

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
As life expectancy increases, the number of patients aged 75 years and older is constantly increasing worldwide [1]. Meanwhile, opportunities to detect hepatocellular carcinoma (HCC) in elderly patients have dramatically increased due to the progress made in medical technology and healthcare services. In the past 2 decades, there have been many changes in the diagnosis and treatment of HCC [23]. The management of elderly HCC patients has become a global problem; accordingly, the need for surgical management in elderly HCC patients has grown and it is becoming increasingly important for clinicians to recognize and fully understand the clinical features and prognosis of HCC hepatectomy in elderly patients [45].
Elderly patients have more comorbidities, including cardiovascular and cerebrovascular disease, pulmonary disease, and renal disease than younger patients. Moreover, hepatic volume and hepatic blood flow have been shown to significantly decrease with age and the impairment of bile acid synthesis, Kupffer cell function, and liver regeneration occurs in aged livers [67]. Therefore, surgical liver resection (LR) is more difficult to perform and requires more attention to be successful in elderly patients than in younger patients.
There is still no general agreement on the definition of the elderly population. Previous studies have used 65 years of age as the cut-off for the definition of elderly, while a more recent study used 75 years as an age threshold [8]. Little is known about surgical operations in elderly HCC patients older than 75 years of age.
Laparoscopic surgery was introduced in 1987 and its widespread use has increased the number of elderly patients subjected to this surgical approach. The general trend has been a shift away from conventional surgical procedures toward the laparoscopic approach. Recently, laparoscopic LR (LLR) has been accepted as feasible in the elderly [910].
The purpose of this study was to compare the postoperative and long-term outcomes of elderly treatment-naïve solitary HCC patients (≥75 years) according to whether the operation occurred in the year 2016 and after or before 2016. In addition, we were to identify risk factors for HCC recurrence and patient death after curative LR in these patients.
METHODS
Patients
This study included elderly patients older than 75 years of age who underwent LR for solitary treatment-naïve HCC from November 1998 to March 2020 in Samsung Medical Center (Seoul, Korea). Hepatectomy patients were those with preoperative Child-Pugh class A who were diagnosed with HCC in pathology. Pathologically diagnosed combined HCC and intrahepatic cholangiocarcinoma, R1 resection, synchronous abdominal operation due to other malignant diseases, robotic LR, or open conversion cases during LLR due to uncontrolled bleeding were excluded. A total of 130 patients were identified, none of whom received adjuvant chemotherapy after curative LR before HCC recurrence. The procedures used for surveillance after LR have been described previously [11]. The present study was approved by the Institutional Review Board of Samsung Medical Center (No. 2020-12-155) and the requirement for written consent from study participants was waived. The study was conducted in accordance with the tenets of the Declaration of Helsinki.
Clinical data
Demographic, preoperative laboratory, pathologic data, and recurrence HCC data were collected prospectively from patient electronic medical records. The collected baseline characteristics were sex, age, and etiology for HCC. Preoperative laboratory findings included routine blood tests, liver function tests, alpha-fetoprotein (AFP) level, and levels of proteins induced by vitamin K absence or antagonist-II (PIVKA-II). Surgical factors included the American Society of Anesthesiologists (ASA) physical status classification, operative extent, LLR, operation time, amount of blood loss during the operation, blood transfusion, postoperative complications, length of postoperative hospital stay, and postoperative mortality. Postoperative pathological assessments included tumor size, tumor grade 3 or 4, encapsulation, microvascular invasion, portal vein tumor thrombosis (PVTT), satellite nodule, cirrhosis, and free resection margin from the tumor. Postoperative complications were classified according to the Clavien-Dindo grading system [12] and recorded for up to 90 days or during the same hospitalization in which the surgery was performed. When recurrent HCC was diagnosed, AFP and PIVKA-II level, initial recurrence sites, and initial treatment strategy in recurrent HCC were collected prospectively.
