

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer (CRC) is the third most common cancer and fourth leading cause of cancer-associated mortality worldwide. The global burden of CRC is expected to increase by 60% to more than 2.2 million new cases and 1.1 million deaths by 2030 [1]. Despite the standardization of surgical procedures (total mesorectal excision and complete mesocolic excision) and the contributory effect of neoadjuvant and adjuvant therapies on survival, recurrence occurs in 30%–50% of CRC cases [2]. There are numerous factors affecting survival in CRC that could be divided into 2 main groups: patient characteristics (performance status, age, and sex) and tumor characteristics (TNM stage, biomarkers, and gene mutations). However, it is well known that the survival time can differ even for patients with the same characteristics and the same disease stage at diagnosis. LDH and albumin are significant markers of systemic inflammation and have been shown to play a key role in promoting cancer progress and metastasis in many cancers including CRC [34567].
The LDH assay is an inexpensive and practical analysis commonly used in clinical practice. LDH, which is a key enzyme in glycolysis, is required for the anaerobic conversion of pyruvate to lactate. LDH levels are regulated by the PI3K/AKT/mTOR pathway, the MYC oncogenic transcription factor, tumor hypoxia, and necrosis [8910]. LDH levels are associated with tumor burden and may reflect tumor growth and invasive potential. Additionally, LDH levels have been shown to act as a significant prognostic marker of major malignancies including CRC and other gastrointestinal tract malignancies [111213141516]. On the other hand, it has been reported that abnormal serum albumin is closely related to the progression of many diseases. Previous studies also indicated that low serum albumin levels are associated with poor prognosis in patients with esophageal, gastric, pancreatic cancers, and CRC [171819]. Increased LDH value and low albumin value are indicators of poor survival. With a high LDH-to-albumin ratio, survival is expected to be poor. Although there is little or no documentation of the LDH-to-albumin ratio in the literature, LDH-to-albumin ratio has been shown to be associated with a poor prognosis in esophageal and hepatocellular cancers [2021].
To our knowledge, there has been no study in the literature investigating the effect on LDH-to-albumin ratio on prognosis in CRC. The aim of this study was to assess the prognostic value of LDH-to-albumin ratio in patients with CRC after curative resection.
METHODS
Study population and ethics statement
The retrospective study included 295 CRC patients that underwent curative resection that was performed by the same surgical team (UA, AB) in the gastrointestinal surgery clinics at Dicle University Medical School Hospital and Elazig City Hospital between January 2013 and June 2019. During the study, 371 patients were operated on. Seventy-six patients (35 with missing pretreatment laboratory data, 4 with hemolysis, 18 without curative resection, 7 with early mortality, and 12 with loss in follow-up) were excluded from the study. The study protocol was approved by Firat University Clinical Research Ethics Committee (No. 97132852/09), and the study was conducted in accordance with the Helsinki Declaration. Written consent was obtained from each patient. Inclusion criteria were as follows: (1) an endoscopic diagnosis of adenocarcinoma established prior to the treatment, (2) a complete laboratory workup including LDH and albumin levels conducted during diagnosis or within the last month, (3) an R0 resection, and (4) complete clinicopathologic characteristics and follow-up data. Exclusion criteria were as follows: (1) a prior history of cancer, (2) any form of acute or chronic inflammatory diseases or infections, (3) any form of systemic diseases, (4) presence of hemolysis, and (5) surgical resection other than R0 resection. Laboratory values of the patients were recorded before taking neoadjuvant chemoradiotherapy or chemotherapy. Chemotherapy and radiotherapy cause tumor lysis and tumor size changes. Since this will cause misleading results in LDH value, laboratory values at the time of diagnosis were recorded. Long-term chemoradiotherapy was given before surgery in patients with locally advanced rectal carcinoma. The treatment decision (surgical or perioperative chemotherapy) in patients with liver metastasis was determined by the multidisciplinary team.
Data collection
The main clinical characteristics including age, sex, tumor location, differentiation, TNM stage, American Society of Anesthesiologists physical status classification, serum levels of LDH, albumin, CEA, and CA 19-9 were retrieved from retrospective medical records. Routine laboratory measurements including counts of WBC, neutrophils, lymphocytes, and platelets were performed before treatment. The LDH level was correlated with AST, ALT, and potassium levels, and was excluded from the study in the presence of hemolysis. Postoperative complications were classified based on the Clavien-Dindo classification [22]. Tumor staging was performed according to the Union for International Cancer Control-American Joint Committee on Cancer (UICC-AJCC) TNM Classification System 7th edition [23].
