

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The prevalence of peripheral artery disease (PAD) of the lower extremities is currently 4.3% and has been increasing gradually in all countries [1]. One subset of PAD is aortoiliac occlusive diseases (AIOD). AIOD is the term for all arterial lesions between the infrarenal distal aorta and common femoral artery (CFA). These lesions are classified in the Inter- Society Consensus for the Management of Peripheral Arterial Disease (Trans-Atlantic Inter-Society Consensus [TASC] II) [2]. AIOD accompanied by severe claudication (SC) or critical limb ischemia (CLI) should be treated according to TASC II recommendations. AIOD involving the aortic bifurcation remains challenging. It can be treated with open surgery (OS), endovascular therapy (ET), or in a hybrid manner. While interventions for infrainguinal disease are now common, ET of AIOD has been avoided by experts for a long time. However, these interventions are now being performed more frequently [234]. Implantation of kissing stents (KS) with covered stents (CS), bare-metal stents (BMS), or self-expandable nitinol stents, covered endovascular reconstruction of aortic bifurcation (CERAB), and endovascular aortic repair are ET modalities for AIOD involving the aortic bifurcation. KS treatment has emerged as an intervention technique for difficult lesions in AIOD [5]. Although there is not enough data to use this intervention as a routine technique, studies show that the KS technique has several benefits over OS, including shorter length of hospital stay, lower 30-day mortality and major morbidity, and comparable short-term outcome [67]. In this study, we report the outcomes of the KS technique in infrarenal AIOD.
Go to : 
METHODS
Study design
The study is designed as a retrospective single-center trial. Between January 2014 and September 2017, 375 patients with a diagnosis of AIOD underwent invasive treatment. This study was approved by the Institution Review Board of Tepecik Training and Research Hospital in Izmir, Turkey (No. 2019/16-24). Patient consent was waived due to the retrospective nature of the study. Electronic medical records were reviewed for patient demographics, vascular disease risk factors, procedural information, and clinical and imaging follow-up. The clinical status of patients was assessed with the Rutherford classification. The inclusion criterion of this study was being treated by KS technique due to AIOD. Indications to perform KS procedure in our practice were symptoms of SC (Rutherford category 3) or CLI (Rutherford category 4 or higher) due to AIOD, and ET was the first option to treat these patients. In this study, the patients treated with these indications included 31 patients with bilateral proximal iliac lesions, some of which had also distal aortic involvement. In the aforementioned time frame, the only situation that KS procedure was avoided was severe renal disease, which also set off the only exclusion criteria. Patients with previous endovascular or surgical treatment of the common iliac artery and patients admitted with acute limb ischemia and severe renal failure (e-GFR < 30 mL/min/1.73 m2) were excluded. However, patients with end-stage renal failure who are on a routine dialysis program were included. Patients were directed from the outpatient clinic for elective operations unless they had CLI. Patients with CLI were scheduled for urgent intervention. Lesions were classified according to TASC II guidelines. All patients who underwent ET were treated with KS technique either with balloon-expandable BMS or balloon-expandable CS.
Stents and procedures
