

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Pancreatoduodenectomy (PD) is one of the most challenging abdominal surgeries, which requires complicated anastomosis. Since Whipple reported the first one-stage operation for complete excision of the head of the pancreas and the entire duodenum in 1940, the surgical techniques and postoperative managements have constantly evolved over the decades [1]. Nowadays, the safety of this operation has improved; its morbidity and mortality rates have been lowered to 18%–43% and 1%–2.3%, respectively [234].
Recently, the surgical outcomes and long-term prognosis in patients with gastric cancer have improved due to the development of imaging modalities, surgical techniques, and the regimens of adjuvant chemotherapy [5678]. Most patients with gastric cancers have frequent postoperative follow-up every 3 or 6 months using various high-resolution imaging modalities, including CT and/or MRI. Therefore, the detection rates of the pancreatobiliary lesions in patients who underwent previous gastrectomy have increased [910].
Despite the difficulties mentioned above, PDs are being performed in patients with a history of gastrectomy. However, little is known about the clinical outcomes of the patients who underwent secondary PD after previous gastrectomy. Many studies were case series due to the difficulty in collecting a large cohort of these patients from a single institution [11121314151617]. Although there was also one multicenter study, case number was also not large enough [9].
Therefore, this study was designed to analyze a relatively large number of patients who underwent secondary PD after previous subtotal or total gastrectomy (TG) in a high-volume tertiary referral center. We also evaluated the clinical outcomes of these patients and compared them with the patients who underwent conventional PD without history of previous gastrectomy using a statistical compensation method.
Go to : 
METHODS
Study population
The study protocols were approved by the Institutional Review Board of Seoul National University Hospital (IRB No. H-1705-031-852) and informed consent was waived by the board. The electronic medical records of 1,722 patients who underwent PD between January 2000 and December 2014 were retrospectively reviewed. The preoperative status of the patients was evaluated with body mass index (BMI), American Society of Anesthesiologists physical status classification, and age-adjusted Charlson Comorbidity Index. The factors associated with the operation and the postoperative clinical outcomes were analyzed and compared according to the absence and presence of previous gastrectomy history. Among the patients who underwent PD, the control group was defined as patients who had never experienced surgery associated with the stomach (patients who underwent simple cholecystectomy and appendectomy were included in the control group). In order to overcome the statistical errors that may occur from the discrepancy in the number of study population between the secondary PD after previous gastrectomy group (gastrectomy group) and conventional PD without history of gastrectomy group (no gastrectomy group), propensity score matching (PSM) analysis was also performed.
Surgical procedures according to the previous operations
During PD, we performed 3 anastomoses using the Child method and standard lymph node dissection (LND) which included the lymph nodes (LNs) around the pancreas (LN 13, 17), hepatoduodenal ligament (LN 12), and gallbladder (LN 12c) [318]. When the tumor invaded other organs or resectable vessels, combined resection manifested organ/vessel and appropriate reconstruction was performed.
Fig. 1A shows the reconstruction in the cases of secondary PD after previous subtotal gastrectomy (STG) with Billroth I anastomosis (BI). In this case, previous gastroduodenostomy (G-D) did not affect the new reconstruction of PD. After further resection of the stomach including previous G-D, anastomoses (pancreaticojejunostomy [P-J], choledochojejunostomy [C-J], and gastrojejunostomy [G-J]) could be performed in the usual PD manner.
 | Fig. 1Resection and reconstruction methods used in these patients. (A) STG Billroth I. (B) STG Billroth II. (C) TG with Roux-en-Y esophagojejunostomy. STG, subtotal gastrectomy; BI, Billroth I; BII, Billroth II; TG, total gastrectomy; C-J, choledochojejunostomy; P-J, pancreaticojejunostomy; G-J, gastrojejunostomy; E-J, esophagojejunostomy. Solid red lines indicate resection of the stomach or jejunum; dashed red lines indicate resection of the pancreas.
|
The reconstruction method in the patients with secondary PD after previous STG with standard Billroth II anastomosis (BII) is illustrated in Fig. 1B. In this group, previous G-J was preserved. After resecting the previous afferent jejunal loop (duodenum and proximal jejunum) just proximal to the G-J, P-J, and C-J were performed using the distal jejunum. Then, jejunojejunostomy (J-J) was performed in the Roux-en-Y manner.
In the patients who underwent a secondary PD after previous TG, the previous esophagojejunostomy (E-J) was preserved (Fig. 1C). After Roux limb and biliopancreatic limb were separated at the level of previous J-J, P-J, and C-J were performed using the distal jejunum. Then, J-J was made between the distal jejunal limb and efferent limb from the E-J in the Roux-en-Y manner.
