

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pancreatic cystic neoplasms (PCNs) account for approximately 30% of resected pancreatic tumors [123]. Due to the increased use of sophisticated imaging modalities and advances in imaging techniques, detection rates for PCNs have gradually increased [4]. There are 4 common categories of PCN including: intraductal papillary mucinous neoplasm (IPMN); serous cystic neoplasm (SCN); mucinous cystic neoplasm (MCN); and solid pseudopapillary neoplasm [1]. Of these, IPMN, MCN, and SCN are recommended to be surgically removed due to their malignant potential [5678].
Although symptomatic SCNs should be surgically removed, regular surveillance of asymptomatic SCNs is generally recommended due to lower malignant potential compared with other PCNs [9]. However, some SCNs do not exhibit the typical honeycomb pattern, and their atypical appearance makes it difficult to discriminate SCNs from other potentially malignant PCNs and to decide whether to perform the surgery [10]. If surgeons could accurately distinguish SCNs from other PCNs, unnecessary operations would be decreased. Therefore, the aim of this study was to evaluate the causes of resection for SCN, to investigate the clinical and radiological features of SCNs that are surgically resected, and to compare the characteristics of SCNs that were diagnosed accurately and those misdiagnosed.
METHODS
Patients and materials
This was a retrospective study that analyzed prospectively collected medical data. Between 2000 and 2014, patients who underwent surgical resection and were diagnosed with pathologically confirmed SCN were included. Patients with incomplete radiological data were excluded. All patients underwent preoperative multidetector CT using either the Brilliance 64 (Philips Medical Systems, Cleveland, OH, USA) or LightSpeed Ultra (GE Healthcare, Little Chalfont, UK) instruments. Additional MRI using the Magnetom Verio (Siemens Healthcare, Erlangen, Germany) system was performed as required.
Clinical factors included age, sex, roots of detection of the lesions, preoperative diagnosis, tumor location, reason(s) for surgery, and operation type. The department of radiology of the authors' institution provided the reporting form for PCNs, which included radiological characteristics including type of cyst (microcystic or macrocystic), tumor size, calcification, central scar, solid component(s), cystic wall thickening, septation in the cyst, enhancing lesion, pancreatic duct dilatation, bile duct dilatation and pancreas atrophy, and suggested all possible diagnoses according to these radiological characteristics. Type of cyst, and other radiological characteristics were defined based on the authors' previous report [10]. Briefly, cysts were classified as microcystic if they were < 2 cm in size, and macrocystic when ≥ 2 cm. The typical “honeycomb” appearance was included among the microcystic features. All radiological images were reviewed by one specialized pancreatobiliary radiologist.
This study was approved by the Institutional Review Board of Seoul National University Hospital (No. 1606-086-771), and all patients consented to participate in this study.
Statistical analysis
Categorical variables were compared using the chi-square test and continuous variables were compared using Student t-test. Differences were considered to be statistically significant at P < 0.05 in 2-tailed testing. All statistical analyses were performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
Clinical variables and radiological features
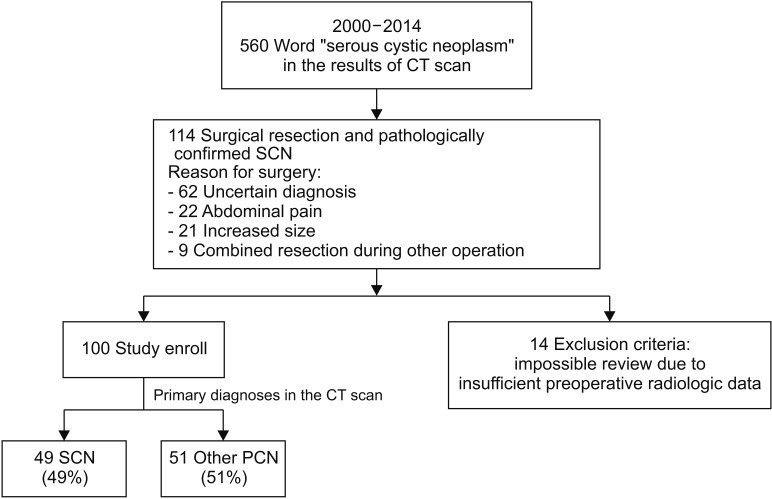
A flowchart illustrating patient enrollment is presented in Fig. 1. Overall, 560 patients were potentially diagnosed with SCN, which was described in the CT scan reports. Most patients underwent regular surveillance, and 114 underwent surgical resection and SCN was pathologically confirmed. All of the excluded patients (n = 14) underwent preoperative radiological examinations in another hospital; therefore, imaging data were not recorded in the medical database and could not be reviewed. Ultimately, 100 patients were included in the present study. There were no cases of serous cystadenocarcinoma.
