

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Healthcare-associated infection (HAI) refers to infections acquired in medical institutions that occurred 48 hours after the first admission, 3 days after discharge, and 30 days after invasive procedures such as surgery [1]. As healthcare services become easier to access and the number of patients undergoing invasive procedures increases, the risk of HAIs also increases. Furthermore, this risk might lead to medical accidents and disputes. Medical disputes, including lawsuits claiming compensation for damage and alleging medical malpractice, have been steadily increasing [2]. Approximately 7.6% of cases filed in the Korea Medical Dispute Mediation and Arbitration Agency were related to infection in 2018 [3], and 4.9% of medical service cases filed in the Korea Consumer Agency involved infections [4].
One of the many infections that can occur in hospitals is necrotizing fasciitis (NF), a destructive bacterial infection characterized by necrosis of fascia and subcutaneous tissues. Because NF is usually accompanied by severe systemic toxicity, it is described as a “flesh-eating disease” [56]. Though the incidence of NF is not high, mortality has been reported to range from 7% to 76%; this might be influenced by the patient's medical history and timing of diagnosis [78]. One research suggested that there were 18.1% NF inpatients with HAI [9]. Early diagnosis and rapid treatment can help prevent and reduce poor prognosis [10]; nevertheless, the diagnosis of NF is very difficult [11]. The initial signs and symptoms are often nonspecific until the patient rapidly deteriorates, and NF is commonly accompanied by shock and decreased level of consciousness [12].
If NF occurs, it progresses rapidly, resulting in hypoxic brain damage and even death. Therefore, NF is considered a risk for medical disputes. With respect to HAIs, few studies have analyzed medical lawsuits related to NF [1314].
Therefore, this study aimed to analyze medical litigation to provide baseline data on the general characteristics of medical accidents involving NF, features of NF, and the typical opinions of courts regarding medical malpractice in Korea.
Go to : 
METHODS
The protocol of this study was approved by the Institutional Review Board of Yonsei University. As this study used judgments for analysis without personally identifiable information, the need for informed consent was waived (No. 7001988-201910-HR-717-01E).
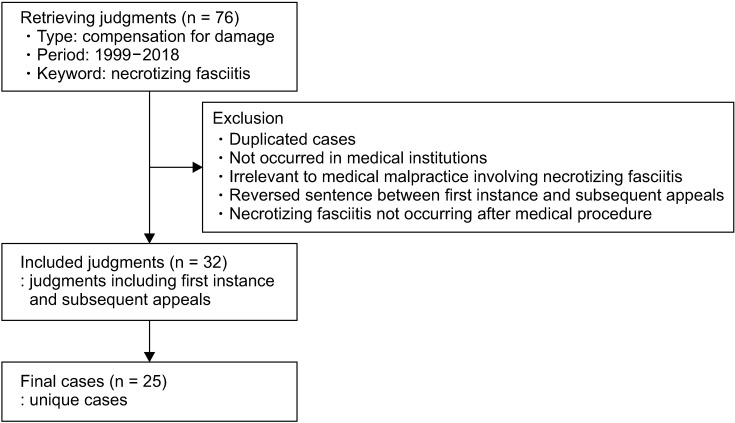
We examined 25 cases of medical civil litigation involving NF during the last 21 years. We performed a search of the Supreme Court of Korea's written judgment management system database of lawsuits closed between January 1998 and December 2018. The following keywords were used for the searches: “NF” and “compensation for damage related to medical malpractice.” First, 76 judgments were retrieved, and rulings were excluded if they (1) overlapped, (2) described a medical accident that did not occur in a medical institution, (3) dealt with medical malpractice involving the occurrence of NF that was not a key factor contributing to the lawsuits, (4) had the decision of the first instance and subsequent appeals reversed, or (5) described a medical accident in which NF did not occur after a medical procedure. Finally, a total of 25 unique cases were selected, and each official copy of the 32 judgments, including the first instance and subsequent appeals, were acquired electronically after personal information was removed for the protection of privacy from the courts (Fig. 1).
