

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Curative resection remains the optimal treatment for hepatocellular carcinoma (HCC), although ablation and liver transplant are indicated for early staged disease [12]. However, the prognosis of HCC after curative hepatic resection (HR) is dismal. Typically, the long-term outcome of cancer after curative surgery is determined mostly by tumor characteristics, e.g., size, number, location, vascular invasion, etc. as well as surgical procedures, e.g., margin, ischemia/reperfusion injury, resection type, blood loss, and transfusion, etc. [34]. Few studies have discussed possible impacts of judgment bias and inaccurate performance of surgeons secondary to progressive fatigue on patient outcomes [5].
Long work hours are considered a tradition among surgeons [67]. Undoubtedly, human performance is adversely affected by sleep deficit, circadian rhythm disruption, and long work hours, leading to decrements in cognitive and psychomotor performance and increased risk of accidents [8]. Prolonged duty hours and sleep deprivation have been associated with increased medical errors among interns [910111213]. For example, even during work days, adenoma detection rate was significantly higher in morning colonoscopies than in afternoon colonoscopies [141516]. Patients anesthetized at different time of the day may have different clinical outcomes [17].
However, some other studies found that sleep deprivation before surgery, or surgery start times during working hours did not measurably affect the short-term outcomes of the patients [18192021].
As a complex and high-risk procedure, HR is susceptible to the surgeon's mood, cognitive performance, and psychomotor function. Progressive fatigue caused by sustained work may impair the attention, judgment, and performance accuracy of surgeons, which would lead to adverse clinical outcomes [22]. No study has investigated the potential influence of surgery start times on long-term outcome of patients undergoing HR for HCC. The objective of the current study aimed to examine the effects of surgery start time on oncologic outcomes of HCC after curative HR.
METHODS
Study cohort
Patients undergoing HR with curative-intent for HCC between January 2012 and September 2015 in our university hospital were included. Patients undergoing palliative surgery (R2), radiofrequency, laparoscopic, or emergency surgery were excluded from the current study. Patients who died within 90 days after surgery were also excluded. The study was approved by the ethics committee of the First Affiliated Hospital, Xi'an Jiaotong University (No. XJTU1AF2017LSL-007) on the premise of obtaining the voluntary informed consent of enrolled patients, the rules of which comply with the Treaty of Helsinki. A waiver of informed consent was obtained, since the data were analyzed from the electronic medical records and reported without personal identifiers.
Data collection
The clinicopathological data of patients were identified from a prospectively maintained database, including age, gender, body mass index, HBV or HCV status, comorbidities, and preoperative biochemical tests. Tumor size, number and location, and surgical margin were collected from the pathological reports. Surgical procedures, duration, and intraoperative blood loss and transfusion were recorded based on operation and anesthesia reports. Tumor stage was categorized according to the 8th edition of the American Joint Committee on Cancer [23] and Barcelona Clinic Liver Cancer (BCLC) [24] stages.
Diagnosis, surgical procedure, and follow-up
Diagnosis of HCC was established by characteristic features on CT, MRI or hepatic arteriography, and/or a serum α-FP level greater than 400 ng/mL. HR was offered by assessment of resectability based on tumor size, number, and liver functional reserve. Liver function status was assessed by liver biochemistry status, indocyanine green retention test for 15 minutes, and Child-Pugh classification.
All the resection procedures were performed by senior surgeons with at least 10-year experience in liver surgery. All HR on work days started between 8 AM to 6 PM. The beginning of the surgery was defined as start of skin incision. As such, patients were classified as morning surgery (started between 8 AM and 1 PM, group M) and afternoon (started after 1 PM, group A) surgery groups. One PM was generally the time when most surgeons transitioned from the previous to the current major cases, and thus allowed for comparisons of fatigue, focus, mental concentration between morning and afternoon surgeries. All the surgeries were allocated to a scheduled time the day before operation by the surgery department.
The type and extent of HR were defined according to the Brisbane 2000 Terminology of Liver Anatomy & Resections [25]. Major HR was defined as resection of 3 or more liver segments, while minor resection was defined as removal of 2 or fewer segments. Hepatic inflow occlusion was performed when deemed indicated by the operating surgeon in order to reduce intraoperative blood loss. Intermittent hepatic inflow occlusion using cycles of 15-minute ischemia followed by 10 minutes of reperfusion was the preferred regimen. All the procedures were mainly accomplished by senior surgeons with surgical experience of more than 10 years.
All the patients were routinely followed in the Outpatient Department or by telephone interview. Patients were regularly followed after surgery with α-FP, and abdominal CT or MRI scanning. Overall survival (OS) was calculated from the date of surgery.