In all patients, preoperative imaging was started with Duplex ultrasound (DUS). For patients with positive findings in DUS, further imaging was performed with computed tomography angiogram (CTA). Calcium score was detected with CTA and defined as none, mild, moderate, or severe. Calcifications of the lesions were classified based on their extension through the length of total lesion and degree in circumference. It was considered mild when calcium deposits extend lesser than 50% of the total length of the lesion and 180° in circumference, severe when calcium deposits cover more than 180° in circumference and extend more than 50% of the total length, and moderate in all other degrees of calcification. All procedures were performed in the interventional angiography laboratory (Siemens AXIOM Artis dTA, Siemens Healthcare, Erlangen, Germany). Procedures were performed percutaneously under local anesthesia. General anesthesia was not utilized for any patient. Percutaneous endovascular access was obtained under ultrasound guidance via bilateral retrograde CFA punctures using the Seldinger technique. Depending on stent sizes, 6 or 7 French vascular sheaths were inserted. Intraarterial 100 units/kg heparinization was applied. The intimal tracking approach was used. ZIPwire 0.035-inch hydrophilic guidewire (ZIPwire, Boston Scientific, Natick, MA, USA), and CTO guidewire and support catheters (Navicross, Terumo, Somerset, NJ, USA; or Rubicon35, Boston Scientific) were used to cross lesions. A pigtail catheter was advanced proximal to the aortic lesion, and digital subtraction angiogram was performed via power injector. Stent length and diameter characteristics were determined based on lesion length and diameter of the adjacent normal vessel using a vascular analysis measurement program on the angiography device (Siemens AXIOM Artis dTA). In cases of total chronic occlusion or near occlusion, predilatation was performed only to facilitate stent delivery. The delivery system was positioned approximately 5 mm above the lesion in order to cover the stenotic or occluded segment. Stent size selection was determined by the diameter of the healthy section of the common iliac artery and distal aorta. If combined stent diameter was greater than the diameter of the distal aorta, smaller diameter stents were deployed. Balloon-expandable BMS (Visi-Pro, Medtronic, Dublin, Ireland) or balloon-expandable CS (Advanta V12, Atrium Medical Inc., Hudson, NH, USA) were simultaneously deployed. Stent choice was left to the discretion of the treating physician. Calcium scores played a more major role in this decision than TASC II classification. Another important factor was the patency of internal iliac artery. The aim was to leave at least 1 patent internal iliac artery. When contralateral internal iliac artery was patent, calcium score gained prominence and CS was used in cases of high calcium scores. When contralateral iliac artery is diseased and the calcium score of the target lesion was high, ipsilateral internal iliac artery was spared by using BMS. Poststenting angiography was routinely performed to confirm stent and runoff patency, and to rule out extravasation. The angiographic procedure of 2 separate cases is shown in Fig. 1. Technical success was defined as successful vascular access, ET completion, and absence of residual diameter reduction over 30% on completion angiography [8]. A closure device was used in all patients (Angioseal, Terumo).
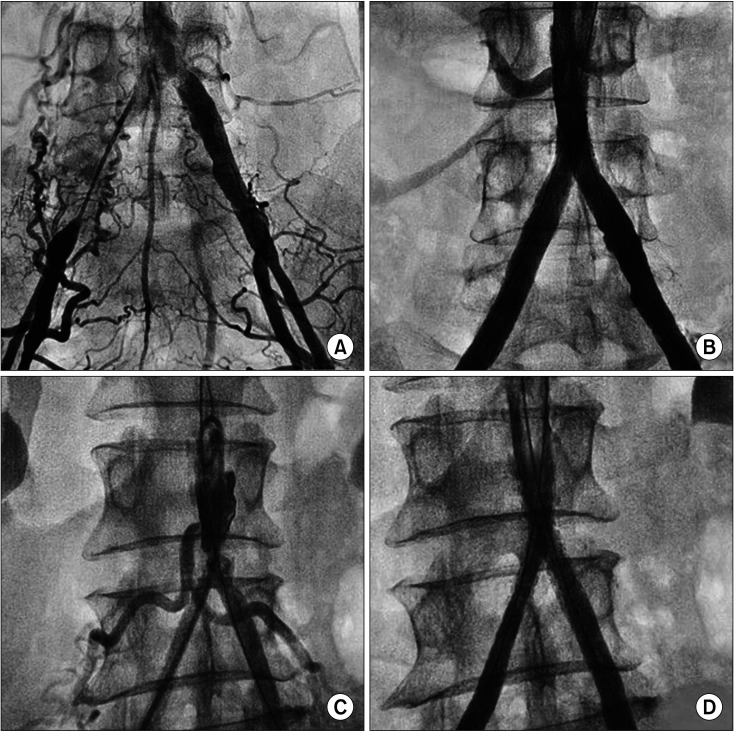 | Fig. 1(A) Initial anteroposterior image from angiogram shows chronic total occlusion of the right common iliac artery, including its origin and near occlusion of the proximal of the left common iliac artery. (B) Ultimate angiogram shows the treatment with kissing stents (KS) technique of the lesions. (C) Initial anteroposterior image from angiogram shows severe infrarenal aortic stenosis involving bilateral common iliac arteries. (D) Ultimate angiogram shows the treatment with KS technique of the lesions.
|
Medical therapy
All patients were immediately placed on postoperative dual antiplatelet therapy that included a 300-mg loading dose of clopidogrel and 100 mg of acetylsalicylic acid (ASA). All cases were performed with broad-spectrum antibiotic prophylaxis given during the hospital stay. Dual antiplatelet therapy was continued indefinitely after stenting with a daily clopidogrel dose of 75 mg and ASA dose of 100 mg.