Subsequently, the researchers categorized the cases into 3 groups based on medical accident, the occurrence of NF, and breach of duty. For medical accidents, we analyzed the following variables that have been used in previous studies [1516171819202122]: the yearly distribution of NF cases, the period of the resolution, type of medical institution, specialized department, patient's sex and age, and the rate of loss of labor capacity as a result of damage. The decision, limitation of liability, and the amount claimed and awarded relating to the medical accident were analyzed. Second, with respect to the occurrence of NF, the diagnosis, procedure before the occurrence of NF, site of the occurrence of NF, and complications according to NF were analyzed. Finally, with regards to a breach of duty, the plaintiff's claims and opinion of the court regarding the duty of care were analyzed.
IBM SPSS Statistics ver. 25.0 (IBM Corp., Armonk, NY, USA) was used for descriptive statistical analysis.
Go to :
RESULTS
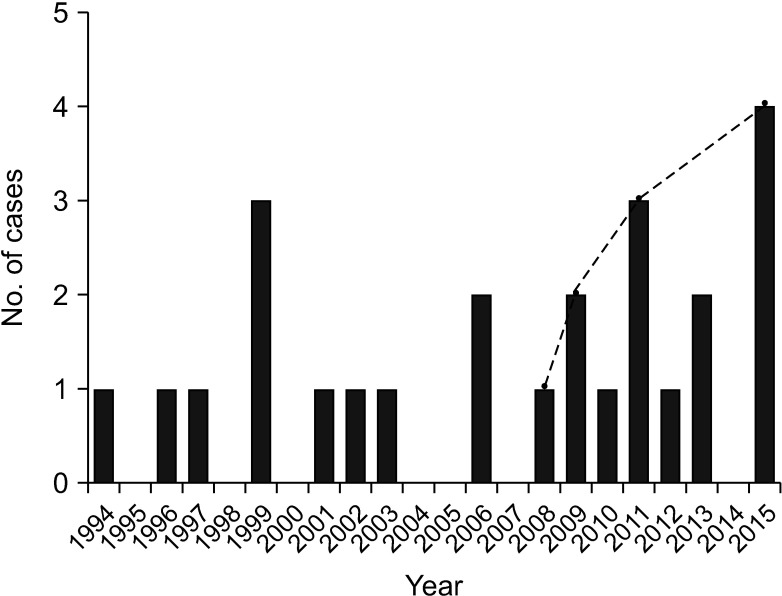
In this study, 25 judgments related to NF were examined. As shown in Fig. 2, the number of claims involving NF has been increasing consistently since 2008.
