

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Choledochal cyst (CC) is a congenital malformation in which cystic dilatation of the biliary tree occurs. In Europe and the United States, 5–15 out of 1 million cases have been observed [1], but in Asian countries such as China, Korea, and Japan, approximately 1,000 out of 10 million cases are observed [23]. It is more frequently observed in females, with a female-to-male ratio of 3:1 [4]. Although the cause of CC occurrence is not clearly stated, anomalous pancreaticobiliary duct union (APBDU) can be considered as one of the causes of occurrence [5]. In patients with APBDU, the biliary and pancreatic ducts meet outside the duodenal wall, and the sphincter of Oddi fails to function, resulting in reflux of the pancreatic enzyme into the biliary tree. Digestive enzymes cause biliary dilatation, and long-term dysplasia can lead to cancer [3].
Unlike in children, CC is often asymptomatic in adults [46]. There are many cases of incidental findings due to the development of radiology [78]. Although CC is a rare and benign lesion, it can progress to biliary tract cancer [491011]. Therefore, surgery can be performed even in the absence of symptoms [12]. However, due to the low incidence of CC, a comprehensive analysis of patients with malignancy is insufficient [1314].
The treatment of CC includes biliary diversion through CC excision and hepaticojejunostomy formation. Recently, minimally invasive surgery (MIS), including laparoscopic and robotic approaches, has been performed [15161718]. Due to the nature of biliary tract surgery, the probability of complications is high, and if it occurs, the sequelae may be severe [4192021]. However, since most patients are reported to have benign lesions, the follow-up period is shorter than that of patients with malignancy, making it difficult to determine long-term clinical outcomes [16].
Therefore, this study aimed to compare the clinical characteristics of patients with malignant and benign CCs and to investigate the long-term outcomes of patients undergoing surgery for CC.
Go to : 
METHODS
Patients
Patients who underwent surgery for CC at Seoul National University Hospital between 2003 and 2020 were selected for the study. All patients aged 19 years or older were included. Patients who were unavailable for the preoperative imaging studies were excluded. Clinicopathologic factors and pre-/postoperative CT or magnetic resonance imaging were reviewed. The Institutional Review Board of Seoul National University Hospital approved all data collection, storage, and analysis (No. H-2104-092-1211). This study was performed in accordance with the Declaration of Helsinki and written informed consent was waived due to its retrospective nature.
Data collection
The patients’ medical records were reviewed for sex, age, body mass index, chief complaint, American Society of Anesthesiologists physical status classification, preoperative serum CEA, preoperative serum CA 19-9, preoperative serum bilirubin, operation, method, operative time, estimated blood loss (EBL), postoperative stay day, acute complications (within 30 days), final cyst pathology, and gallbladder (GB) pathology.
All contrast-enhanced CT or magnetic resonance cholangiopancreatography and endoscopic retrograde cholangiopancreatography were reviewed before surgery, including the Todani classification, APBDU, and cyst length and diameter. For cholangiography, cyst length was added to each segment for portions with biliary tract dilatation. After the operation, contrast-enhanced CT was followed up and reviewed to confirm the postoperative proximal bile duct diameter and postoperative distal bile duct diameter on postoperative day (POD) 4 or 5. After presuming the location of the resection on POD 4 or 5 CT, the size was measured on preoperative CT.
In the final pathology results, cyst high-grade dysplasia (HGD), cyst adenocarcinoma (ADC), and associated gallbladder cancer (GBC) were classified into the malignancy group, and the malignancy and benign groups were compared. Delayed complications were defined as cases of Clavien-Dindo (CD) classification grade III or higher, usually at the second outpatient visit after discharge, 3 months postoperatively.
Statistical analysis
Statistical analysis was performed using the Pearson chi-square test and the Fischer exact test for categorical data and the Student t-test for continuous data using IBM SPSS Statistics ver. 25.0 for Windows (IBM, Armonk, New York, USA). Statistical significance was set at P < 0.05.