Study endpoints
The primary endpoint was primary patency, which was defined as uninterrupted patency after the index procedure without reintervention on the treated segment during follow-up. Secondary endpoints were secondary patency, technical success, complications, and survival. Technical success was defined as patency shown in control angiogram after stent deployment in the index procedure. Secondary patency was defined as patency of the treated segment following a reintervention to maintain patency during follow-up. Restenosis was defined as greater than 30% diameter reduction on angiogram of treated lesion in patients who presented with claudication. Follow-up of stent patency was based on clinical and radiological assessments. Patients were routinely followed up by aortoiliac DUS at 3, 6, 12, 18, and 24 months after intervention. If significant stenosis was detected with DUS, further imaging was performed with CTA.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Mac ver. 20 (IBM Corp., Armonk, NY, USA). Numeric variables were summarized as mean ± standard deviation values and median (range) values. Categorical variables were evaluated by cross-tabulation analysis and shown numerically with percentages. The Student t-test was used for normally distributed data measured on a continuous/interval scale, while the Mann-Whitney U-test was used for non-normally distributed data. Pearson correlation test was used to measure the statistical relationship or association between continuous variables. Stent patency was analyzed by using survival analysis with Kaplan-Meier log-rank test. A P-value less than 0.05 was considered indicative of a statistically significant difference.
Go to :
RESULTS
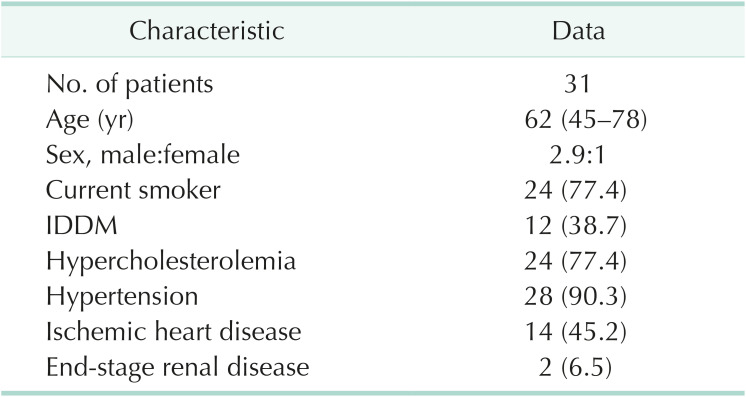
The majority of patients was male (77.4%), and median age was 62 years (range, 45–78 years). All patients were symptomatic. The patients’ characteristics and risk factors are summarized in Table 1.
All patients were classified according to TASC II criteria. Eight patients (25.8%) were classified as TASC B. Fifteen patients (48.4%) were classified as TASC C, and 8 patients (25.8%) were classified as TASC D. These 23 patients with TASC C or D lesion were classified as complex AIOD group. Preprocedural and procedural details are summarized in Table 2.
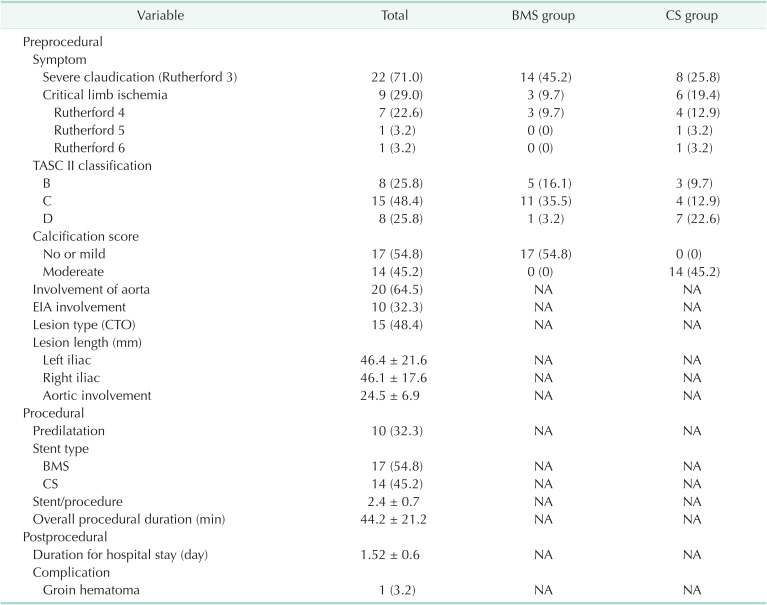
Twenty-two patients (71.0%) had SC (Rutherford 3) and 9 patients (29.0%) had CLI on admission. In the CLI group, 7 patients had Rutherford 4, 1 had Rutherford 5, and 1 had Rutherford 6 symptoms. Compared to the group with TASC B lesions, CLI was seen more frequently in the complex AIOD group (P = 0.040). Seventeen patients (54.8%) h ad at least mild calcification, whereas 14 patients (45.2%) had moderate calcification (TASC B, 3 patients; complex AIOD, 11 patients). No severe calcification was detected.