Follow-up
All the patients were followed up once a month within the first year, once every 6 months within the first 3 years, and once every year thereafter. Recurrence was identified based on radiological or biopsy (as needed) results, or surgical exploration. Disease-free survival (DFS) was defined as the time interval between the date of operation and the time when recurrence was first identified. Overall survival (OS) was defined as the time interval from the date of surgery to the date of death. For patients without any sign of an event, the last follow-up data constituted the terminal record.
Cutoff determination of LAR
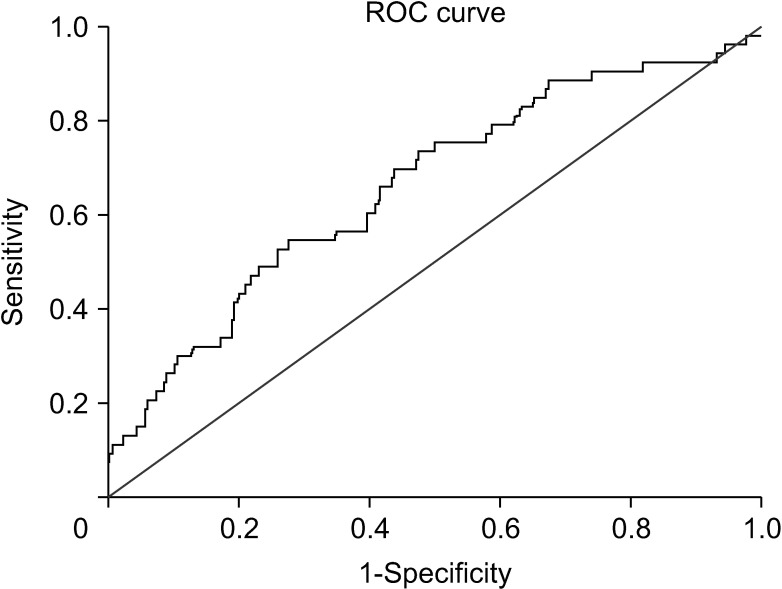
According to the time-dependent receiver operating characteristic (ROC) curve analysis that was conducted for predicting patients that died before the median OS, the optimal cutoff value for pretreatment LDH-to-albumin ratio was 52.7, which resulted in a sensitivity of 69.8% and a specificity of 56.2% (area under the ROC curve, 0.661; P = 0.001) (Fig. 1). Based on this cutoff value, 152 patients (51.5%) had a lower and 143 patients (48.5%) had a higher LDH-to-albumin ratio value before treatment. On the other hand, the cutoff values determined for the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio were 2.73 and 141.8, respectively (P > 0.05 for both).
Statistical analysis
Data were analyzed using IBM SPSS Statistics for Windows ver. 21.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviations or median with ranges. Categorical variables were expressed as frequencies (number) and percentages (%). Continuous variables were compared using independent samples t-test and categorical variables were compared using chi-square test or Fisher exact test. The OS was estimated using the Kaplan-Meier method and the outcomes were compared using the log-rank test. A Cox regression model was used to analyze the independent prognostic risk factors. Significant factors identified in univariate analysis were subsequently enrolled in the multivariate Cox proportional hazard model. A 2-tailed P level of <0.05 was considered significant.