Statistical analysis
Continuous variables are expressed as median and interquartile range (IQR) and compared with Student t-test or the Mann-Whitney U-test. Categorical variables are expressed as numbers and percentages, and compared with the chi-square test or Fisher exact test. OS was estimated by the Kaplan-Meier method and the log rank test was used to compare differences between different groups. A P-value of <0.05 was considered statistically significant. Statistical analysis was carried out using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
Patient characteristics
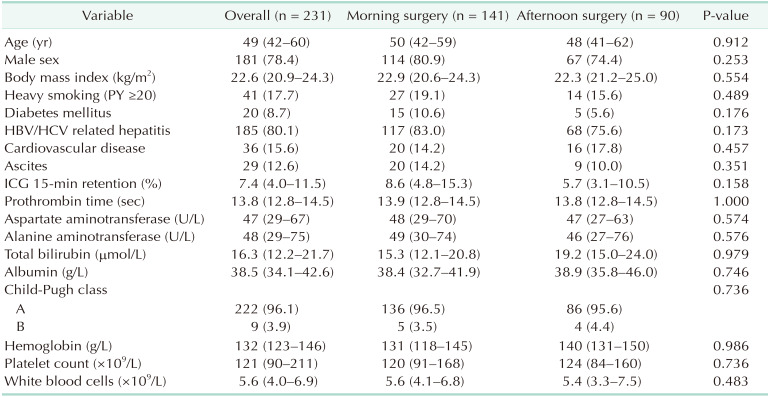
In total, 231 patients were included in the study. Among them, 141 patients underwent morning surgery (8 AM–1 PM, group M), while 90 patients underwent afternoon surgery (1 PM–6 PM, group A). The clinical data of the patients were summarized in Table 1. The median age was 49 years (IQR, 42–60 years). The majority of patients were male (n = 181, 78.4%), and HBV or HCV positive (n = 185, 80.1%). Liver function of Child-Pugh class A was found in 96.1% of patients.
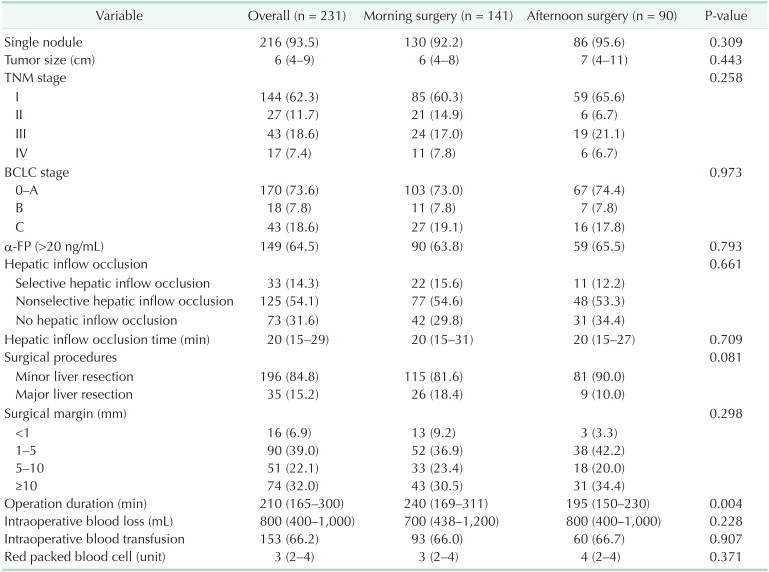
The tumor and surgery associated information was summarized in Table 2. Most patients had a single tumor (n = 216, 93.5%). The median tumor size was 6 cm (IQR, 4–9 cm). Hepatic inflow (selective or nonselective) was a routine procedure performed in about 2/3 of patients during surgery (n = 158, 68.4%). The duration of hepatic inflow occlusion was about 20 minutes (IQR, 15–29 minutes). The median operation time was 210 minutes (IQR, 165–300 minutes). Based on the final pathology report, 74 patients (32.0%) had a wide surgical margin (≥10 mm), 141 patients (61.1%) had a narrow surgical margin (1–10 mm), while 16 patients (6.9%) had microscopically positive margin (<1 mm).
Baseline characteristics: morning vs. afternoon surgery
Patients subjected to afternoon surgery were not different from patients undergoing morning surgery in demographic characteristics, comorbidities, preoperative liver function, tumor size, and number, as well as the TNM and BCLC stages (Tables 1, 2). Interestingly, patients who underwent morning surgery were more likely to experience major resection (morning 18.4% vs. afternoon 10.0%, P = 0.081) and thus longer surgery time (median, morning 240 minutes vs. afternoon 195 minutes, P = 0.004). However, the final surgical margin status, intraoperative blood loss, and blood transfusion were not different between morning and afternoon surgery groups (all P > 0.05).