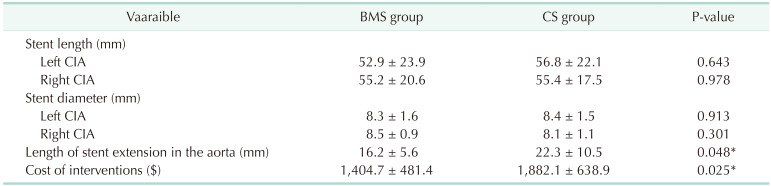
Bilateral retrograde CFA approach was successfully performed in all patients, and antegrade approach via upper extremity was not necessary for any patient. Predilatation with plain old balloon angioplasty (POBA) was performed in 10 patients (32.3%), and all belonged to the complex AIOD group. BMS was used in 17 patients (54.8%), and CS was used in 14 patients (45.2%). Five patients in the TASC B group were treated with BMS, and 3 patients were treated with CS. Twelve patients with complex AIOD were treated with BMS while 11 patients were treated with CS. Although there were no significant differences between patients treated with BMS and CS in terms of total stent length, left and right CIA stent diameters, and mean total stent diameter for aorta (P = 0.643, P = 0.978, P = 0.913, P = 0.300, P = 0.715), mean length of stent extension in the aorta was significantly longer in patients treated with CS (BMS, 16.2 ± 5.6 and CS, 22.3 ± 10.5; P = 0.048) (Table 3).
The mean procedural duration was 44.2 ± 21.2 minutes. The procedural duration was 32.1 ± 4.9 minutes for TASC B lesions and 48.3 ± 23.1 minutes for complex AIOD (P < 0.001). Technical and clinical success was achieved in 100% of treated cases. There were no periprocedural complications. One postprocedural complication (3.2%) was reported among the cohort. The patient was discharged and readmitted with a 3 × 4-cm groin hematoma. The groin hematoma did not have pseudoaneurysm formation and was managed conservatively. The patient was discharged the day after readmission. A comparison of lesion types in terms of periprocedural features was shown in Table 4.

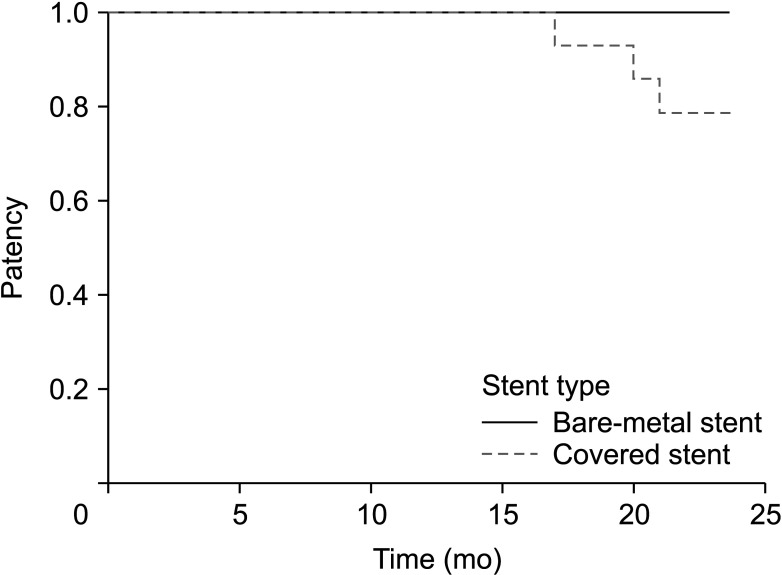
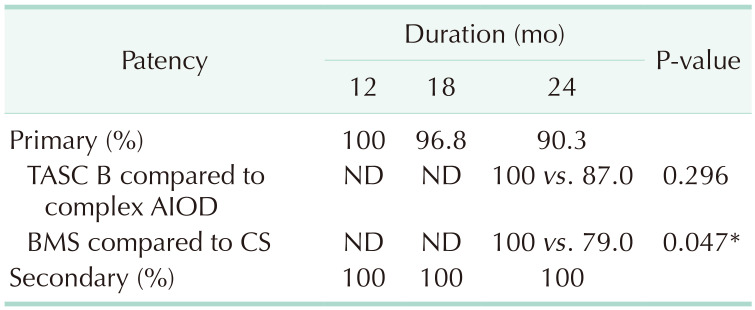
The median follow-up was 24 months (24–34 months). Primary and secondary patency are shown in Table 5. The overall primary patency rates at 12, 18, and 24 months after ET were 100%, 96.8%, and 90.3%, respectively, while the secondary patency rate at 24 months was 100%. Subgroup analysis showed 100% primary patency in the TASC B group at 24 months while rates in the complex AIOD group at 12, 18, and 24 months were 100%, 95.7%, and 87%, respectively (P = 0.296). During follow-up, significant unilateral in-stent restenosis was observed in 3 patients (9.7%). All patients had TASC II D lesions with moderate calcification and were treated with CS (P < 0.001). In all of these cases, severe stenoses were in the aortic edge of the stents. Subgroup analysis showed better primary patency for BMS than CS (100% vs. 79%, P = 0.047) (Fig. 2). There were no significant differences between stent diameters or stent lengths of patients with and without reintervention (P = 0.28, P = 0.990). However, 3 patients treated with CS who required reintervention had the longest extension above the aortic bifurcation. Mean length of extension for these patients was 3.7 ± 0.6 cm (P = 0.02). All restenoses were treated percutaneously with POBA and OS was not needed during follow-up.