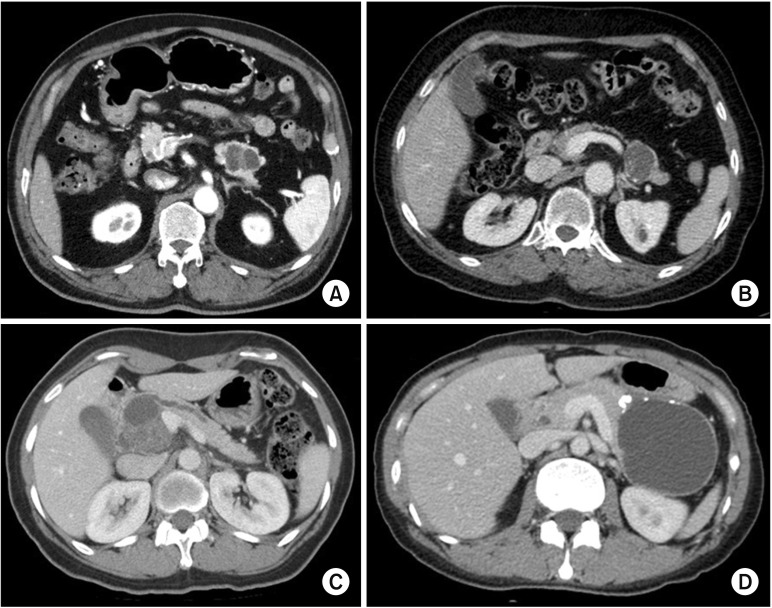
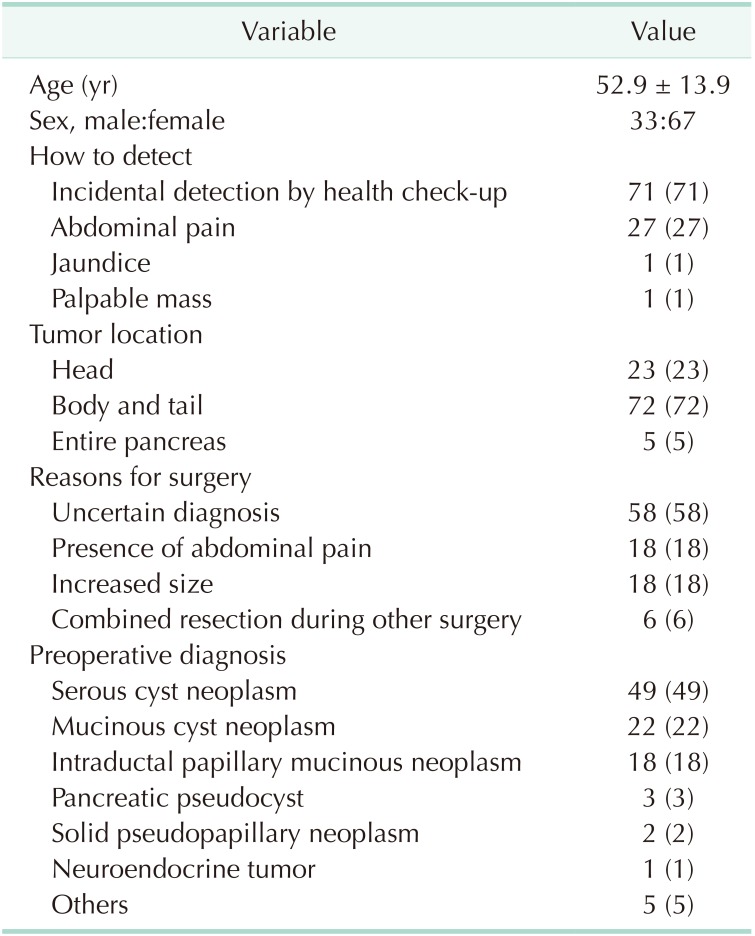
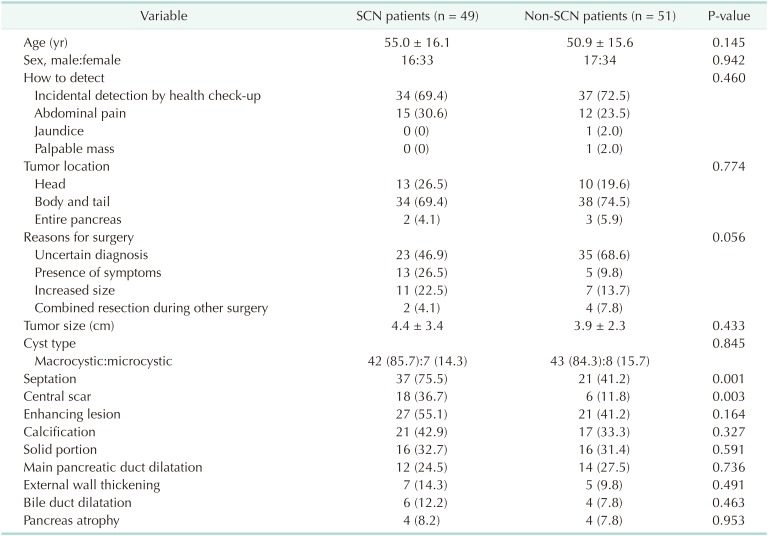
The mean age of the patients was 52.9 years and 67 (67%) were female (Table 1). Seventy-one patients (71%) had their PCNs incidentally detected at a regular health check-up, 27 (27%) were due to abdominal pain, 1 (1%) due to jaundice, and 1 (1%) due to a palpable mass. Seventy-two patients (72%) had the PCN in the pancreatic body and tail. Reasons for surgery included uncertain diagnosis (n = 58, 58%), symptomatology (n = 18, 18%), and combined resection during other surgery (n = 8, 8%). Of patients with an uncertain diagnosis, 10 were preoperatively diagnosed with possible malignant lesions, in which the most probable preoperative diagnoses were: IPMN with invasive carcinoma (n = 5); pancreatic head cancer (n = 2); pancreatic tail cancer (n = 2); and multiple metastases from renal cell carcinoma (n = 1). The preoperative diagnoses were SCN (n = 49, 49%) (Fig. 2A), misdiagnosed MCN (n = 22, 22%) (Fig. 2B), misdiagnosed IPMN (n = 18, 18%) (Fig. 2C), and misdiagnosed pancreatic pseudocyst (n = 3, 3%) (Fig. 2D).