Postoperative management and follow-up
Every patient had 3 closed suction drains around the anastomosis. Although there were some differences depending on the general condition of each patient, postoperative diet was started sequentially from postoperative day (POD) 1 (sips of water on POD 1 and soft blended diet on POD 4). The laboratory test including amylase concentration in serum and intraabdominal drain fluid was assessed every other day (POD 1, 3, 5, and 7) and postoperative CT scan was performed on POD 4 or 5.
Postoperative pancreatic fistula (POPF) was diagnosed when the amylase concentration in the drainage fluid was over 3 times greater than the upper limit of the normal serum value after POD 3, in accordance to the criteria of International Study Groups on Pancreatic Fistula [19]. The pancreatic fistula grades B and C were considered as clinically relevant POPF.
Statistical analysis
All statistical analyses were performed with IBM SPSS Statistics ver. 22.0 (IBM Corp, Somers, NY, USA) and R environment ver. 2.13.0 (The R Foundation for Statistical Computing, Vienna, Austria). Nominal data were compared by chi-square tests, and continuous data by Student t-tests or analysis of variance with post hoc tests. Two-sided P-values less than 0.05 were considered statistically significant. To reduce selection bias inherent to retrospective observational studies and extreme differences in the number of cases between the groups, a one-to-one matching analysis was performed between the gastrectomy group and no gastrectomy group. To estimate the propensity score, a function was built by logistic regression model for the presence of history of prior gastrectomy on the bias of patient's clinical factors. The propensity score was calculated with preoperative factors included age, sex, and malignancy of the lesions.
Go to :
RESULTS
Demographic findings of entire patient cohort and gastrectomy group
Of the total 1,722 patients who underwent PD during the study period, the male to female ratio was 1:0.62 and the mean age was 63.3 years. The mean operation time was 332.1 minutes and the mean number of retrieved LNs was 14.1. The mean estimated blood loss (EBL) during operation was 447.8 mL and 207 patients (12.0%) had transfusion. Of the patients, 147 patients (8.5%) experienced postoperative complications of Clavien-Dindo classification III or higher, and 224 patients (13.0%) had clinically relevant POPF. The mean postoperative hospital stay was 16.9 days.
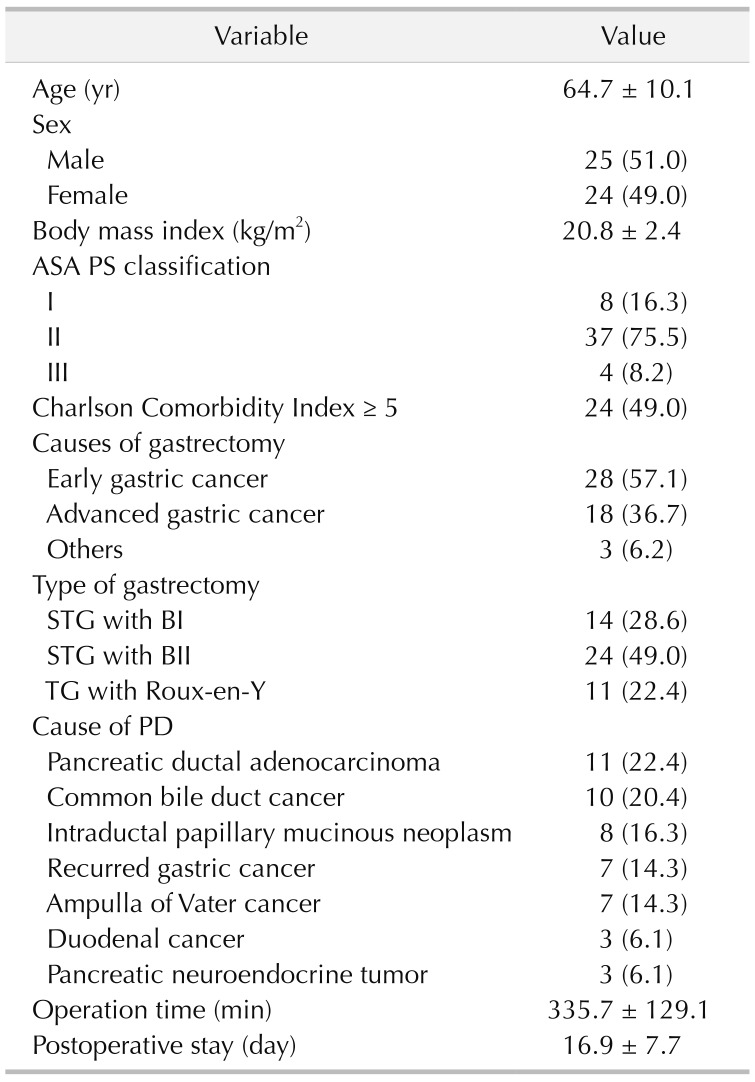
The demographic findings of the patients who had a history of prior gastrectomy are summarized in Table 1. Forty-nine patients (2.8%) with previous history of gastrectomy received secondary PD. Types of previous gastrectomy included 14 (28.6%) of STG with BI, 24 (49.0%) of STG with BII, and 11 (22.4%) of TG with Roux-en-Y J-J. Gastric cancer was the most common cause of prior gastrectomy (93.8%), followed by gastric adenoma with high-grade dysplasia (2.0%), lymphoma (2.0%), and ulcer perforation (2.0%). The most common cause of the secondary PD was pancreatic ductal adenocarcinoma (22.4%), followed by common bile duct cancer (20.4%). The mean interval from prior gastrectomy to the secondary PD was 67.3 months. There was no mortality case until 3 months after secondary PD and no reoperation. One patient was readmitted and underwent conservative management for 4 days due to postoperative ileus.