RESULTS
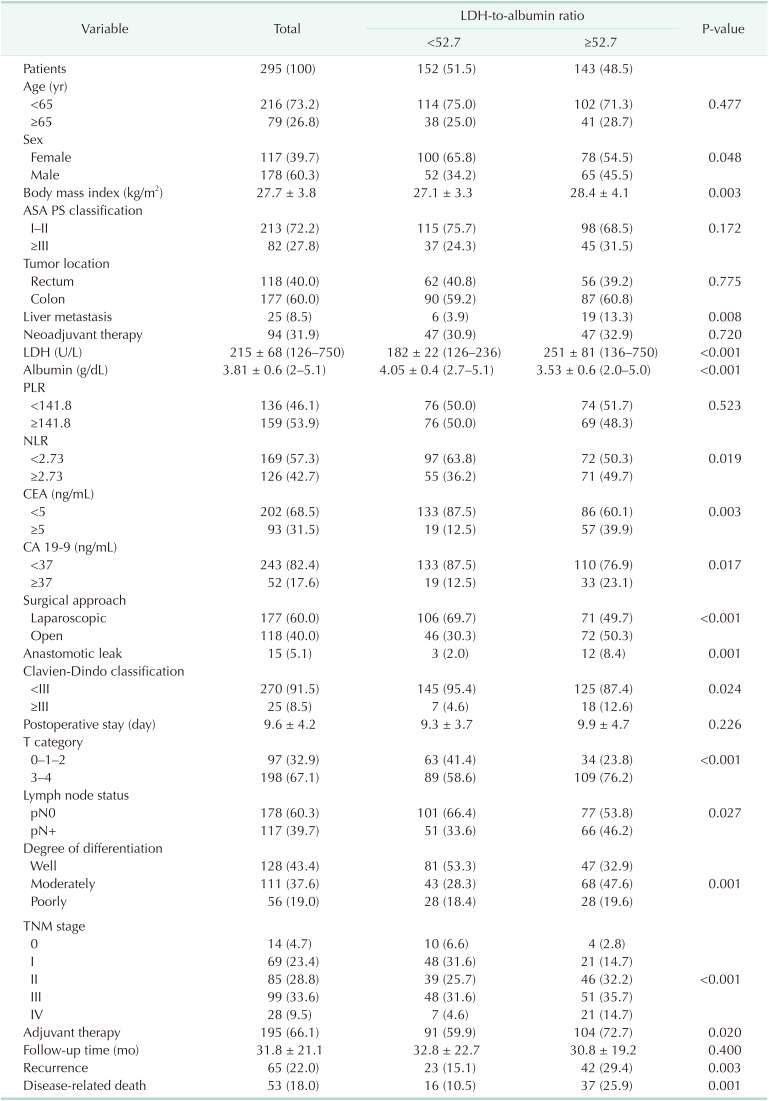
The 295 participants included 117 women (39.7%) and had an overall mean age of 55.8 ± 14.1 years. Baseline characteristics of the cohort were shown in Table 1. The most common tumor localization was colon (n = 177, 60.0%) and resection of synchronous liver metastases was performed in 25 patients (8.5%). Before surgery, 86 patients received chemoradiotherapy (for locally advanced or metastatic rectal cancer), and 8 patients received chemotherapy only for metastatic colon cancer. LDH values in LDH-to-albumin ratio <52.7 and LDH-to-albumin ratio ≥52.7 groups were 182 ± 22 (range, 126–236) and 251 ± 81 (range, 136–750), respectively, and were significant (P < 0.001). The median LDH-to-albumin ratio value of the groups with LDH-to-albumin ratio <52.7 and LDH-to-albumin ratio ≥52.7 were 45.1 (range, 29.3–52.6) and 63.5 (range, 52.7–244.0), respectively, and were statistically significant (P < 0.001). Liver metastasis (P = 0.008), high serum LDH level (P < 0.001), CEA ≥5 ng/mL (P = 0.003), C A 19-9 ≥37 ng/mL (P = 0.017), low albumin level (P < 0.001), anastomotic leakage (P = 0.001), major complications (grade III–IV) (P = 0.024), lymph node positivity (P = 0.027), and advanced tumor stage (P < 0.001) were significantly higher in the group with higher LDH-to-albumin ratio compared to the group with lower LDH-to-albumin ratio (Table 1).
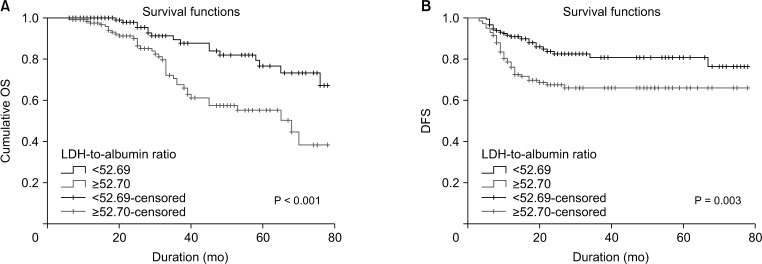
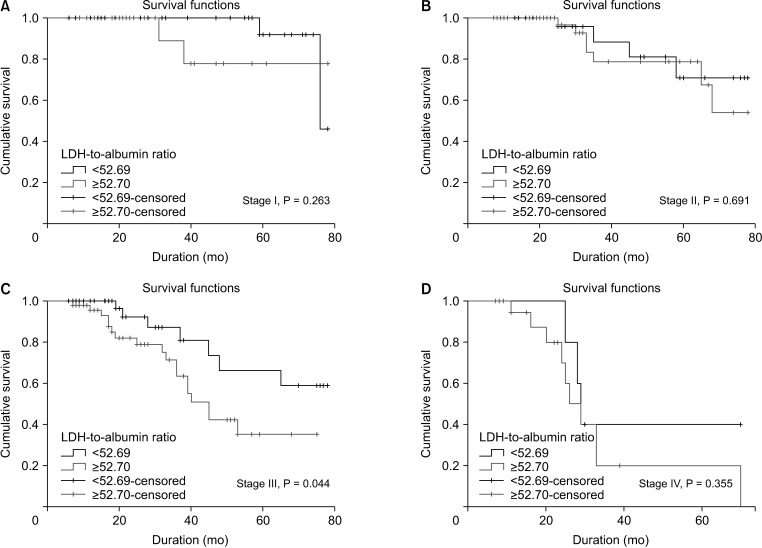
Median follow-up period was 31.8 months (interquartile range, 6–78 months). At the last follow-up, 53 patients (18%) died of cancer-related causes. Five-year OS and DFS rates were 68.5% and 65.4% in the group with lower LDH-to-albumin ratio and were 55.4% and 55.2% in the group with higher LDH-to-albumin ratio. Kaplan-Meier curves showed that LDH-to-albumin ratio ≥52.7 was significantly associated with worse OS and DFS (P < 0.001 and P = 0.003) (Fig. 2). When the effect of stage on survival is examined; survival was worse in stages II, III, and IV, but only stage III was statistically significant (P = 0.044) (Fig. 3).