Definition
Group 1 was defined as patients who underwent LR from 1998 to 2015 (n = 68) and group 2 was defined as those who underwent LR between 2016 and 2020 (n = 62). The year 2016 was decided arbitrarily because both groups were divided into similar patient numbers. Postoperative pathology was reported based on guidelines from the Liver Cancer Study Group of Japan [13]. Tumor grades of HCC were assessed according to the Edmonson-Steiner grading system [14]. Minor LR was defined as the removal of 1 or 2 segments, while a major LR procedure was defined as the removal of 3 or more segments. Anatomical LR was defined as a case in which the area was resected after clamping the glissonian pedicle. The albumin-bilirubin (ALBI) score and AST to platelet ratio index (APRI) were calculated using the following formulas [1516]: ALBI score = −0.085 × (albumin, g/L) + 0.66 × log10(bilirubin, mmol/L) and APRI = [(AST/upper limit of normal)/platelet count, 109/L] × 100. The ALBI score was further stratified as follows: ALBI grade 1 (≤−2.60); grade 2 (>−2.60 and ≤ −1.39); or grade 3 (> −1.39). Postoperative complications were recorded for up to 30 days after LR or during the same hospitalization period in which the surgery was done. Death within 90 days of surgery was considered to be a case of perioperative mortality. Patient death was ascertained by linkage to the vital registration data provided by Statistics Korea, a central government organization for statistics, where all the deaths that occur in Korea are registered.
Surgical technique for LR
Surgical techniques of LR in our institution were described previously [171819]. The choice between LLR or open LR (OLR) depended on the preferences of individual patients and their surgeons. The selection criteria for choosing the laparoscopic approach were surgeon-dependent and are described in a previous study [10]. The indication of OLR included tumor size of greater than 10 cm, except when the tumor was of the pedunculated type; reconstruction of vascular or biliary conduit; proximity to an important vital structure that is deemed difficult to dissect laparoscopically; and invasion to adjacent organs necessitating concomitant resection and reconstruction. A flexible laparoscopic camera was used while maintaining the intraperitoneal pressure of 11 to 12 mmHg during LLR. A Cavitron ultrasonic surgical aspirator (Excel; Valleylab, Boulder, CO, USA) was used in OLR and different energy devices (Sonicison or Ligasure from Medtronic, Minneapolis, MN, USA; Harmonic Ace from Ethicon, Somerville, NJ, USA) were applied in LLR in accordance with the surgeon’s decision [20].
Perioperative management
Each patient received standardized pre- and postoperative management according to the routine manual [10]. The preoperative evaluation of elderly patients included echocardiography and pulmonary function tests. All patients received intravenous patient-controlled analgesia and additional analgesic drugs. The patient was continued on an oral diet from the first day after LR and was discharged once they were deemed free of complications.
Statistical analyses
Continuous variables were expressed as medians with ranges, and Mann-Whitney U analyses were used to identify differences between the 2 groups. Categorical variables are described as numbers and percentages of patients, and Fisher exact test was conducted to evaluate differences in the frequencies of categorical variables between the groups. The differences between disease-free survival (DFS) and overall survival (OS) rates between the 2 groups were assessed using the Kaplan-Meier survival method. The prognostic factors for HCC recurrence and death in univariate analysis were determined using a Cox-regression hazards model. Based on these results, variables with P < 0.05 were included in multivariate analyses. All of the statistical analyses were performed using the IBM SPSS Statistics ver. 22.0 (IBM Corp., Armonk, NY, USA) and P < 0.05 was considered to be statistically significant. All of the statistical tests were evaluated as 2-tailed.
RESULTS
Baseline characteristics
The basic demographics and preoperative characteristics of the 2 groups are summarized in Table 1. The median age of patients in both groups was 77 years (range, 75–84 years). The proportion of male patients and etiology in the 2 groups were not significantly different. The incidence of diabetes, hypertension, cardiovascular disease, cerebrovascular disease, lung disease, or previous abdominal operation in group 1 did not differ from those in group 2. There were also no statistically significant differences in complete blood count, liver function test results, international normalized ratio (INR), CRP level, and indocyanine green retention rate at 15 minutes, AFP, PIVKA-II, and APRI between the 2 groups. The median serum creatinine level in group 2 was lower than that in group 1 (0.87 ng/mL vs. 0.93 ng/mL, P = 0.042). The ALBI grade of group 2 was worse than that of group 1.