Comparison of clinical outcomes according to the presence of the history of prior gastrectomy
Table 2 shows the differences of clinical outcomes between the 2 groups before and after PSM analysis. When the 49 patients who underwent previous gastrectomy were compared with the 1,673 who did not, analysis showed that BMI (20.8 ± 2.4 kg/m2
vs. 23.3 ± 3.4 kg/m2, P < 0.001) and retrieved LNs (8.9 ± 8.1 vs. 14.2 ± 5.6, P = 0.001) were significantly lower, whereas EBL (729.5 ± 842.1 vs. 442.8 ± 465.4, P = 0.001), transfusion rate (36.7% vs. 11.3%, P < 0.001), and the incidence of complication of over Clavien-Dindo classification III (36.7% vs. 8.1%, P = 0.043) were higher in the gastrectomy group. Most of the details with complications of over Clavien-Dindo classification III were postoperative POPF, intra-abdominal fluid collection, and wound problem. Operation time (335.7 ± 129.1 vs. 332.0 ± 85.5, P = 0.773), rate of clinically relevant POPF (14.3% vs. 13.0%, P = 0.572), and duration of postoperative hospital stay (17.6 ± 9.1 vs. 20.1 ± 18.9, P = 0.355) were comparable in the 2 groups.
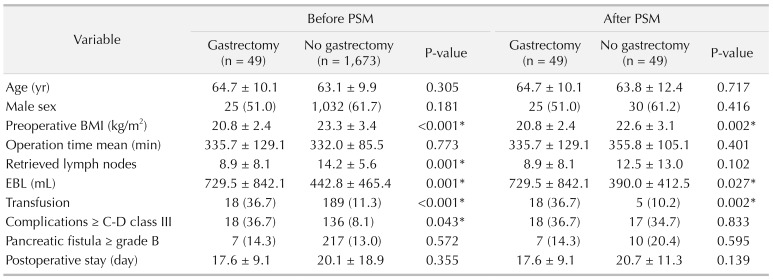
To reduce the statistical errors related to the significant differences in the number of patients between these 2 groups, we performed additional one-to-one PSM analysis using age, sex, and malignancy. After PSM analysis, the differences in preoperative BMI (20.8 ± 2.4 kg/m2
vs. 22.6 ± 3.1 kg/m2, P = 0.002), EBL (729.5 ± 842.1 vs. 390.0 ± 412.5, P = 0.027), and transfusion rate (36.7% vs. 10.2%, P = 0.002) remained statistically significant between the groups. However, the mean number of retrieved LNs and the complication (Clavien-Dindo classification III or higher) rate were no longer significant after PSM analysis.