Go to :
RESULTS
Demographics and type of CC
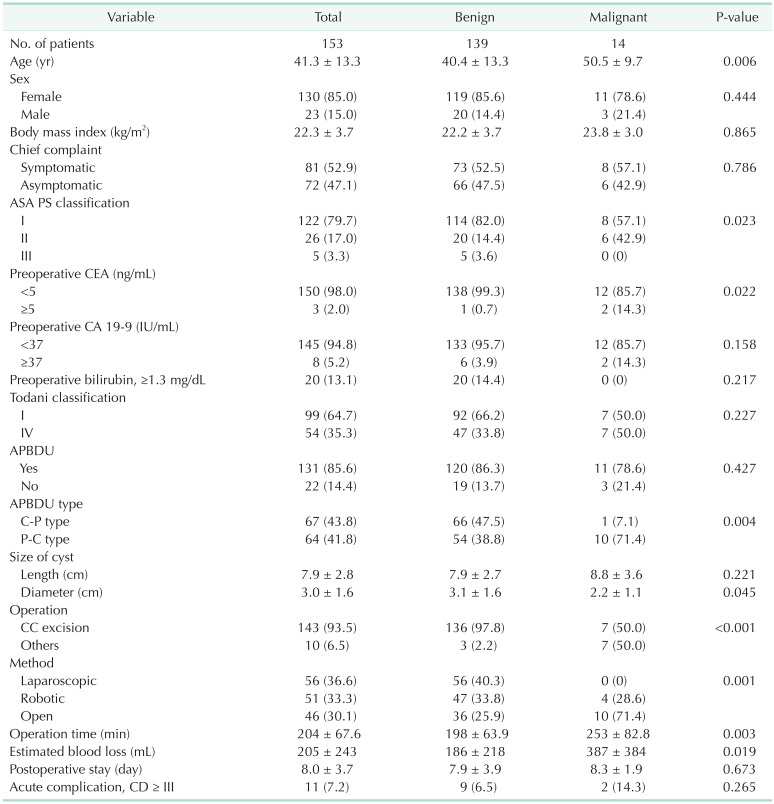
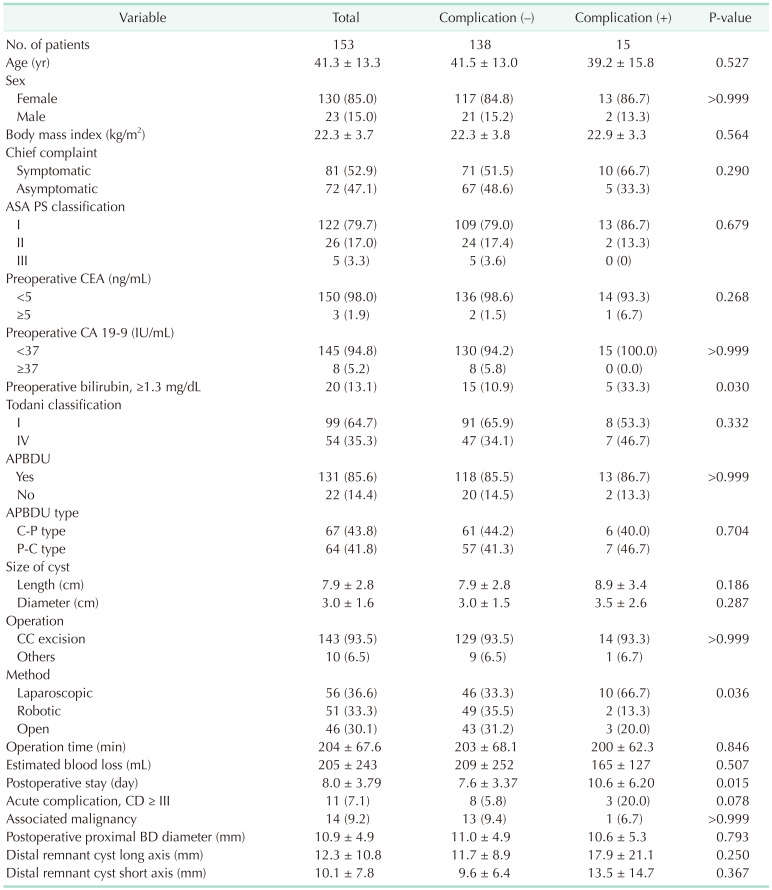
Between 2003 and 2020, 153 patients who underwent surgery for CC at Seoul National University Hospital were included in the study, and 1 patient whose preoperative image was not available was excluded. The mean patient age was 41.3 years, and 130 patients (85.0%) were female. Of 153 patients, 81 (52.9%) complained of symptoms, and the most common chief complaint was abdominal pain. The median preoperative CEA and preoperative CA 19-9 levels were 1.2 ng/mL and 8.3 IU/mL, respectively. Twenty patients (13.1%) had preoperative bilirubin levels above 1.3 mg/dL. According to the Todani classification, 64.7% and 35.3% were types I and IV, respectively, and the most common subtype was Ic (36.6%). There were no types II, III, and V. The presence and absence of APBDU and subtype were also checked, and C-P and P-C type and no APBDU were 43.8%, 41.8%, and 14.4%, respectively. The length and diameter of CC were also checked, and their means were 7.9 and 3.0 cm, respectively (Table 1).
Operation and clinical course of patients with CC
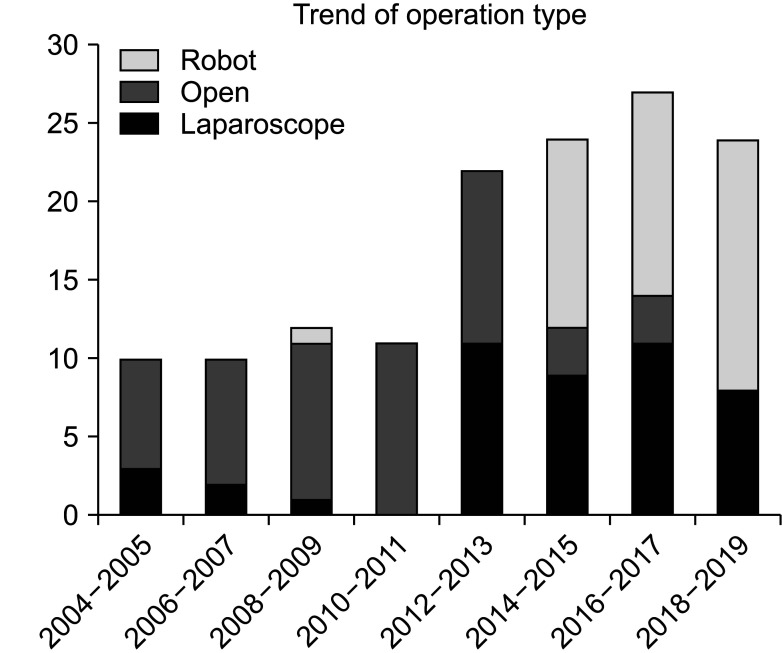
CC excision was performed in 143 patients (93.5%). In addition to CC excision, various surgeries were performed in 10 patients. Eight patients underwent additional wedge resection of the liver at the GB bed because GBC was suspected on preoperative imaging. One patient who had left hepatic duct stricture intraoperatively underwent left hemihepatectomy, and in the last patient, periampullary cancer was observed on preoperative imaging, and pylorus-preserving pancreaticoduodenectomy (PPPD) was performed. Of the cases of patients suspected of GBC, only 5 were confirmed pathologic, and stages 1 (n = 1), 2 (n = 3), and 3 (n = 1) were observed, and 2 of them recurred after 35 and 121 months, respectively. The surgical approach was observed with a laparoscopic approach (36.6%), robotic approach (33.3%), and open method (30.1%). Over time, the MIS rate increased (Fig. 1). The average operation time was 204 minutes, and the average EBL was 205 mL. There were 11 patients with complications of CD classification grade III or higher within 30 days after surgery. Bile leak (n = 4), ileus (n = 3), bleeding (n = 2), fluid collection (n= 1), pancreatitis (n = 1), and aspiration pneumonia (n = 1) were observed. In 1 patient, postoperative aspiration pneumonia and bleeding were observed together (Table 1).