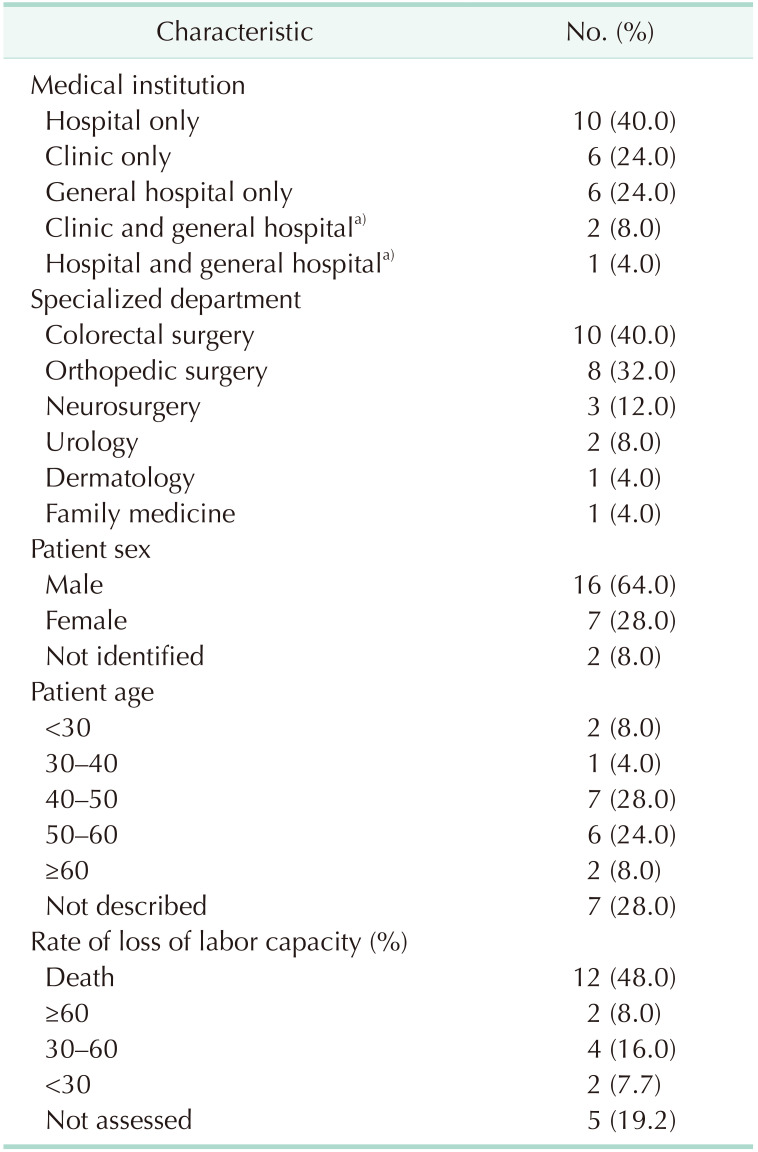
There was an average duration of 3.7 years (range, 1.8–8.3 years) between the occurrence of the patient harm and the date of the decision. The average amount claimed for damage was 249,194,456 ± 210,280,036 Korean won (KRW) (206,714 US dollar [USD]), and the average amount awarded was 70,877,607 ± 98,194,153 KRW (58,975 USD). The medical accidents most frequently occurred in hospital-level medical institutions (10 cases, 40.0%). The department of colorectal surgery was involved most frequently (10 cases, 40.0%). Of the 25 litigation cases, NF involving medical accidents occurred more often to male patients (64.0%). There were 7 (28.0%) and 6 (24.0%) cases involving patients aged 40–50 and 50–60 years, respectively. Because of the medical accidents, the patient died in 48.0% of the cases or lost 30%–60% of labor capacity in 16.0% of the cases (Table 1).
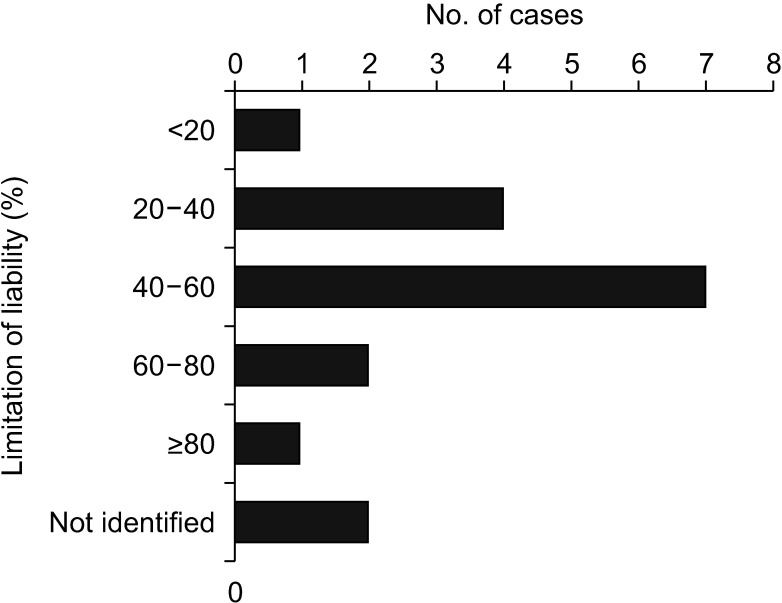
Except for 8 dismissal cases and 2 settlement cases, 15 cases (60.0%) were decided as partially awarded to the plaintiff. In these cases, a liability ratio of the defendants of 40%–60% was the most frequent (41.2%) (Fig. 3).