Comparison of clinical outcomes according to the types of prior gastrectomy
Comparison of clinical outcomes according to the 3 types of gastrectomy (STG BI vs. STG BII vs. TG) are shown in Table 3. The transfusion rate was significantly higher in the STG BII subgroup than in the STG BI and TG subgroups (STG BI, 21.4% vs. STG BII, 54.2% vs. TG, 18.2%, P = 0.046); this finding was also observed when patients with combined resection were excluded (18.2% vs. 47.1% vs. 0%, P = 0.027). The BMI (21.0 ± 3.2 vs. 21.0 ± 2.0 vs. 20.1 ± 2.1, P = 0.538) were comparable among the 3 groups, as well as the mean EBL (452.3 ± 144.9 vs. 851.7 ± 899.7 vs. 785.9 ± 1,173.7, P = 0.391) and the mean number of retrieved LNs (11.2 ± 12.4 vs. 7.5 ± 5.7 vs. 9.8±6.0, P = 403). The postoperative complications were evaluated including clinically relevant POPF, delayed gastric emptying, ileus, wound problem, and intra-abdominal fluid collection. The incidence of postoperative complications and complications of over Clavien-Dindo classification III were similar among the 3 groups (23.1% vs. 41.7% vs. 45.5%, P = 0.443). Also, mean postoperative hospital stay was comparable in the 3 groups. (13.9 ± 8.2 vs. 19.8 ± 8.3 vs. 16.4 ± 5.9, P = 0.181).
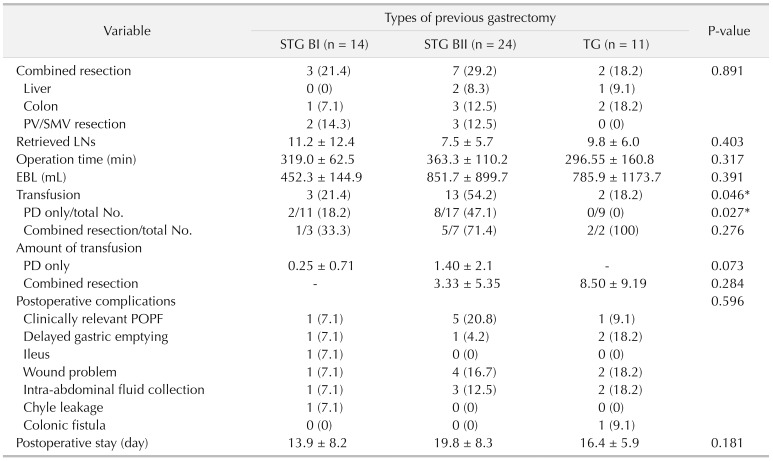
Table 3
Comparison of clinical outcomes according to the types of previous gastrectomy
Values are presented as number (%) or mean ± standard deviation.
STG, subtotal gastrectomy; BI, Billroth I; BII, Billroth II; TG, total gastrectomy; PV, portal vein; SMV, superior mesenteric vein; LNs, lymph nodes; EBL, estimated blood loss; PD, pancreatoduodenectomy; POPF, postoperative pancreatic fistula.
*P < 0.05, statistically significant difference.
![]()
Go to :
DISCUSSION
PD remains one of the most challenging surgeries among abdominal surgeries. This challenging surgery can become even more complex in patients with previous operation history, especially if gastrointestinal surgery. Previous gastric surgery may alter the anatomy of the alimentary tract and cause a significant amount of adhesion around the surgical field of PD. Despite the challenges, PD after previous gastrectomy is possible and continues to be performed. However, there is only a very limited number of reports on secondary PD in patients with a history of previous gastrectomy. Most of the previous reports are case reports or case series of less than 10 patients [111214151617]. Lee et al. [9] reported a multicenter study about secondary PD in patients with a history of previous gastrectomy in 2017. They analyzed 39 patients and confirmed the safety and feasibility of secondary PD, based on results which were similar to those of our study.
To our knowledge, this is the first study to compare the clinical outcomes of secondary PD after prior gastrectomy and primary conventional PD using the largest study population based on the unified surgical maneuver from a single institution.
Gastric cancer is one of the most common malignancies in Asian countries, such as Korea, Japan, and China [567]. For this reason, we are able to find the pancreatobiliary tumors in patients with a history of gastric surgery more frequently in these countries. In addition, the treatment outcome of gastric cancer has been so greatly improved that the number of gastric cancer survivors is increasing. Furthermore, because these patients receive regular follow-up using high-resolution cross-sectional imaging techniques, incidental detection of pancreatobiliary tumors is becoming more frequent nowadays [2021]. For such reasons, confronting pancreatobiliary neoplasm in need of PD in patients who have received previous gastric surgery is not such a rare occasion today, especially in Asian countries. Therefore, surgeons need to be familiar with the operative techniques and the unique outcome of PD in these patients.
There are several challenges in performing a secondary PD in patients with previous gastrectomy. First of all, because gastric surgery, especially if it was cancer surgery, shares the operation field with PD, much adhesion is formed around the hepatoduodenal ligament, the common hepatic artery, and the anterior/superior surface of the pancreas. This results in difficulty and challenges in surgical dissection. These adhesions increase the risk of intraoperative bleeding and injury of structures and vessels in the process of dissection [12]. Moreover, in the patients who had been suffering from complications after previous gastrectomy, the adhesions may be even more severe than expected. Therefore, very meticulous adhesiolysis and dissection are especially important in the secondary PD.
