

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Axillary lymph node dissection (ALND), along with mastectomy, has played an important role in the radical treatment and staging of breast cancer since it was introduced by Halstead [12]. However, there is a risk of complications such as lymphedema and axillary nerve damage, which can lead to poor quality of life [345].
Sentinel lymph node biopsy (SLNB) is considered a standard procedure for histologically identifying axillary lymph node metastasis in clinically node-negative breast cancer. With the introduction of SLNB, the number of ALNDs has decreased compared to that in the past. Furthermore, several clinical trials have been conducted on procedures that can be used to omit ALND even in SLNB with 1 or 2 axillary lymph node metastases [678]. The American College of Surgeons Oncology Group (ACOSOG) Z0011, a randomized trial, reported that there was no effect on the survival rate after omission of ALND for 1 or 2 lymph node metastases identified in SLNB in early breast cancer patients who underwent breast conservative surgery (BCS) [9]. In addition, as breast screening examination increases the early detection of breast cancer, the number of early breast cancer patients has increased [1011].
Although BCS is mostly performed in patients with early breast cancer, total mastectomy (TM) may be inevitable depending on various factors such as tumor location. Furthermore, the rate of mastectomy has increased again since 2013. This is because advances in imaging diagnosis such as magnetic resonance imaging have made it easier to diagnose a wide range of breast cancer and multiple breast cancers, and the National Health Insurance Service covers breast reconstruction for breast cancer and actively reflects patients' opinions on fear of recurrence or expectations of improved survival [121314]. However, although several studies have suggested that radiation therapy, usually involved in BCS, may have a therapeutic effect on residual lymph nodes [1516], lymph node metastasis in patients undergoing TM without radiotherapy has rarely been studied with SLNB alone. We used data from the Korean Breast Cancer Society registration system (KBCR) to evaluate the usefulness of ALND in patients with early breast cancer who had undergone TM with 1 or 2 lymph node metastases in the final pathology.
METHODS
Study design
This study enrolled patients older than 18 years with early breast cancer who underwent TM. The large-scale data of the KBCR were retrospectively analyzed. Since 1996, the KBCR has collected data from 110 training hospitals nationwide in Korea. The cause and date of death in these data were used in connection with the data of the Korea Central Cancer Registry (Ministry of Health and Welfare in collaboration with the Korean National Statistical Office) to compile complete death statistics which were updated through 2014. The study was approved by the Institutional Review Board of Daejeon St. Mary's Hospital (No. DC18RESI0041). The inclusion criteria were: TM and SLNB, pathologic T stage 1 or 2, clinically negative axillary lymph nodes, 1 or 2 positive axillary lymph nodes on final pathology, no radiation therapy, and no neoadjuvant therapy.
The basic clinical characteristics of patients assessed include axillary operation method, age, pathologic T stage, lymph node status, immunohistochemistry, histologic type, histologic grade, nuclear grade, lymphovascular invasion, number of metastatic lymph nodes, total number of lymph nodes, family history, menopausal status, position of tumor, adjuvant chemotherapy or hormonal therapy, and overall survival (OS).
As 2 groups for analysis, the SLNB only and SLNB + ALND groups were matched according to the maximum propensity scores (1:4). The factors matched included age, pathologic T stage, estrogen receptor or progesterone receptor status, human epidermal growth receptor 2 status, histologic grade, nuclear grade, and lymphovascular invasion. The primary endpoint was a comparison of the OS differences between the 2 groups. In addition, a subgroup analysis was performed to confirm the OS according to the axillary operation method for each clinical factor.