Overall survival: morning vs. afternoon surgery
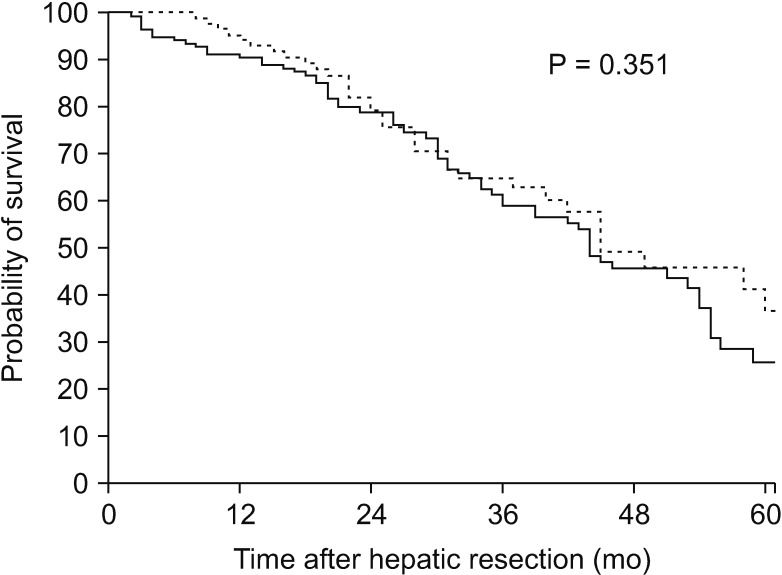
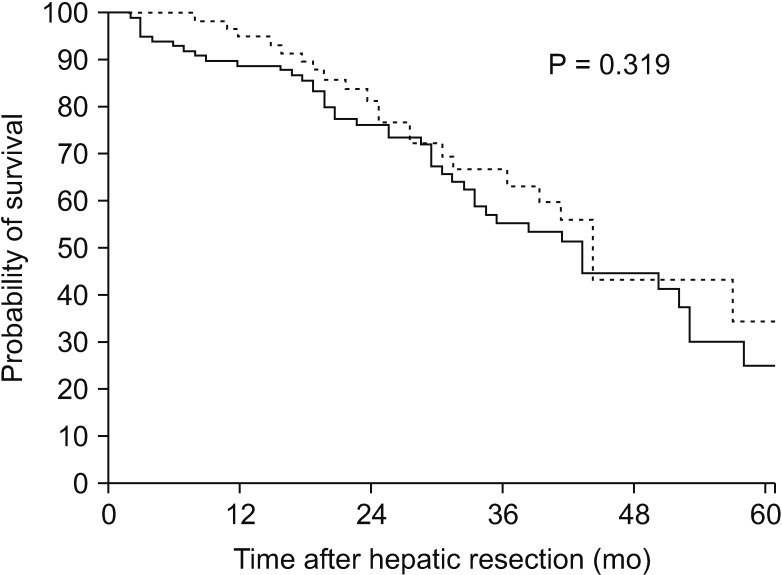
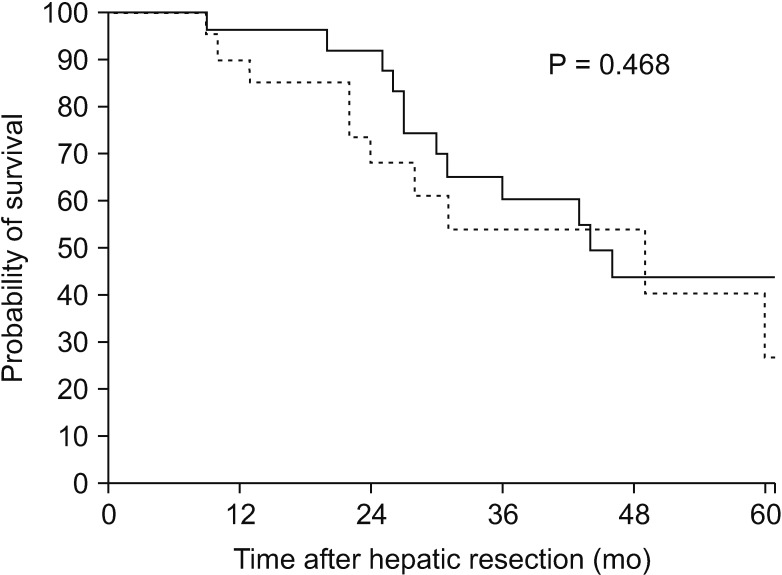
The median, 1-, 3-, and 5-year OS were 45 months, 91%, 78%, and 26% for patients undergoing morning surgery, and 48 months, 93%, 88% and 37% for patients undergoing afternoon surgery (P = 0.351) (Fig. 1), respectively. A further subanalysis was performed depending on the surgical margin and surgery start times. Consistently, patients undergoing morning surgery had equivalent OS versus those undergoing afternoon surgery either in narrow surgical margin group (1–10 mm, median OS, morning surgery 43 months vs. afternoon surgery 44 months, P = 0.319) (Fig. 2) or wide surgical margin group (≥10 mm, median OS, morning surgery 44 months vs. afternoon surgery 52 months, P = 0.468) (Fig. 3).