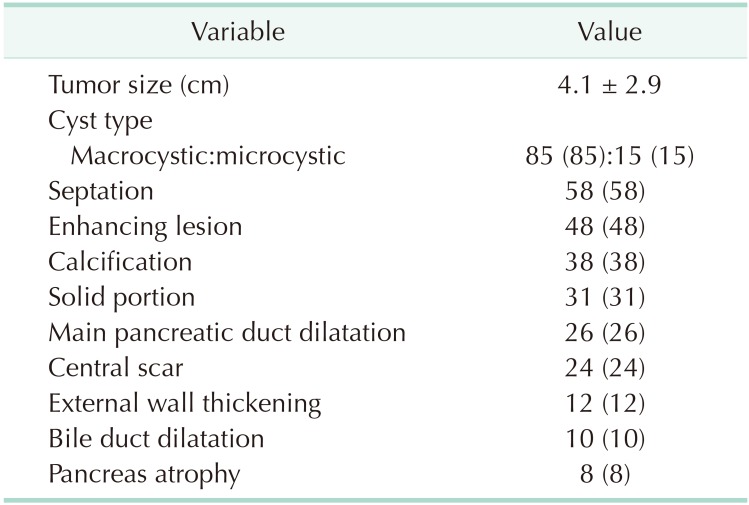
The radiological characteristics of all patients are summarized in Table 2. The mean tumor size was 4.1 cm. Because only patients with surgically resected SCNs were enrolled in this study, most lesions exhibited macrocystic features (n = 85, 85%), followed by microcystic appearance (n = 15, 15%). Septation in the cyst was evident in 58 (58%) patients, enhancing lesions in the cyst in 48 (48%), and calcification in the cyst in 38 (38%).
Comparisons of clinical and radiological features according to preoperative diagnoses
Patients were divided into 2 groups: those preoperatively diagnosed with SCN (n = 49, 49%); and those who were diagnosed with lesions other than SCN (n = 51, 51%). The clinical and radiological characteristics of the 2 groups are compared in Table 3. There were no significant differences in clinical features between the 2 groups. In terms of radiological features, septation (75.5% vs. 41.2%, P = 0.001) and central scar (36.7% vs. 11.8%, P = 0.003) were more prevalent in patients preoperatively diagnosed with SCN.
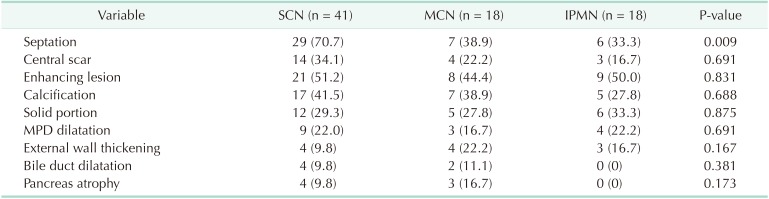
A comparison of radiological features according to preoperative diagnoses for those with macrocystic neoplasms is shown in Table 4. Macrocystic lesions did not exhibit different radiological features among the preoperative diagnoses, although septation in the cyst was more prevalent in those accurately diagnosed with SCN compared with those preoperatively misdiagnosed with MCN or IPMN (70.7 vs. 38.9 vs. 33.3%, respectively, P = 0.009).
DISCUSSION
PCNs are increasingly being detected due to increased use of radiological examinations [411]. Whereas IPMNs and MCNs consist of columnar epithelium, which produces mucin, and have a relatively high malignant potential, SCNs have a single layer of either cuboidal or flattened cells, and malignant SCNs have been reported in a very limited number of cases [27121314]. Therefore, surgical indications for SCNs have not been based on oncological potential, but generally on large size, symptomatology, and difficult or impossible discrimination from other potentially malignant lesions [1516]. However, because pancreatectomies are associated with a high morbidity rate, surgical resections of benign SCNs have also caused postoperative complications that would be preventable if the benign SCNs had been initially accurately diagnosed [171819].
The present study investigated 100 consecutive patients who were diagnosed with pathologically confirmed benign SCN after complete surgical resection. Most lesions were discovered incidentally at health check-up (71%) or due to abdominal pain (27%) (Table 1). Most patients underwent surgical resection due to uncertain preoperative diagnosis (58%), with 51 lesions (51%) preoperatively diagnosed as non-SCNs. In other words, if the benign SCNs had been accurately diagnosed, more than onehalf of patients could have undergone close observation instead of surgical resection.