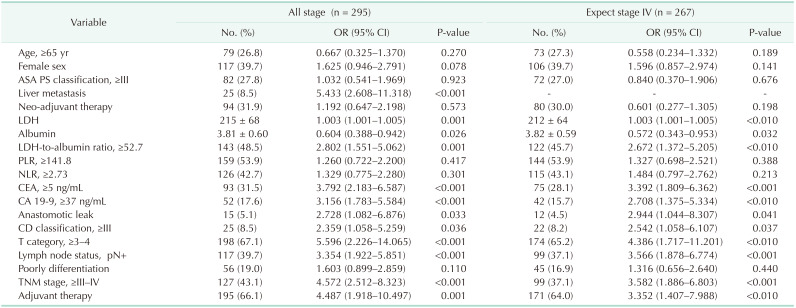
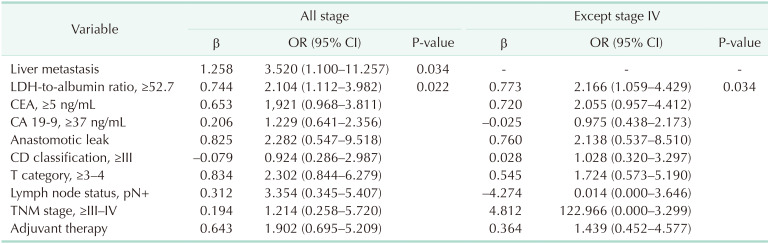
Univariate analysis was performed to determine the prognostic value of LDH-to-albumin ratio and other clinical variables for OS (Table 2). The analysis indicated that the presence of liver metastasis (P < 0.001), LDH-to-albumin ratio ≥52.7 (P = 0.001), CEA ≥5 ng/mL (P < 0.001), C A 19-9 ≥37 ng/mL (P < 0.001), anastomotic leakage (P = 0.033), grade III–IV complications (P = 0.036), pT3–4 (P < 0.001), lymph node positivity (P < 0.001), and TNM stage III–IV (P < 0.001) were associated with OS. On multivariate analysis, however, only LDH-to-albumin ratio ≥52.7 (odds ratio [OR], 2.104; 95% confidence interval [CI], 1.112–3.982; P = 0.022) and liver metastasis (OR, 3.520; 95% CI, 1.100–11.257; P = 0.034) were found to be independent predictors of OS (Table 3).
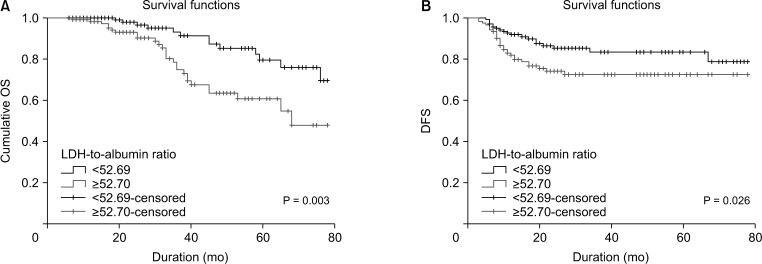
When stage IV patients were excluded, 5-year survival was 70% in the group with LDH-to-albumin ratio <52.7 and 58.9% in the group with LDH-to-albumin ratio ≥52.7 (P = 0.003, Fig. 4). In the univariate and multivariate analyses performed by excluding stage IV, the LDH-to-albumin ratio ≥52.7 was again an independent risk factor associated with poor prognosis (OR, 2.166; 95% CI, 1.059 to –4.429; P = 0.034) (Tables 2, 3).