Pathology and comparison of clinicopathologic data according to combined malignancy
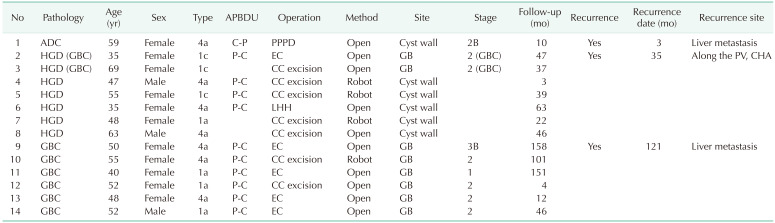
In the final pathology results, cancer was observed in 14 patients. Distal bile duct ADC (n = 1), bile duct HGD (n = 5), and GBC (n = 6) were observed. In 2 patients, bile duct HGD and GBC were observed together.
Patients with benign and malignant CCs were compared, and age (40.4 years vs. 50.5 years, P = 0.006), preoperative CEA of ≥5 (0.7% vs. 14.3%, P = 0.022), operation time (198 minutes vs.. 253 minutes, P = 0.003), and EBL (186 mL vs. 387 mL, P = 0.019) were significantly higher in patients with malignancy. The cyst diameter (3.1 mm vs. 2.2 mm, P = 0.045) was significantly smaller in patients with malignancy. There was no statistical difference when compared according to the presence or absence of APBDU (13.7% vs. 21.4%, P = 0.427), but when compared by type, the P-C type was 15.6% (10 of 64) and the C-P type 1.5% (1 of 67) was observed in patients with malignancy, respectively. The P-C type was observed to be significantly higher in patients with malignancy (P = 0.004). There were more cases of combined surgery other than CC excision in patients with malignancy (2.2% vs. 50%, P < 0.001). The open approach (25.9% vs. 71.4%, P = 0.001) was higher in patients with malignancy (Table 1).
Clinical course of patients with malignancy
In 1 patient with common bile duct (CBD) cancer, the stage was observed to be 2B, and 8 patients with GBC had stages 1 (n = 1), 2 (n = 6), and 3 (n = 1). The follow-up range was 3–158 months, and the median was 42.5 months. Recurrence was observed in one patient with CBD cancer and 2 patients with GBC. In a patient with CBD cancer, liver metastasis was observed 3 months after surgery, and 1 patient with GBC and CBD HGD had metastasis around the portal vein and common hepatic artery (CHA) 35 months after surgery, and the other patients with GBC had metastasis at the liver 121 months after surgery (Table 2).
Clinical characteristics of patients experiencing delayed complications
Outpatient follow-up was continued after surgery, and the maximum follow-up duration was 186 months and the average follow-up duration was 46.2 months. CT was followed up on postoperative day 4 for all patients, and the mean proximal bile duct diameter was 10.9 mm. The distal remnant cyst of the intrapancreatic portion was observed in 91 patients (59.5%), and the means of the long and short axes of the distal remnant cyst were 12.3 and 10.1 mm, respectively. It was also confirmed that delayed complication occurred 3 months after surgery. Delayed complications were observed in 15 patients (9.8%). Cholangitis in 9 patients (60.0%), ileus in 2 patients (13.3%), liver abscess in 2 patients (13.3%), pancreatitis in 1 patient (6.7%), and remnant intrapancreatic cyst infection in 1 patient (6.7%). The complication timing range was 3–159 months, and the median was 30.0 months. Seven patients (46.7%) were improved by conservative treatments, but 4 patients (26.7%) underwent intervention due to ascending cholangitis or remnant intrapancreatic cyst infection, and 4 patients (26.7%) underwent reoperation.
