nevertheless, we included more patients than previous studies [456710111213141517181920]. It must also be highlighted that the low incidence of MD precludes a prospective randomized trial. The present study is also one of few studies to have compared the clinical outcomes among different types of surgery, including open surgery vs. MIS and LAD vs. LOD. We also identified several risk factors for postoperative complications, namely older age and preoperative diagnosis of ileus, but the type of surgery was not a risk factor for postoperative complications.
The present study showed that MIS of MD is associated with quicker recovery without increased risk of postoperative complications. Therefore, MIS may be considered as the surgical procedure of choice for the treatment of MD. We also compared outcomes between 2 laparoscopic techniques (LOD and LAD), and found that LAD may be more effective in cases requiring more skillful procedures, including bowel resection and anastomosis. An old age and preoperative ileus were associated with a risk of postoperative complications.
Go to :
 XML Download
XML Download