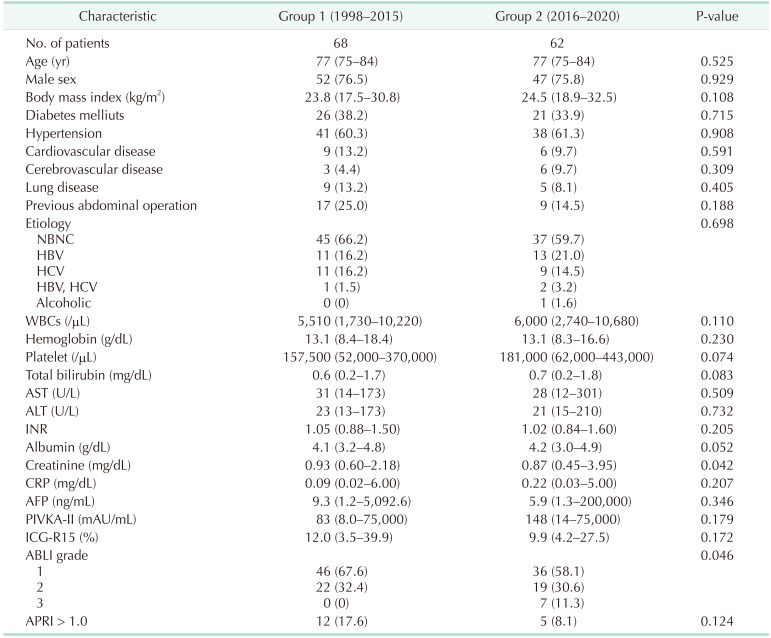
Table 1
Baseline characteristics
Values are presented as number only, median (range), or number (%).
NBNC, non B non C; INR, international normalized ratio; AFP, alpha-fetoprotein; PIVKA-II, proteins induced by vitamin K absence or antagonist-II; ICG-R15, indocyanine green at 15 minutes; ALBI, albumin-bilirubin; APRI, AST to platelet ratio index.
![]()
Perioperative and pathologic characteristics
The perioperative and pathologic characteristics of the 2 groups are outlined in Table 2. The proportion of major LR, anatomical LR, and LLR procedure performed in group 1 was significantly lower than those in group 2. Also, the median operation time was shorter and the amount of blood loss during LR was less in group 2 than in group 1. Rates of intraoperative RBC transfusion and postoperative complication, and median hospitalization length in group 2 were significantly lower than in group 1.
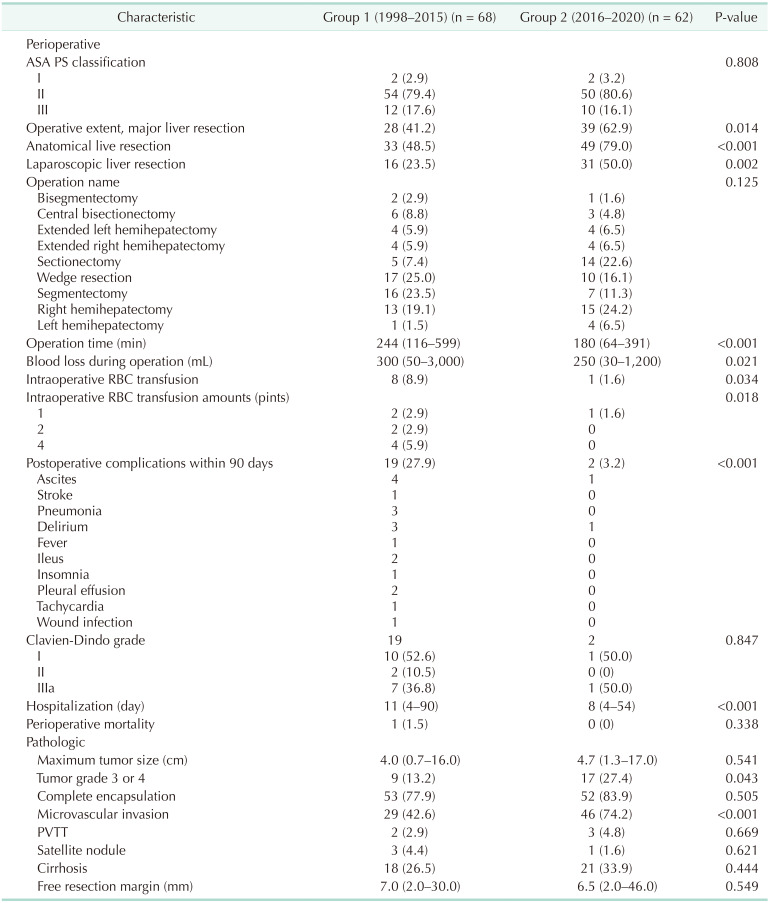
The presence of tumor grade 3 or 4 and the incidence of microvascular invasion in group 2 were higher than those in group 1. However, there were no statistically significant differences in the tumor size, encapsulation, PVTT, satellite nodule, cirrhosis, and free resection margin in tumors between the 2 groups.