DISCUSSION
Overload of work and subsequent progressive fatigue of physicians may lead to increased medical errors or accidents among interns or junior physicians [8910111213]. The reason for decreased efficiency of medical performance may include: (1) Afternoon fatigue. Evidence suggests that fatigue impairs human performance and many physicians work from early in the morning to late in the day. (2) Afternoon circadian lows. The natural circadian rhythm which regulates sleep-wake cycle, cognitive performance, and other physiological functions go down in the afternoon, which may make it harder for medical professionals to maintain performance levels [8]. (3) Work shift in the afternoon. Anesthetists and nurses often change shifts in the afternoon, which might cause information loss or neglect. However, other studies have shown that sleep deprivation, or progressive fatigue during the work day did not increase the postoperative morbidity of the patients [18192021]. It is likely that in medical professional disciplines, physicians can adjust their work schedule, collaborate within teams, and regulate clinical procedures, with an endeavor to minimize adverse events caused by nontechnical factors [18].
Although surgery start time may not measurably affect the postoperative morbidity of patients due to self-regulation and wellness control by surgeons, it remains unclear whether the progressive fatigue of surgeons during a normal working day can significantly weaken their judgment and performance in surgery. The present study is important, as it is the first to investigate the long-term prognosis of HCC following morning versus afternoon HR. The patient characteristics, tumor feature, and surgical procedures were not significantly different between morning and afternoon surgery groups. Of note, the long-term prognosis was equivalent regardless of surgery start times.
In fact, the duration of operations beginning in the morning was longer than those performed in the afternoon in the current study (Table 2). Actually, major resection seemed to be more frequently performed in the morning than afternoon (18.4% vs. 10.0%, Table 2) and, generally, it seems true that complex operations are more likely arranged in the morning. As analyzed, patient demographics, liver function, and tumor characteristics were similar among patients undergoing morning versus afternoon surgery. This implied a relatively random assignment of patients to the day surgery. In fact, assignment of surgery is mostly determined by the operation and anesthesia department in our hospital, and each surgical team has 1 to 2 “normal operation days” due to limitation of operation rooms, which means their surgery can start at 8 AM. in the morning on these days. Therefore, most surgeons would like to arrange more complicated and difficult surgeries on “normal operation days.” It is not surprising that surgeons in the morning are more energetic, and have enough time to finish the operation during the daytime. However, as we noticed, the surgical margin, intraoperative blood loss, and transfusion, which might be more likely affected by progressive fatigue and subsequent inaccurate surgical performance of surgeons, were not different among patients undergoing morning versus afternoon surgery. As such, the OS was equivalent after morning versus afternoon surgery. These findings indicated that surgery start time had no significant influence on physician judgment, productivity, or performance, and therefore had no adverse oncological impacts on patients even when the operation was performed in the afternoon.
HR is a complex and high-risk surgery, and was mostly performed by experienced surgeons after at least 10-year professional training [26]. Experienced surgeons were unlikely to be affected by progressive fatigue when performing operations during a normal work day, as they are more self-regulated and adapted to this situation. Similarly, Slaughter et al. [27] reported that there was no association between surgery start time and long-term prognosis of patients undergoing minimally invasive surgery for gynecologic cancer. The findings of our study supports continued use of the current surgical practice in liver surgery. However, with significant increases in caseloads, the physical health of the physicians should be of concern as well in order to improve the efficacy and efficiency of operations on patients.
There were several limitations of the current study. First, as a retrospective and single-center study, some inherent biases could not be identified or excluded. Second, the time cutoff differentiating morning versus afternoon surgery was somewhat depending on the regular working time of these surgeons (8 AM–6 PM). It is possible other categories of morning versus afternoon surgery may have identified different results. Additionally, disease-free survival was not available in the current study due to inaccurate reports of recurrence or shift to local hospitals. Therefore, OS was utilized as the primary end point.
In conclusion, patients undergoing curative-intent HR appear to have been rather randomly assigned to morning and afternoon surgery. Surgery start times (morning versus afternoon) had no measurable influence on the long-term prognosis of patients. Physicians performing afternoon surgery had no obvious deviation of their judgment or skill even with progressive fatigue, as surgical margin, intraoperative blood loss, and transfusion were not different between afternoon and morning surgery. However, these null findings do not exclude the possible impacts of excessive fatigue of physicians, such as after 24 hours on-call or after a night emergency operation, on the prognosis of patients undergoing regular daytime surgery.
 XML Download
XML Download