In our previous report, we mentioned that the opposite of “microcystic” was “macrocystic,” not “oligocystic,” and proposed that the “oligocystic SCN” according to the World Health Organization classification should be revised to “macrocystic SCN” [1020]. We also suggested that macrocystic SCN could be divided into 2 subtypes: “unilocular” and “multilocular.” The most representative radiological feature of SCN (i.e., honeycomb appearance) was included in the microcystic SCN [16]. Generally, macrocystic SCNs are detected in <10% of all SCN patients [1621]. However, one large-scale study recently reported that macrocystic SCNs were detected in 32% of cases, and mixed macrocystic/microcystic in 18% [22]. In this study, 85% of SCNs exhibited macrocystic features (Table 2). This was because the present study enrolled surgically resected SCNs, not those that had undergone regular surveillance. Although we attempted to evaluate radiological differences in macrocystic tumors among the preoperative diagnoses, no significant difference was revealed, except for septation (Table 4). This result was in accordance with our previous study, in which CT could differentiate macrocystic unilocular SCN with low diagnostic accuracy [10].
Furthermore, the enrolled SCNs exhibited other radiological features such as enhancing lesions (48%), calcification (38%), solid component (31%), and main pancreatic duct dilatation (26%) that were representative of other PCNs including MCN, IPMN, and pseudocyst (Table 2). Microcystic honeycomb appearance is a representative feature of typical SCNs (Fig. 2A). However, some radiological features, such as a macrocystic lesion with calcification (Fig. 2B), a cystic lesion with a solid component and the presence of main pancreatic duct dilatation (Fig. 2C), and a cystic lesion with evenly-thickened wall with multiple calcifications (Fig. 2D), made it difficult to distinguish between SCN and other PCNs. Although 49 patients were preoperatively diagnosed with SCN, 23 (46.9%) underwent surgical resection due to uncertain diagnoses (Table 3). Conventional radiological examination provides fundamental information to the clinician, but cannot exactly diagnose atypical SCNs, which can mimic other PCNs.
As mentioned earlier, surgical indications for SCNs remain controversial. Tumor size > 4 cm has been generally accepted because larger lesions tend to cause symptoms [1423]. Furthermore, laparoscopic surgery becomes more difficult if tumors grow larger than a specific size due to small available operation field [2425], or chronic inflammation around the cystic mass. Hwang et al. [2425] suggested the timely and active surgery, especially for pancreatic body or tail SCN of more than 3 cm at detection, because laparoscopic distal pancreatectomy already proved to be safe and feasible. Two studies reported that cyst growth rate was not related to initial cyst size [2627]. Recently, one large-scale European study reported that cyst size ≥ 4 cm exhibited a faster cyst growth rate than those < 4 cm [22]. Despite these results, the authors argued that whether size or growth rate criteria was an appropriate surgical indication remained questionable [222728]. Although symptom resolution is also an essential goal of surgery, not all SCNs are associated with abdominal pain [22]. Therefore, surgical resection could be considered if SCNs are associated with abdominal symptoms or growth into a large cyst, even if the diagnosis of SCN is highly suspected.
The distinction between SCNs and other PCNs is worldwide, long-term task. Recently, endoscopic ultrasonography (EUS) or EUS-guided fine-needle aspiration (FNA) biopsy has been performed to diagnose PCNs accurately. However, EUS or EUSguided FNA biopsy was not helpful in diagnosing benign SCNs that it had low sensitivity with high specificity that was not superior to CT or MRI [222829]. In addition, EUS-guided FNA biopsy had always potential peritoneal dissemination in case of malignant tumor [30]. Therefore, EUS or EUS-guided biopsy would be helpful for selected lesions that could not be distinguished from other potentially malignant diseases.
In conclusion, it is difficult to accurately distinguish atypical SCNs from other PCNs using conventional radiological examinations, especially macrocystic SCNs. For more accurate diagnosis, new biomarkers and/or other diagnostic modalities are needed and, thus, warrant further investigation.
 XML Download
XML Download