One patient developed a new cancer around the distal remnant cyst. This patient had pancreatic head cancer 39 months later, and the patient underwent PPPD (Fig. 2).
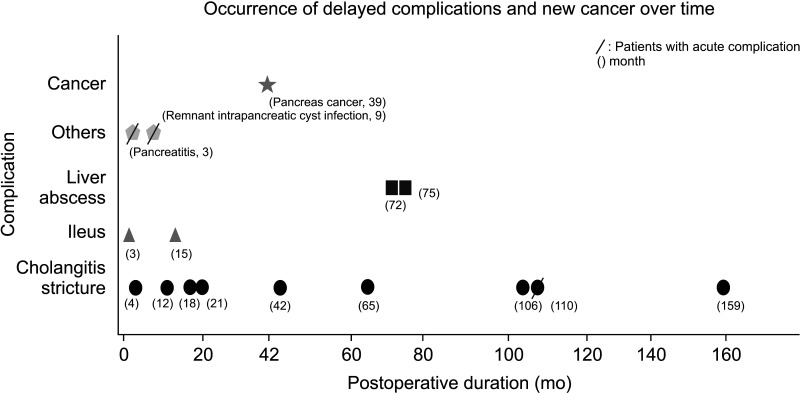 | Fig. 2Delayed complications are observed in 15 patients (9.8%), cholangitis in 9 patients (60.0%), ileus in 2 patients (13.3%), liver abscess in 2 patients (13.3%), pancreatitis in 1 patient (6.7%), and cyst infection in 1 patient (6.7%). The patients with acute complications are marked with slashes. The complication timing range is 3–159 months, and the median is 30.0 months. One patient developed a new cancer around the distal remnant cyst. The patient had pancreatic head cancer 39 months later.
|
Based on comparisons according to the presence or absence of delayed complications, high preoperative serum bilirubin level over 1.3 mg/dL (33.3% vs. 10.9%, P = 0.030) and laparoscopic approach (66.7% vs. 33.3%, P = 0.036) were significantly higher in patients who suffered from delayed complication. Preoperative imaging, postoperative imaging, and malignancy were not associated with delayed complications (Table 3). We compared 9 patients with biliary stricture with the rest of the patients. The ratio of surgical approach, open method, laparoscopic approach and robotic approach was 29.9% (n = 43), 34.7% (n = 50), 35.4% (n = 51), respectively, among patients without biliary strictures. Meanwhile, the ratio of open method, laparoscopic approach and robotic approach was 33.3% (n = 3), 66.7% (n = 6), 0% (n = 0), respectively, among patients with biliary strictures, which tended to cause biliary stricture in laparoscopic surgery (P = 0.061). Hepaticojejunostomy revision was performed in 2 cases.
Go to :
DISCUSSION
Because CC is a congenital disease, there are many reports in children, but studies on adult CC have mostly been small-scale studies, and there are no reports of long-term outcomes [121518]. In our study, preoperative and postoperative images and pathology were comprehensively analyzed in 153 patients, and long-term outcomes were analyzed through a sufficient follow-up period. In patients with malignancy, P-C type APBDU was observed more frequently, and the cyst diameter was often smaller. Delayed complications were observed more frequently in patients with acute complications of CD classification grade 3 or higher.
There are differences in the clinical characteristics of CC between adults and children. Abdominal pain is more common in adults, and jaundice is more common in children [4622]. Preoperative interventions were more commonly performed in adults, including endoscopic retrograde pancreatography, percutaneous transhepatic cholangiography, and endobiliary stenting. Postoperative complications were significantly higher in adults than in children [422]. The frequency of the Todani classification types in adults and children is controversial [4610]. In most studies, biliary tract malignancy was not observed in children, but embryonal rhabdomyosarcoma was observed in some cases [422]. In our study, abdominal pain was the most common symptom among symptomatic CCs, and Todani classification Ic and C-P type APBDU were the most common in adult CC.