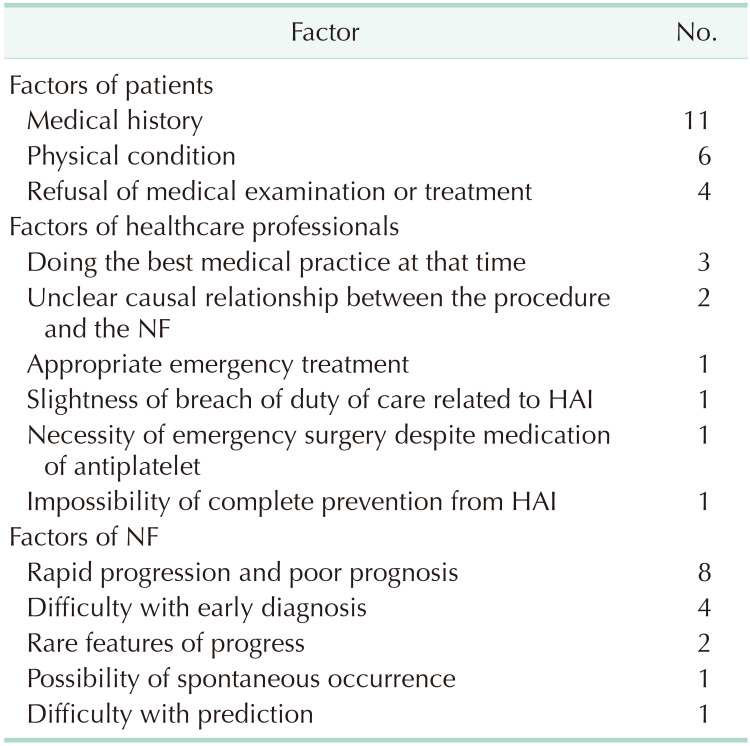
The liability of the defendant was limited for various reasons that can be categorized by 3 factors: patient, healthcare professional, and NF. With respect to the patient, medical history was the most frequent limitation (11 cases). In 3 cases, the liability of the defendant was limited because the best medical practice was performed at that time by the healthcare professionals. With respect to NF, characteristics such as rapid progression and poor prognosis were frequent reasons for the limitation of liability (8 cases) (Table 2).
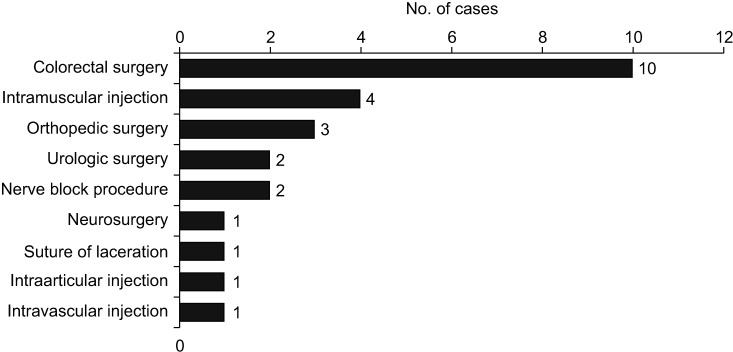
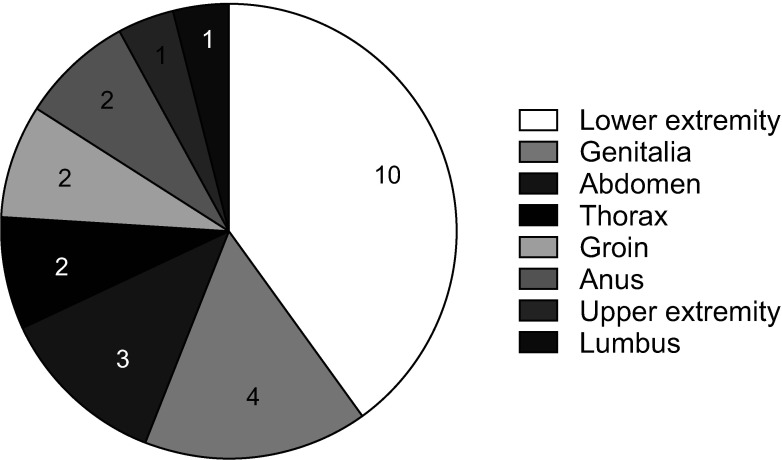
An analysis of the procedure before the diagnosis of NF revealed that there were 10 cases (40.0%) involving colorectal surgery, followed by 4 (16.0%) and 3 cases (12.0%) related to intramuscular injection and orthopedic surgery, respectively (Fig. 4). In the 25 limitation cases, NF occurred in the lower extremities in 10 cases (40.0%), the genitalia in 4 cases (16.0%), and the abdomen in 3 cases (12.0%) (Fig. 5).