Study population
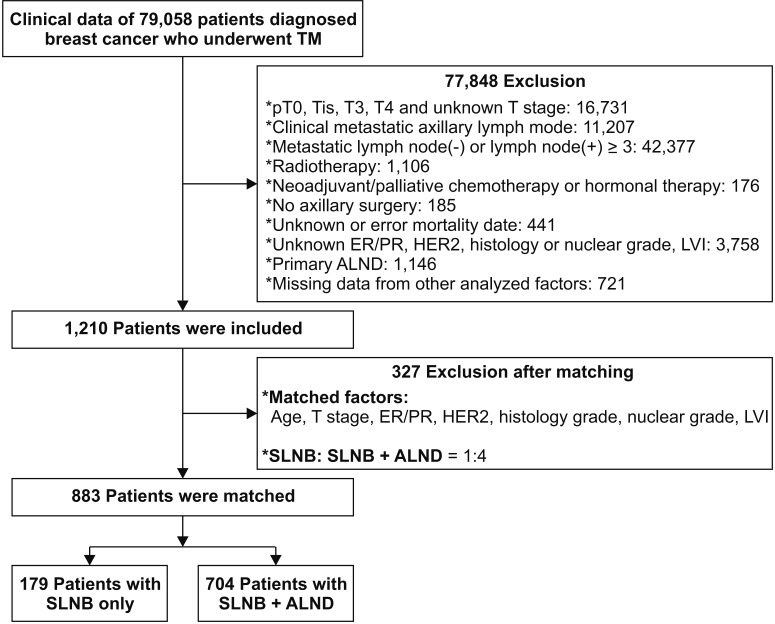
A total of 79,058 patients who underwent mastectomy were excluded as they did not meet the inclusion criteria or had insufficient data. The remaining 1,210 patients were matched by propensity scores using the matched factors, and a total of 883 patients were included in the analysis (Fig. 1). In addition, we compared the annual incidences of the SLNB only and SLNB + ALND groups among patients who met the diagnostic inclusion criteria: pathologic T stage 1 or 2, clinically negative axillary lymph nodes, and 1 or 2 metastatic axillary lymph nodes in the final pathology.
Statistical analysis
The clinical characteristics of patients in the matched cohort were compared using the chi-square test and the Student t-test. The differences in survival between the 2 groups were assessed via multivariate logistic regression analysis, the Kaplan-Meier method, and Cox proportional hazards regression analysis. Subgroup analysis, according to clinical factors, was used to identify factors that yielded differences in survival according to additional ALND. All statistical analyses were performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA), and P-value <0.05 was considered statistically significant.
RESULTS
Annual incidence of SLNB only or SLNB + ALND among patients who underwent TM with 1 or 2 metastatic axillary lymph nodes
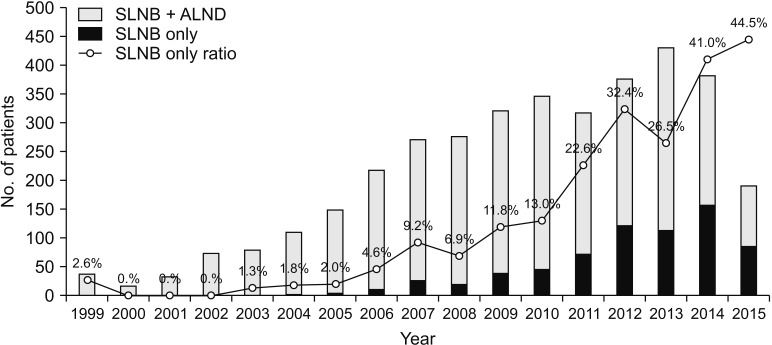
Of the 79,058 patients who underwent TM, 3,632 patients were met the diagnostic inclusion criteria. The numbers of performed SLNB only and SLNB + ALND have increased respectively and the proportion of only received SLNB also has increased from 1999 to 2015 (Fig. 2).