DISCUSSION
This study investigated the effect of LDH-to-albumin ratio on prognosis in CRC, based on the high LDH and low albumin levels associated with poor prognosis in many cancers. The results indicated that high LDH-to-albumin ratio had an adverse effect on the prognosis in CRC patients undergoing curative resection. To our knowledge, this is the first study in the literature investigating the relationship between LDH-to-albumin ratio and prognosis in CRC patients. The oxidoreductase LDH, which converts pyruvate to lactate when oxygen is absent or in short supply, plays a crucial role in the metabolism of cancer cells. LDH-A is overexpressed in hypoxic carcinomas as well as metastatic cancer cells, and its levels correlate with tumor viability. In numerous tumor types, serum LDH levels are indirect markers of tumor hypoxia, neo-angiogenesis, and poor prognosis [1224]. Additionally, high LDH is closely associated with increased tumor vascular intensity, increased tumor burden, and tumor progression [25]. Serum albumin level is a significant marker of nutritional status. Tumor-related systemic inflammatory response may contribute to the progressive loss of albumin. In addition, hypoalbuminemia significantly influences the length of hospital stay and complication rates, specifically surgical site infection, enterocutaneous fistula, and deep vein thrombosis formation. For this reason, low albumin level may be a valuable prognostic factor for poor survival in CRC patients [11262728].
Studies reporting on the prognostic effect of LDH-to-albumin ratio are highly limited and are relatively recent. Feng at al. [20] evaluated 346 patients with esophageal squamous-cell carcinoma and reported that LDH-to-albumin ratio, TNM stage, and weight loss were effective on survival. The authors determined a cutoff value of 5.5 for LDH-to-albumin ratio and suggested that LDH and albumin alone had no effect on the prognosis of the disease [20]. In another study, Gan et al. [21] found that high LDH-to-albumin ratio was associated with poor prognosis in patients with hepatocellular cancer. The drawback of that study is that both LDH and albumin levels could be affected by the presence of the underlying chronic liver disease regardless of the tumor. In the present study, the cutoff value of albumin level was determined as 52.7 and was expressed as g/dL; however, it would have been determined as 5.27 if it had been expressed as g/L. Determining the LDH-to-albumin ratio level before treatment in patients with CRC may be useful in predicting the prognosis. More aggressive and combined therapies may be recommended to improve prognosis in patients with LDH-to-albumin ratio ≥52.7. Especially in metastatic CRC, high LDH level affects prognosis more negatively. Therefore, the use of chemotherapy protocols with bevacizumab is recommended in patients with high LDH and metastases [2930].
In our study, resection of synchronous liver metastases was performed in 25 patients (8.5%) to achieve an R0 resection. However, recurrence occurred in 72.0% of patients (18 out of 25) within a period of 2 years. On the other hand, both liver metastasis and LDH-to-albumin ratio were found to be independent risk factors for prognosis (OR, 3.520; 95% CI, 1.100–11.257; P = 0.034). Liver metastasis was present in 89.3% of patients (25/28) in stage IV group. The reason for the TNM stage not being statistically significant is that it can be analyzed together with stage III. Namely TNM stage IV (liver metastasis) is an independent predictor associated with poor prognosis, such as LDH-to-albumin ratio. Liver metastasis is the most common site of distant spread and approximately 15%–25% of CRC patients will have distant metastases at the time of primary diagnosis while another 18%–25% patients will develop distant metastases within 5 years from the first diagnosis. Over the last several decades, there has been an increase in surgical resection of liver metastasis, and this procedure has been shown to have a positive contribution to OS. However, it has also been shown that recurrence occurs in 40%–75% of patients after liver resection [313233].
There are several limitations associated with the present study: (1) the study had a relatively small number of patients; (2) the study had a retrospective design; (3) the groups of patients in the study were heterogeneous since the study evaluated patients with colon and rectal cancers in a single study, (4) the results could not be verified by long-term follow-up; and (5) the optimum cutoff value for the preoperative LDH-to-albumin ratio was unknown although 52.7 was set as the cutoff value using the results of an ROC analysis. Despite these limitations, it is the first study to examine the effect of LDH-to-albumin ratio on prognosis in CRC, and we believe it is important.
In conclusion, high LDH-to-albumin ratio is an independent risk factor for OS in CRC patients undergoing curative resection. Although further prospective studies with large patient series and longer follow-up periods are needed to substantiate the effect of LDH-to-albumin ratio on the prognosis of CRC, we consider that LDH-to-albumin ratio is a practical and inexpensive marker that can be used in predicting the prognosis of many cancers.
 XML Download
XML Download