Major amputation was performed in 1 patient (3.2%). The patient was initially admitted with Rutherford 6 forefoot wound with osteomyelitis and required a below-knee major amputation 2 weeks after the intervention.
The mean duration of hospital stay was 1.52 ± 0.6 days, and subgroup analysis revealed no significant differences between TASC B (1.38 ± 0.5 days) and complex AIOD (1.57 ± 0.6 days) groups (P = 0.47). Mean total cost for interventions were $1,213.8 ± $717.2 for the TASC B group and $1,666.12 ± 489.1 dollars for the complex AIOD group (P = 0.130). However, comparison of mean total cost between patients treated with BMS and CS revealed significant differences (BMS, 1,275.0 ± 348.5 and CS, 1,882.1 ± 638.9; P = 0.002). No early or late mortality was detected during follow-up.
Go to :
DISCUSSION
The current study included 31 AIOD patients with symptoms of SC (Rutherford category 3) or CLI (Rutherford category 4 or higher) and proximal bilateral iliac lesions with or without distal infrarenal aortic stenosis being treated with KS. Although surgical reconstruction of these patients remains the gold standard and has up to 90% 5-year patency, mortality, perioperative systemic and local complications, and late graft-related complication rates are remarkable [29]. Furthermore, the gap between ET and OS outcomes seems to be closing. A meta-analysis conducted by Groot et al. [5] compared patency rates for KS; primary patency before 2005 was significantly lower than results obtained after 2005. This may be explained by improvements in endovascular techniques, equipment, and experience [10].
According to TASC II recommendations, ET is the treatment of choice for TASC A and B and focal or short lesions of AIOD. Nevertheless, recent studies state that KS technique may be an appropriate option even for TASC C and D lesions of AIOD [6111213]. There is still no consensus on the best ET and type of device. Due to reimbursement issues, only KS technique is a choice for ET in these lesions.
Studies report technical success rates for ET between 73% and 100% [1014]. Although most of our population consisted of patients with complex AIOD, we had a high technical success rate (100%) in KS. This outcome is because our center has a high volume of ET and good preprocedural evaluation. Preprocedural evaluation is vital. In our clinic, CTA was routinely performed to determine lesion characteristics, vascular measurements, and runoffs. This allows preparation with the necessary tools, such as CTO guidewires and support catheters.
In many studies, primary stenting showed superiority to POBA alone in AIOD due to elastic recoil in POBA alone [15161718]. In our series, primary stenting was mostly used. POBA was performed only for predilatation to facilitate stent delivery when necessary. However, debate remains on which stent type to use with KS to treat these lesions. Self-expanding nitinol stents have similar patency rates as balloon-expandable stents. However, the cost for these stents is higher than balloon expandable stents, and protective specifications against complications are weaker than those for CS [19].