Clinical characteristics
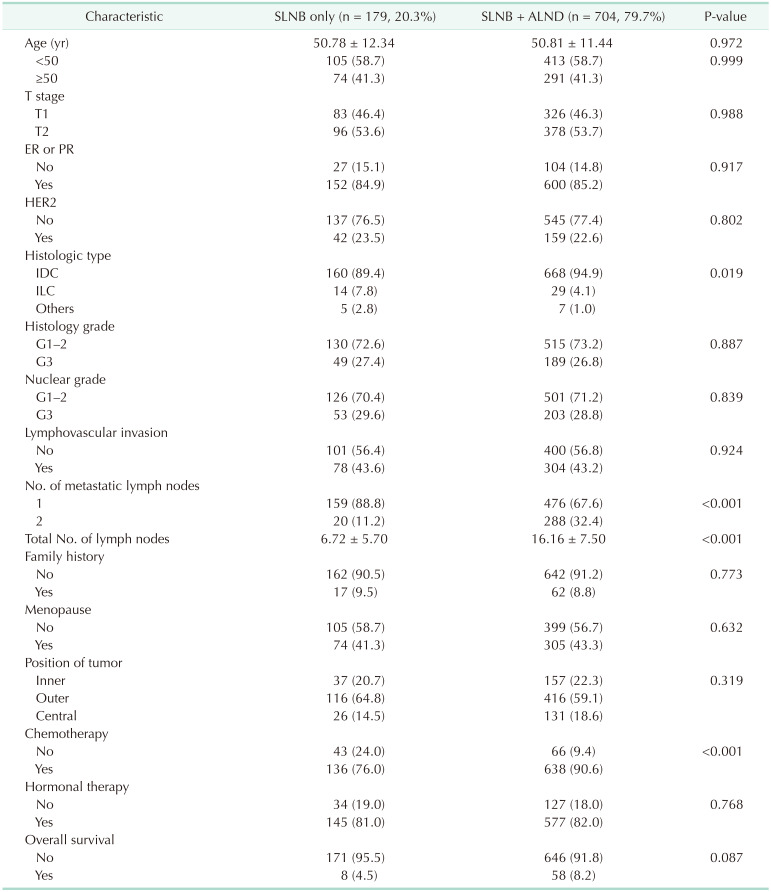
Among the 883 patients in the matched cohort from 1999 to 2014, the median follow-up period was 54.00 ± 36.946 months. Apart from the histologic type (P = 0.019), number of metastatic lymph nodes (P < 0.001), total number of lymph nodes (P < 0.001), and chemotherapy (P < 0.001), there were no significant differences in the other characteristics between the 2 groups (Table 1).
Factors associated with axillary dissection and survival