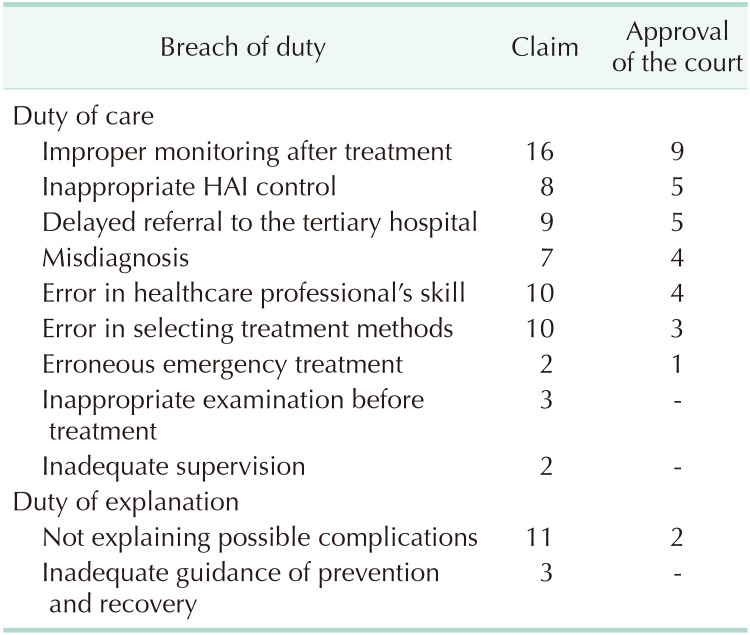
Because the plaintiff claimed different breaches of duty that were imposed on the defendant in each case, improper monitoring after treatment was the most common breach of duty claimed in the 25 cases. Aside from the claims, improper monitoring after treatment was the most frequently identified violation of duty (9 cases), followed by inappropriate HAI control (5 cases) and delayed referral to the tertiary hospital (5 cases) (Table 3).
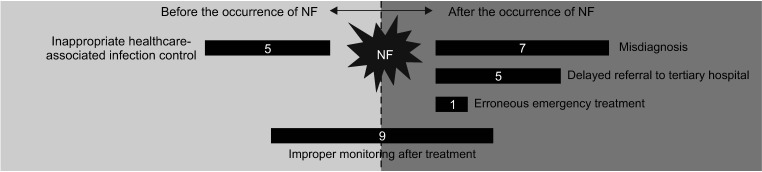
In 17 cases awarded partially to the plaintiff, the courts recognized improper monitoring (9 cases) most frequently, regardless of the time of occurrence of NF. However, the duty of care after the occurrence of NF, such as misdiagnosis (7 cases) and delayed referral to the tertiary hospital (5 cases), were emphasized by the court as opposed to those before the occurrence of NF (Fig. 6).
The following 3 cases were selected as examples where the court agreed there was a breach of the specific duty of care. For each case, we provide a summary, breach of duty, and the reason for the limitation of liability.
Case 1
A 47-year-old man who was diagnosed with chronic diabetes mellitus visited a general surgery clinic for pain and swelling around the anus. He was diagnosed with an anal fistula with perianal abscess and was treated with drainage. After discharge, the patient experienced vomiting, abdominal pain, and dyspnea. He was referred to the tertiary hospital with suspicion of sepsis and diabetic ketoacidosis. Emergency fasciotomy and multiple debridements were performed after the diagnosis of NF. However, the patient eventually died due to sepsis and an embolism. The patient's family filed a lawsuit in 2015 for a violation of the duty of care and explanation. The court agreed that there were inappropriate blood sugar checks before the surgery, improper antibiotic treatment after the surgery, and delayed referral to a tertiary hospital. The liability of the defendant, however, was limited to 30% because of the patient's medical history, difficulty with the prediction of NF, and the indefiniteness of a causal relationship between anal drainage and occurrence of NF.
Case 2
A 49-year-old woman who was on antiplatelet medications because of thrombosis visited a general hospital for abdominal pain. She was diagnosed with acute appendicitis and underwent an appendectomy. After the operation, a sanguineous discharge was observed, and she complained of chills, fever, and pain at the surgical site. On the 9th day after surgery, she became lethargic and was referred to the tertiary hospital immediately. She died that day because of septic shock due to NF. Her family sued in 2012 for a breach of duty of care. The court recognized the misdiagnosis of NF. The liability of the defendant, however, was limited to 40% because of the patient's medical history, the necessity of early operation despite the risk of bleeding, and having received the best medical care possible.