One advantage of CS over BMS is its design to exclude plaque and form a new lumen. In contrast to BMS, CS ensures lumen gain, reduces flow disturbance, and prevents the stimulus for proliferation of inflammatory and vascular smooth muscle cells [14]. As a result, CS has the potential to decrease restenosis due to intimal hyperplasia and provides longer patency rates [2021]. Sabri et al. [21] reported superior primary patency for CS compared to BMS (92% vs. 72%). However, CS is more expensive than BMS and larger profile sheaths are necessary for deployment. Mwipatayi et al. [22] claimed that because CS require larger delivery systems than BMS, the patient may have a higher risk of groin complications. They also concluded that crossing the long CTO with a larger delivery system creates difficulties and predilatation with balloon angioplasty is necessary for those lesions. In our trial, BMS was implanted only for patients with no or mild calcification, while all patients with moderate calcification were treated with CS to avoid periprocedural complications. Most patients in the TASC B group were treated with BMS while most patients with complex AIOD were treated with CS.
Subgroup analysis showed better primary patency rates and successful avoidance of complications for BMS. However, this result may be related to crossing the KS over the aortic bifurcation rather than stent type. Three patients treated with CS required reintervention during follow-up, and the mean length of extension for these patients was significantly longer. Although some studies claim that extension of KS over the aortic bifurcation had no effect on stent patency [523], the BRAVISSIMO trial showed that the use of KS extending into the aortic bifurcation was an independent predictor of lower primary patency [24]. Extension may lead to flow disturbance and wall shear stress to result in increased risk of thrombus [25]. In another trial, the cutoff value was specified as 20 mm. Our average aortic stent extension length was longer than 20 mm in patients treated with CS (22.3 ± 10.5 mm). This may also influence patency rates in the CS group [26]. It should be noted that extension length is not related to quality of intervention and cannot be adjusted. The main issue is whether extension length affects possible subsequent surgery. Piffaretti et al. [27] showed that ET as a first-line treatment does not affect the complexity of OS.
CERAB is another treatment option for AIOD. In one study in which 89% of lesions were TASC D, 3-year results of CERAB technique were examined. The primary patency rate was calculated as 83.9% at 24 months [28]. The CERAB study emphasized that excellent patency is related to flow dynamics, and coated stents probably play a role. In the COBEST durability trial [29], the first randomized controlled trial that compared CS to BMS in the management of AIOD, primary patency rate was 82.2% in 24 months in the CS group. This ratio is comparable with our study and to that of the CERAB trial [28].
The number of complex lesions (TASC C + D) was 23 (74%). This rate was higher than the most recent meta-analysis published by Groot et al. [5] in 2019, which is the largest group in the literature (8.1%). There was a tendency to use CS in more complex lesions in our trial. This may also have an effect on primary patency rates. However, no significant difference was found between patients with complex AIOD and TASC B in terms of primary patency (87% vs. 100%) [613]. Although our cohort included a high-risk group, overall 24-month primary and secondary patency rates were 90.3% and 100%, respectively.
The most important advantages of ET are low rates of major and minor complications and mortality [10]. Groin complications are the most common complications after KS. In our study, one patient had a groin hematoma that was treated conservatively [5]. Our low groin complication rates are probably related to the use of a vascular closure device, as shown in a recent review [30]. However, a meta-analysis conducted by Das et al. [31] revealed no significant difference between the use of closure devices and compression in terms of reduced complications. In our study, no periprocedural and postprocedural major complications were observed, including distal embolization and aortic rupture or dissection. Considering the complexity of aortic lesions, the tendency to use primary stenting might have minimized the risk of aortic rupture and dissection. In addition, none of our patients had severe calcification. BMS was implanted only for patients with no or mild calcification, while all patients with moderate calcification were treated with CS. These factors might also have resulted in our low complication rate.
Although complex AIOD lesions predicted worse secondary patency in a recent study, our secondary patency rate was 100% [23]. Three patients underwent reintervention, and all of these lesions were managed with POBA. The main reason for this is lesion detection at the stenosis stage. Close clinical follow-up is crucial to allow early uncomplicated intervention.
We did not find any significant differences between TASC groups in terms of mean costs. However, significant differences were detected between patients treated with BMS and CS. This result is not surprising, as CS is more expensive than BMS.
The limitations of our study are non-randomization, retrospective design, small sample size, and short follow-up.
In conclusion, we found that the KS technique has satisfying 24-month results, even in complex AIOD lesions, with successful technical success and low complication rates. Multicenter, randomized, controlled, and large studies are needed to produce comparable results with long-term surgical outcomes.
Go to :
 XML Download
XML Download