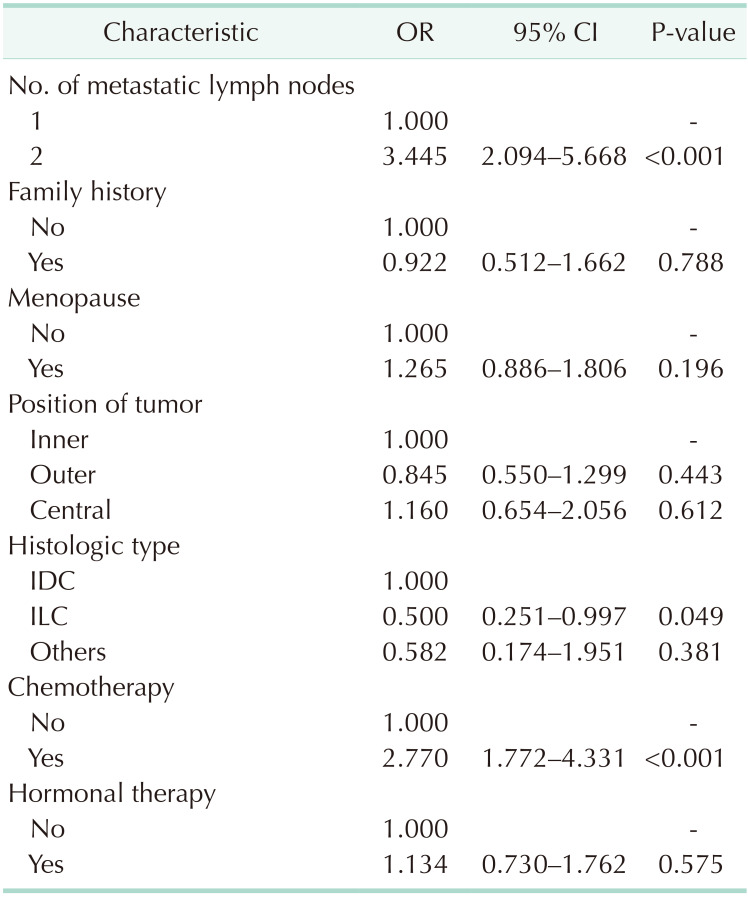
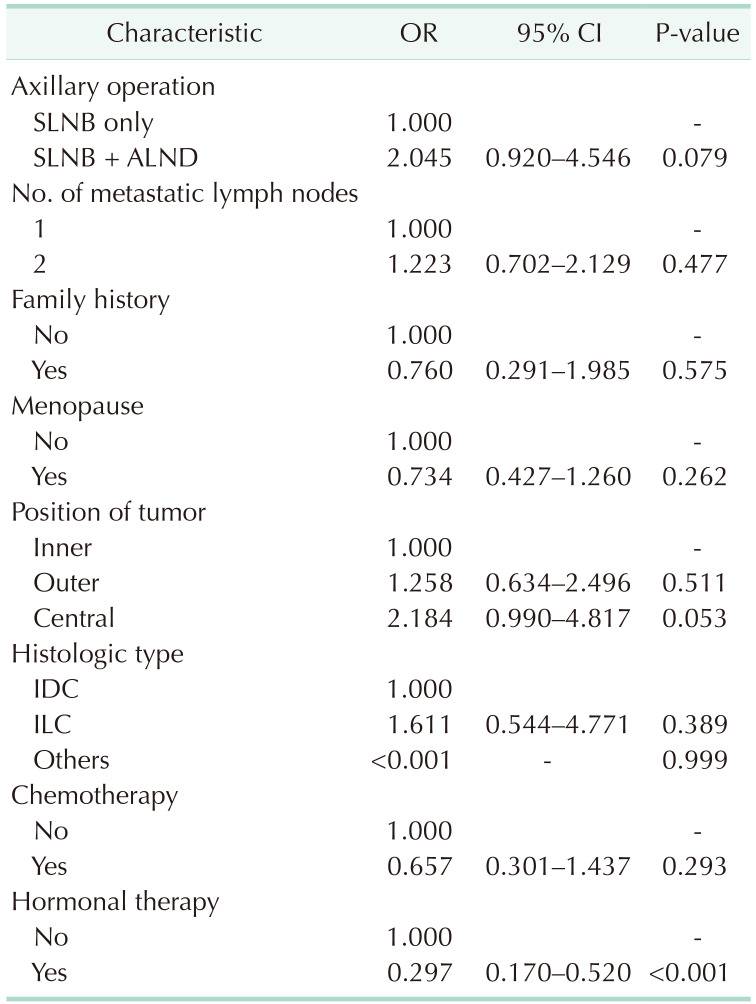
Multivariate logistic regression of factors apart from those matched revealed that ALND was more frequent among patients with 2 metastatic lymph nodes, invasive ductal carcinoma, and chemotherapy (Table 2) and that hormonal therapy significantly improved the OS (Table 3).
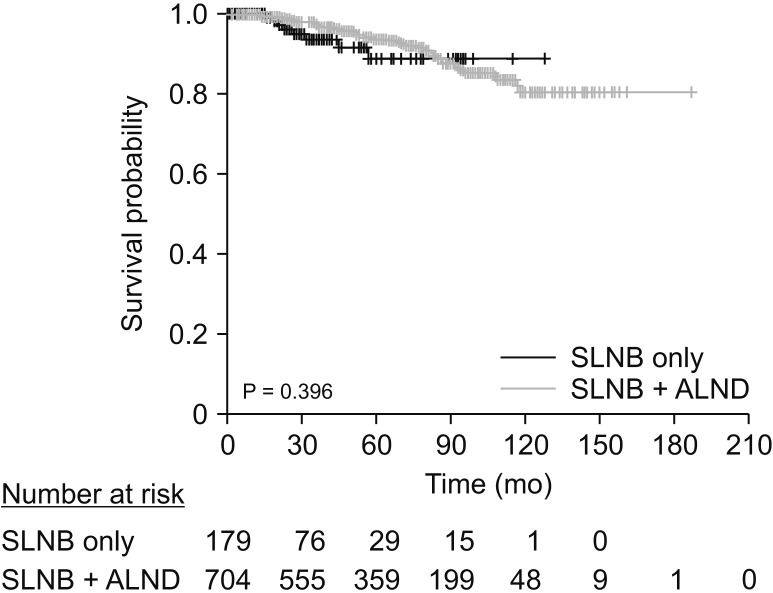
Kaplan-Meier survival analysis revealed no difference in OS between the SLNB only and SLNB + ALND groups (P = 0.396) (Fig. 3).