Tumor recurrence and overall survival
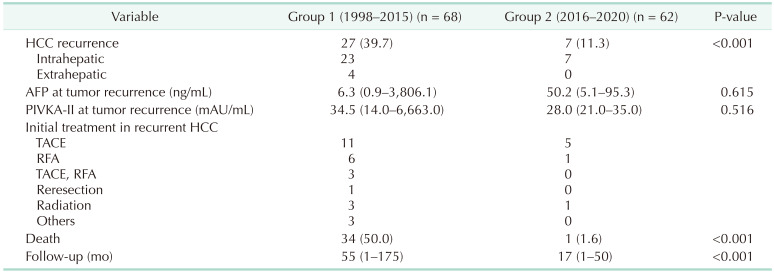
HCC recurrence is summarized in Table 3. The median follow-up period was 55 months (range, 1–175 months) for group 1 and 17 months (range, 1–50 months) for group 2 (P < 0.003). HCC recurrence was observed in 27 patients (39.7%) in group 1 and 7 patients (11.3%) in group 2 during the follow-up period, with initial recurrence sites including the liver (n = 23) and extrahepatic sites (n = 4) in group 1. The initial recurrent site in group 2 was intrahepatic in 7 patients. The cumulative DFS and OS rates at 1, 2, and 3 years were 83.9%, 65.2%, and 55.9% and 86.8%, 83.7%, and 74.2%, respectively, in group 1; and 89.5%, 82.8%, and 82.8% and 100%, 96.0%, and 96.0%, respectively, in group 2 (Fig. 1). The DFS and OS rates of group 2 were better than those of group 1 (P = 0.029 and P = 0.006, respectively).
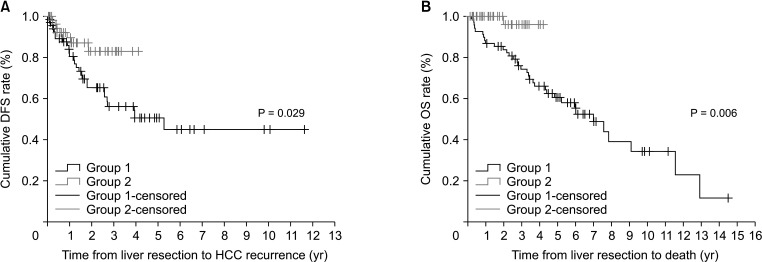
Fig. 1
(A) Disease-free survival (DFS) and (B) overall survival (OS) between group 1 and group 2. Group 1, the patients who underwent liver resection before 2016 (n = 68); group 2, the patients who underwent liver resection during or after 2016 (n = 62).
![]()
Univariate analysis showed that group 1 status, AST, ALT, INR, albumin, creatinine, APRI >1.0, AFP level of greater than 40 ng/mL, PIVKA-II levels of greater than 75 mAU/mL, and satellite nodules were strongly associated with HCC recurrence (Supplementary Table 1). An APRI value of greater than 1.0 and the presence of satellite nodules were predisposing factors for HCC recurrence in multivariate analysis (Table 4). Group 1 status, WBC count, AST, ALT, LLR, intraoperative RBC transfusion, long hospitalization length, and the presence of satellite nodules were strongly associated with patient death in univariate analysis (Supplementary Table 2). Finally, group 1 status, long hospitalization length, presence of satellite nodules, and increased intraoperative RBC transfusion rate were predisposing factors for patient death (Table 4).