Secondly, it is difficult to perform fine LND and to retrieve a sufficient number of LNs in the secondary PD. In cases of operations for gastric cancer, the LNs around the hepatoduodenal ligament (D1+ LND) and the common hepatic artery (D2 LND) are routinely removed. This previous LND in these regions causes adhesions and fibrosis around the structures. The LND becomes very hard occasionally leading to incomplete LND, and distinguishing fibrotic tissues and lymphatic tissues becomes difficult. In this study, the mean number of retrieved LNs in the gastrectomy group was 8.9, comparable to the results of previous studies [22]. It should be noted that the mean number of retrieved LN was significantly lower in patients with a history of previous gastrectomy in the overall analysis, although it did not show statistical differences after PSM analysis. Also, although statistical significance was not reached, the absolute number of retrieved LN was lower in patients with a history of previous gastrectomy (8.9 vs. 12.5), even in PSM analysis. This may reflect how much more effort needs to be asserted in patients with a history of previous gastrectomy to perform comparable LND with those without a history of gastrectomy, even considering that some LND was performed in the previous surgery.
Thirdly, the altered anatomy of the alimentary tract due to previous gastric surgery makes anastomoses in secondary PD more difficult. The surgeon should recognize what type of gastrectomy was performed previously and carefully plan how the new anastomoses and reconstructions should be done. In our institution, Child method is routinely used for reconstruction, in which P-J is done at the most proximal of the jejunal stump, followed by C-J approximately 10 to 15 cm distal to P-J site, and G-J or duodenojejunostomy most distally (about 50 cm distal from C-J) [18]. Reconstruction in STG BI is not very complicated, and similar routine anastomosis could be performed once dissection and adhesiolysis are successfully completed. More complicated reconstruction is needed for the patients who underwent either STG BII or TG than those who underwent STG BI. In both STG BII and TG, bowel continuity is altered and the adhesions around the previous bowel anastomosis may interfere with the dissection and new reconstruction [23]. However, our experience demonstrates that it is all possible with careful dissection and planning. Although, a previous study reported some cases of postoperative afferent loop syndrome due to kinking of the small bowel, none of the patients in our study experienced such complications.
Finally, extending on the challenges inflicted by adhesion, the problems with adhesion are not only limited to the operation field of PD but applies to the whole length of the bowel. Every inch of small intestine is important. Perforations or small intestine segmental ischemia during adhesiolysis or dissection may make the planned reconstruction impossible if caused on a critical area. The surgeon may have to alter the plan and improvise with whatever remains available. This may lead to possible postoperative complications such as leakage or perforations. If very unfortunate, reconstruction may not be at all possible. To avoid unnecessary bowel injury, entire bowel evaluation should not be insisted on if there are severe adhesions, as long as bowel continuity can be inferred.
Through this analysis, we found that secondary PD after previous gastrectomy is characterized by lower preoperative BMI, higher EBL and rate of transfusion compared to conventional PD. After PSM analysis, there were no significant differences in postoperative complications (Clavien-Dindo classification ≥ III) according to the presence of history of prior gastrectomy. The operation time, frequency of clinically relevant POPF, and duration of postoperative hospital stay were also comparable in the 2 groups.
Current study is limited due to its retrospective nature; however, the nature of the population makes a prospective design difficult, and compensation for the shortcomings of retrospective PSM analysis was additionally performed. Another limitation may be the focus on the surgical techniques and short-term surgical outcomes and no long-term results.
In summary, performing secondary PD in patients with a history of gastrectomy is more likely to have bleeding or transfusion; however, there are no significant differences in the actual quality of surgery, postoperative course, and short-term clinical outcomes. Multicenter studies with a larger population are needed in the future to evaluate the oncologic outcomes and establish proper treatment guidelines for patients who require secondary PD after previous gastrectomy.
In conclusion, this study showed that patients who underwent PD after gastrectomy had a lower preoperative BMI, greater blood loss during surgery, and higher transfusion rates than those who underwent conventional PD. However, there were no differences in postoperative clinical courses, including complication rates, clinically relevant POPF and delayed gastric emptying, and hospital stay. This demonstrates that secondary PD after previous gastrectomy is safe and feasible when performed by experienced surgeons, but requires high caution and meticulous skills.
Go to :
 XML Download
XML Download