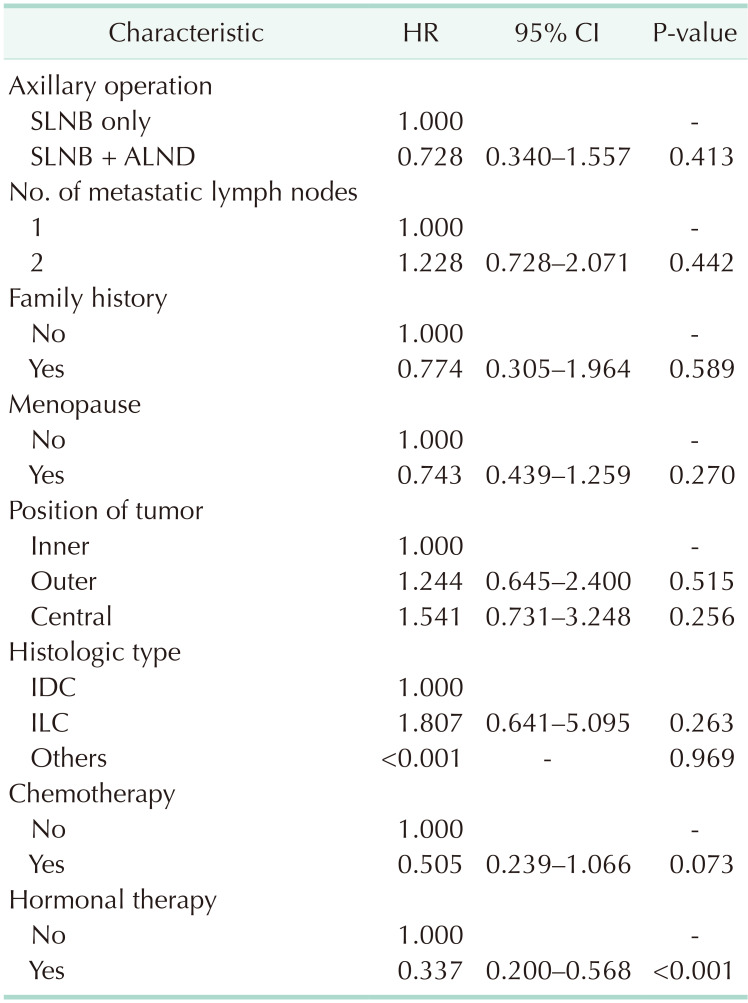
The Cox proportional hazards model revealed no difference in OS between the SLNB only and SLNB + ALND groups (hazard ratio [HR], 0.728; P = 0.413). Only hormonal therapy showed a significant survival benefit (HR, 0.337; P < 0.001) (Table 4).
Subgroup analysis
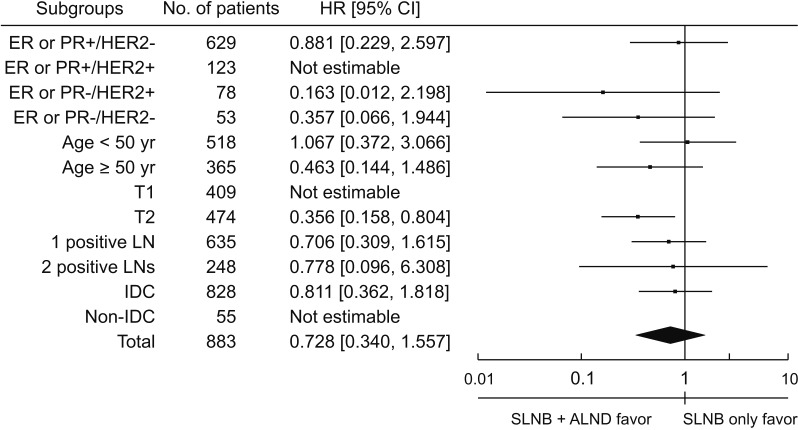
In the subgroup analysis, SLNB + ALND among patients in the stage T2 group showed survival benefits when assessed via Cox proportional hazards model divided by immunohistochemistry, age, T stage, number of metastatic lymph nodes, and histologic type (HR, 0.356; P = 0.013) (Fig. 4).