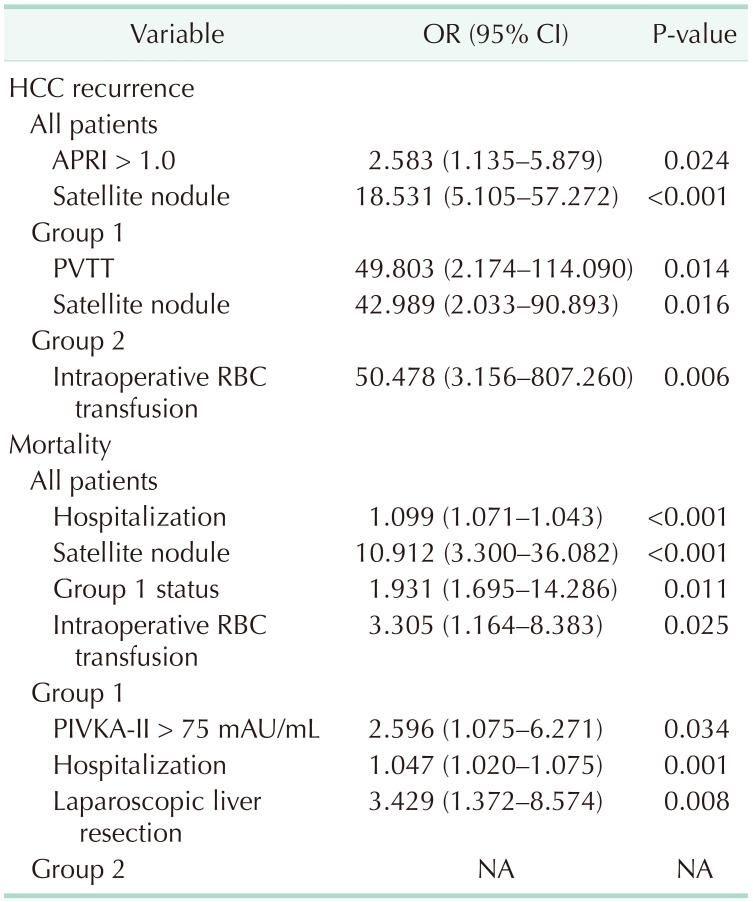
Table 4
Risk factors for hepatocellular carcinoma (HCC) recurrence and mortality in multivariate analyses
OR, odds ratio; CI, confidence interval; APRI, AST to platelet ratio index; PVTT, portal vein tumor thrombosis; PIVKA-II, proteins induced by vitamin K absence or antagonist-II; NA, not applicable.
Group 1, the patients who underwent liver resection before 2016 (n = 68); group 2, the patients who underwent liver resection during or after 2016 (n = 62).
![]()
We identified risk factors for HCC recurrence and mortality in group 1 and group 2, respectively (Supplementary Tables 3, 4). Multivariate analysis revealed that risk factors for HCC recurrence were PVTT and satellite nodule in group 1 and intraoperative RBC transfusion in group 2, respectively. In addition, high PIVKA-II, long hospitalization, and LLR group were predisposing factors for mortality in group 1. However, mortality events were very few in group 2, thus predisposing factors for mortality were not identified (Table 4).
DISCUSSION
As the incidence of HCC increases in elderly patients, the number of elderly patients being referred for surgery is also growing [1]. The definition of the elderly population has changed over time, thus categorizing elderly patients has been met with some challenges. Most developed countries accept the chronological age of 65 years as the definition of an elderly person, at which a person becomes eligible for statutory and occupational retirement pensions. However, recent review article regarding older age life expectancy, the World Health Organization defines older adults as those aged 60 years or older [6]. The government of Japan divides the elderly into 2 groups; The first elderly stage (<75 years) and the second elderly stage (≥75 years) [21]. According to the life expectancy data from South Korea, a 75-year-old man can expect to live an additional 10.8 years, and a 75-year-old woman can expect to live an additional 12.4 years [22]. Hence, it is likely for an elderly patient to have a life expectancy of an additional 10 or more years. Therefore, there is an urgent need to develop a new treatment strategy for elderly patients with HCC.
These patients present with lower functional reserves of the liver and increased comorbidities relative to younger patients. From 1998 to 2020, 130 patients older than 75 years old with treatment-naïve solitary HCC underwent LR. Based on 2015, which is the median year of the time of surgery among the 130 patients, we compared the characteristics and outcomes at time-dependent differences and surgical approach.
Although there was no difference in preoperative baseline characteristics between the 2 groups, the frequency of major LR and LLR was greater in group 2, while the operation time, amount of blood loss during operation, and intraoperative RBC transfusion rate were significantly lower. Because of this difference, the postoperative complications and hospital stay in group 2 were significantly lower than in group 1. Although HCC-related factors of grade 3 or 4 and microvascular invasion were higher in group 2, DFS and OS rates in group 2 were significantly better than in group 1. In the subgroup analysis of group 1, high PIVKA-II, long hospitalization, and laparoscopic LR were closely associated with mortality. In the subgroup analysis of group 2, however, none of the factors increased mortality. This difference is thought to be attributed to improved surgical technique, shortened hospitalization and quicker recovery period due to laparoscopic LR, and increased anatomical LR. Accordingly, group 2 did not demonstrate a relationship with HCC recurrence in multivariate analysis, but it appears to be an important predisposing factor in OS.