The proportion of biliary tract malignancy associated with CC in adults is known to be 4%–19% and tends to increase with age [1011]. In our study, the proportion of malignancies including HGD was only 9.2%. The cancer incidence was 1,000–2,000 times higher in patients with CC than in the general population, and the proportions of GBC, bile duct cancer, and periampullary cancer were observed in different studies [722]. APBDU is known as a risk factor for GBC, and continuous efforts are being made to apply better surgical methods to patients by further subdividing the types of APBDU, such as suggesting new Komi classification [2324]. According to previous studies, combined malignancy was related to the Todani classification, but in our study, it was related to P-C type APBDU. There were also reports that cyst diameter was related to malignancy, but in our study, the diameter was smaller in patients with malignancy [11]. These results imply that the undilated CC is not reassuring for malignancy. In general, there are reports that cancer is caused by several mechanisms in CC, and that cancer incidence differs depending on morphological characteristics. In particular, although studies on the occurrence and types of cancer according to the APBDU type are very scarce, it is a finding consistent with several reports that the PC type has less biliary duct dilatation, and that less biliary duct cancer has a higher incidence of biliary tract cancer. Although the cause is not known, Tashiro et al. [25] have already indicated that the incidence of biliary tract cancer is higher in the absence of bile duct dilatation. The study on the cause of oncogenesis for APBDU type will be needed in the future.
The incidence of acute complications is high compared with other benign diseases, and long-term follow-up data are needed because there is a high possibility of leaving long-term sequelae if complications occur. However, since most pathological results are reported to be benign, the follow-up duration is short, so research on this is insufficient. In this study, late complications were observed only in 9.8% (n = 15) of patients; 46.7% were improved by conservative treatments, but 26.7% (n = 4) underwent intervention due to ascending cholangitis or remnant intrapancreatic cyst infection, and 26.7% (n = 4) underwent reoperation. Two patients underwent hepaticojejunostomy revision due to anastomosis site stricture at 3 years and 6 months and 7 years after surgery, respectively. One patient underwent distal pancreatectomy at 3 months postoperatively due to recurrent pancreatitis, and the other patient underwent laparoscopic gastrojejunostomy due to duodenal stenosis at 3 months after surgery.
According to other studies, the probability of developing new cancers such as pancreatic ADC and cholangiocarcinoma during the outpatient follow-up period after surgery was 0%–4.25% and 8–32 years after surgery [41213]. In this study, only 0.7% of patients (n = 1) had new periampullary cancer in distal remnant cysts within 3 years. There is a difference from previous reports, but continuous follow-up is necessary due to the possibility of developing new malignancies.
We already know that the robotic approach has significantly fewer acute complications and biliary tract complications than the laparoscopic approach [26]. In this study, the use of robotic surgery increased over time, and the postoperative complication rate in the robotic approach group was significantly lower than that in the laparoscopic approach and open method groups due to the security of robotic anastomosis. We compared 9 patients with biliary stricture with the rest of the patients. Biliary stricture occurred at a higher rate in the laparoscopic approach, whereas there were no patients who exhibited biliary stricture in robotic approach. It has been approximately 10 years since robotic surgery was introduced in patients with CC, and there is still only research on short-term and mid-term results, so longterm follow-up is required [1527].
Our study has several limitations. First, a prospectively collected database was used; however, the study had a fundamental limitation of being a retrospective study in a single center. Second, the registration period was long; thus, there may be differences in the operation and perioperative management. Third, since CC is a benign disease, there are several cases in which periodic outpatient follow-up was not well performed, and cases with follow-up loss were also observed.
In conclusion, 9.2% of resected CCs had combined malignancy in the biliary tracts, and the proportion of malignancy was higher in patients with P-C type APBDU and short cyst diameter. Therefore, a thorough imaging examination is required before surgery. Since late complications are common in patients with acute complications, careful management of patients in the immediate postoperative period is required.
Go to :
 XML Download
XML Download