DISCUSSION
Our study revealed that additional ALND did not affect the survival rate among early breast cancer patients who underwent TM and SLNB with 1 or 2 axillary lymph node metastasis in the final pathology. In the ACOSOG Z0011, the median followup period among enrolled patients with 1 or 2 pathologically identified positive lymph nodes from SLNB was 6.3 years; the 5-year OS was 92.5% with SLNB and 91.8% with ALND [9]. Our study included patients with 1 or 2 metastatic lymph nodes in the final pathology, unlike the ACOSOG Z0011. The median follow-up period was 4.5 years, and the 5-year OS was 88.8% with SLNB and 93.6% with ALND. Similar to the present study, Lee et al. [17] reported that there was no difference in OS regardless of ALND among patients with early breast cancer who underwent BCS with 1 or 2 positive lymph nodes in the final pathology. FitzSullivan et al. [18] reported that there was no significant difference in recurrence-free survival and OS among patients with metastatic lymph nodes from TM and SLNB regardless of additional ALND or irradiation. In this regard, the omission of ALND may be expected to reduce morbidity and improve the quality of life among early breast cancer patients who underwent TM and SLNB with 1 or 2 axillary lymph node metastasis.
In this study, there were some cases where ALND was omitted prior to the announcement of the ACOSOG Z0011 results. Since the design of our study is retrospective, we were not able to determine the exact reason why ALND was omitted on such cases. However, given that there were several studies prior to 2011 on the omission of ALND in breast cancer patients with favorable features [1920], we presumed that those studies provided basis for ALND omission.
There was no difference in adjuvant chemotherapy rates between the SLNB and ALND groups in ACOSOG Z0011. However, in our study, the adjuvant chemotherapy rate was relatively higher in the SLNB + ALND group (90.6%) than in the SLNB only group (76.0%) (P < 0.001). Considering that 27.3% of patients had nonsentinel lymph node metastasis in ACOSOG Z0011 [21], although there is a possibility that some metastatic lymph nodes remain and the relatively low adjuvant chemotherapy rates in the SLNB only group of our study, the lack of difference in survival seems to be a meaningful result.
The survival rate was higher among patients who received hormonal therapy than among those who did not. This seems to be in the same context that, as is known, patients with hormone receptor positive disease showed a better survival rate than did those with hormone receptor negative disease [22232425].
The most common histologic type in this study was invasive ductal carcinoma, and invasive lobular carcinoma was rare (4.9%). The proportion of patients with invasive lobular carcinoma was relatively high in the SLNB only group, but there was no difference in survival rate according to histologic type. In some studies, ALND was not related to survival in invasive lobular carcinoma meeting the ACOSOG Z0011 criteria [2627].
In the subgroup analysis, unlike the T1 subgroup, additional ALND resulted in a significantly higher survival benefit than SLNB only in the T2 subgroup. Considering that nonsentinel lymph node metastasis was related to tumor size in other studies [2829], even if it is included in the category of early breast cancer, it is necessary to subdivide it to consider additional ALND.
In ACOSOG Z0011, tangential field whole breast irradiation was performed after BCS in all patients, which partially included or did not include the axillary field [1516]. Radiotherapy as adjuvant therapy was the main target of residual breast tissue after BCS. Axillary irradiation may have been secondarily included in the tangential field according to the radiologist's findings, but this was not the main adjuvant therapy. In this study, TM itself was not an indication for tangential field whole breast irradiation. In AMAROS trial, there was no difference in survival between the ALND group and the axillary radiotherapy group in early breast cancer patients with sentinel lymph node metastasis [30]. On this basis, adjuvant radiotherapy after TM was excluded to rule out the effects of adjuvant therapy in the axillary field.
The main strengths of this study were that we reduced confounders via propensity score matching and increased the reliability by assessing more homogenous populations. However, this study has several limitations. First, it was a retrospective study. Additionally, limited information was available on prognosis, such as recurrence or breast cancer specific survival. Then, prognosis was assessed using OS. However, there was a possibility that other factors might have been involved in mortality. Furthermore, in the SLNB + ALND group, the total and metastatic lymph nodes were registered as the mixture of data regarding sentinel lymph nodes and additional dissected lymph nodes, which limited their further analysis. Most of the analysis data contained data from 2010 onwards, so the follow-up period was rather short. Finally, the matched factors were mainly the pathological factors of breast cancer, and there is a possibility that the analysis result might be influenced by selection bias of other unmatched factors.
In this study, we confirmed that there was no difference in the patients' survival rate regardless of additional ALND even among early breast cancer patients who underwent TM and SLNB with 1 or 2 axillary lymph node metastases in the final pathology. Although further studies are needed, omission of ALND may be considered in selected patients.
 XML Download
XML Download