Elderly patients are considered fragile due to their comorbidities, and they are believed to be more vulnerable to the complications of surgical treatment. Therefore, there is a tendency to choose locoregional therapies rather than surgical treatment and supportive care rather than active treatments for elderly patients with HCC, which may contribute to their increased mortality relative to younger patients. Notably, however, there was just one case of 90-day postoperative mortality in our elderly study population. Previous studies have reported that LR in the elderly contributes to a very high mortality rate of 3.5% to 5.6% [23]. Although more minor LR and non-anatomical LR were performed in group 1 relative to in group 2, the rate of postoperative complications was remarkably high (27.5% in group 1 vs. 3.2% in group 2, P < 0.001). Over time, there was no change in the standard of surgery or postoperative care in our institution and LLR was performed more actively.
The role of LLR techniques is to reduce the amount of surgical trauma and the degree of physiological disruption to patients. There have been numerous publications detailing the short-term benefits of LLR when applied to a general population [10182324]. Previous studies have reported an association between operative time and postoperative morbidity in LLR [25]. Laparoscopic surgery is a more complex and time-consuming approach than the conventional open approach, but our team has sufficient experience and advanced skill for LLR, so surgical operation time has ceased to be an obstacle in the spread of the procedure in our hospital [26]. The elderly population represents a unique surgical challenge because of the associated complex comorbidity and diminished cardiopulmonary reserve. With current advances in anesthesiology, surgical techniques, and better knowledge of disease pathology, the perioperative morbidity and mortality risk associated with hepatic resection in HCC patients has been reduced significantly with five-year survival rates being as high as 50% [27].
Satellite nodules are known as important factors for patient prognosis after curative LR. Our study also revealed that satellite nodules are predisposing factors for HCC recurrence and patient death. Preoperative assessment of the hepatic functional reserve is important to individualize treatment strategies for HCC. APRI is a noninvasive scoring system for chronic liver disease that is known to be effective at assessing liver fibrosis and cirrhosis [28]. The incidence of HCC recurrence remains high after curative LR [2930]. Liver fibrosis is an important risk factor for multicentric carcinogenesis [31]. High APRI is closely correlated with HCC recurrence in elderly patients, yet APRI did not correlate with death.
LR is associated with a high risk of bleeding and perioperative blood transfusion, which can be related to mortality rate and long-term survival [32]. Previous studies reported that 25.2% to 56.8% of patients received an RBC transfusion [3334]. The intraoperative RBC transfusion rate in our study was 8.9% in group 1 and 1.6% in group 2. Suboptimal LR, inadequate division plane, and injury to the major vessels may cause blood loss during surgical procedures. These complications can lead to severe sequelae, such as hepatic failure after surgery because of decreased tissue perfusion and oxygenation [151635]. In addition, RBC transfusion may have immunomodulatory and proinflammatory effects [3436]. As surgical techniques improved in our team, blood loss, transfusion rate, and operation time decreased. The HCC guidelines in Korea stated that blood transfusion compromises anticancer immunologic mechanisms and increases postoperative recurrence [37]. Therefore, surgeons should reduce blood loss during hepatectomy and avoid perioperative RBC transfusion.
Our study also demonstrated that intraoperative RBC transfusion and long hospitalization were predisposing factors for patient death. Longer operative times are related to greater rates of intraoperative RBC transfusion [34]. Our study revealed that patients who received intraoperative RBC transfusions had longer operation times and worse liver function in the postoperative period. The limited functional reserves and lower recovery capacity of elderly patients may extend their hospital stays.
Several limitations in this study must be considered, including all the limitations inherent to a retrospective analysis. Selection bias may occur in our patient population because the population that received non-surgical treatment is missing—that is, hepatectomy patients with good performance status and preserved liver function. The comparison of outcomes between groups 1 and 2 was likely to be affected by some degree of selection bias because of similar tumor characteristics and liver function in the 2 groups. Second, it is not statistically appropriate to compare 2 consecutive periods. The surgical skills of our surgeons improved through the accumulation of experience.
In conclusion, LR in elderly HCC patients has been frequently performed recently, and the outcomes have improved significantly compared to the past. It is believed that DFS and OS were improved by decreased operation time, amounts of blood loss during LR, and intraoperative RBC transfusion rates in patients over 75 years of age who underwent recent surgery, but more detailed studies are needed in the future.
 XML Download
XML Download