Case 3
A 53-year-old woman visited a hospital for swelling of the knee joint. She was treated by arthresis and physiotherapy for 4 years. One day, pyogenic arthritis was suspected after arthresis of the left knee. She was referred to a tertiary hospital and was subsequently diagnosed with left femoral NF, left gonitis purulenta, and left femoral abscess. After being treated with several irrigations and debridements, the range of motion of her knee and femur remained limited. The plaintiff filed a lawsuit in 2016, claiming a violation of the duty of care. The court agreed that there was improper monitoring related to infection after arthresis and surgery and that invasive procedures should not have been performed after the suspicion of infection. The liability of the defendant, however, was limited to 50% because of the patient's medical history, such as swelling of the knee joint and the possibility of spontaneous occurrence of NF.
Go to :
DISCUSSION
In this study, we analyzed 25 litigation cases related to NF in the past 21 years in Korea. The number of medical lawsuits related to NF has been increasing since 2008 [2].
The limitation of liability is a basic principle in which, after a fair share of damages, the defendant compensates the victim to reduce damages caused by malpractice after taking various factors into account [18]. This is usually expressed as a percentage of the defendant's liability. Furthermore, most lawsuits were filed against departments of surgery (40%) [16], as also shown in this study. There can be several reasons for the limitation of liability, categorized according to the following factors: patients, healthcare professionals, and the features of diseases. First, the most common reason was the patient's medical history. If the patient had a medical history that could confer a risk of infection, such as diabetes mellitus, the compensation may be reduced because it could be assumed that there was no breach of duty and that the patient influenced the damages. Second, despite recognizing a breach of the duty, the liabilities of the physicians can be reduced because of the characteristics of medical practice. Because healthcare professionals do not practice to harm patients on purpose, and although they do their best job, bad results can occur because of bad luck. Finally, the most commonly cited factors of NF that limit the physicians' liability was the rapid progression and poor prognosis of NF. Even when the court recognized the malfeasance, it considered that NF was hard to cure.
The results of this study showed that colorectal surgery was the most relevant procedure before the diagnosis of NF. Colorectal surgery is also the most frequent type of surgery in medical lawsuits relating to general surgery [16]. Additionally, the most common sites of NF have been reported to be the upper and lower extremities, trunk, and head or neck [2324]. The sites of NF reported in litigation cases were similar: the lower extremity, the genitalia, and the abdomen. Particularly, in the genitalia, Fournier gangrene is a type of NF characterized by a rare, serious, and progressive infection [25].
The court frequently agreed that improper monitoring after treatment was related to the NF. With respect to the time of occurrence of NF, the duty of care after the occurrence of NF was highlighted by the court than that before the occurrence of NF. Judgments that reflected the characteristics of NF occurred frequently. These findings suggest that healthcare professionals should focus on early diagnosis and progressive treatment of NF. Furthermore, physicians in the clinic- and hospital-level institutions should transfer patients to tertiary hospitals when abnormal signs and symptoms appeared.
Learning from medical accidents is important in risk management to prevent the occurrence of similar cases and improve the quality of healthcare services [2627]. An individual physician cannot completely prevent severe infections such as NF. The institution should provide support to reduce the incidence of HAI. These litigation cases suggest that physicians cannot be blamed when NF occurs. Nevertheless, surgeons, especially in the department of colorectal surgery, should pay attention to changes in a patient's status after surgery. The timely recognition and management of NF might be considered as one of the main factors for deciding malpractice in court. Likewise, through an analysis of adverse events such as medical litigation, human and systemic factors might improve in the healthcare system [27].
This study has several limitations. First, the details of the medical processes were not accurately assessed due to the characteristics of judgments, which described only the details required for the decision. Nevertheless, we reviewed some previous studies regarding medical malpractice and judicial precedents [15161718192021282930] and tried to set appropriate variables for quantitative analysis and structure for qualitative analysis. Second, there were only a few litigation cases related to NF, meaning a longer period was needed to retrieve cases; therefore, judgments in the past might not reflect the current clinical practice.
In conclusion, 25 medical malpractice cases involving NF were reported in this study. Despite some limitations, we highlighted the medicolegal implications from medical lawsuits involving NF. This study provides physicians with information for preventing medical accidents and disputes involving NF via an analysis of medical accidents, features of NF, and the opinions of the courts. To avoid medical lawsuits, physicians should make an early diagnosis and treatment based on the monitoring of high-risk patients who undergo invasive procedures. A deficiency in the diagnosis and treatment of NF can increase the probability of medical disputes.
Go to :
 XML Download
XML Download